
Abstract
Abstract
Background:
Hospital-based palliative care consultative teams assist with decision-making, symptom management, patient and family support, and discharge planning for those with advanced illness. However, there is evidence to suggest that many patients dying within acute hospitals receive no specialist palliative care input. This project aimed to assess care provided to patients dying within a large Australian hospital and to understand senior clinician decision-making around referral to palliative care.
Methods:
A multi-methods approach was taken that incorporated a literature review, a retrospective chart-audit using the Liverpool Care Pathway to assess quality of end-of-life care, and semistructured interviews with clinicians.
Results:
The audit demonstrated wide variation in referral practices from clinical units, with overall only 42% of dying patients referred. A number of deficiencies in the care of dying patients within the hospital were evident; however, referral for palliative care consultation was associated with improvements in availability of appropriate end-of-life medication orders, communication with patients and families, and cessation of futile treatment and interventions. Eight themes emerged from the interviews with clinicians, including uncertainty as to the role of palliative care and a discrepancy between medical and nursing views of the utility and timing for palliative care.
Conclusions:
The findings demonstrate both the need for more frequent and/or earlier referral of dying patients and the need for generalist staff to become more skilled in the delivery of palliative care. It also highlights the need for palliative care clinicians to be educators and advocates within services to enhance care at end-of-life.
Introduction
Despite the intention of many palliative care services to enable patients to die in the environment of their own choosing, recent studies have shown that 55% to 78% of adults in Western societies continue to die within hospitals or institutions.8–10 Whilst end-of-life care and management of terminal symptoms is well accepted by most health care professionals as a key task of any palliative care service, 6 it has been shown that many patients who die in tertiary hospitals do not receive management advice from palliative care services. A recent study conducted in the United States looked at 1222 deaths occurring in a tertiary hospital over a 1-year period. 11 In that study, palliative care was only involved in 20% of patients who died in a hospital. 11
The Royal Melbourne Hospital (RMH) has the largest number of admissions and separations of any hospital in Australia and serves as a state-wide referral center for specialist care in areas such as neurosciences, trauma, and nephrology. The established RMH palliative care consultancy service receives referrals from all departments within the hospital, with one-third of all referrals being for management advice of patients at end-of-life. As with other centers, the majority of patients who die at the RMH do not receive management advice from the palliative care service. An audit conducted at the RMH in 2005 showed that despite 75% of deaths occurring in the hospital being anticipated by clinicians, fewer than 38% of these patients were referred to the palliative care service. 12
The available data suggest that improvements in the care of the dying and the underutilization of palliative care services remain issues to be addressed. 13 Henceforth, this quality improvement project was undertaken at the RMH during 2007–2008 with the aim of assessing care provided to patients dying within our hospital and understanding senior clinician decision-making around referral to palliative care.
Methodology
A multi-methods approach was used and incorporated a literature review, chart audit, and interviews. The project was assessed by the hospital research ethics committee chair as being a quality improvement project.
Audit
A retrospective audit of 3 months of sequential hospital deaths during 2007 (n = 190) using the Liverpool Care Pathway (LCP) baseline audit tool 14 was undertaken. This audit tool assesses the quality of care provided to dying patients; however, it only captures care that has been documented in the patient's chart. The goals of care assessed are divided into domains that relate to comfort measures, psychological and insight issues, religious needs, communication with family and primary health-care team, ongoing assessments, and care after death.
Interviews
Semistructured interviews were conducted with 27 RMH clinicians to collect data regarding their understanding of palliative care and how decisions were made around referral to the service. A purposive sample of participants was selected, the aim being to capture senior clinicians from most departments and disciplines, who were assumed to be most influential in the decision-making process and the “palliative care culture” in units around the hospital. Interviews were transcribed verbatim and then subjected to thematic analysis. We approached the data with an open mind and attempted to identify important themes emerging from the data.15,16
Results
Audit
The purpose of the audit was to determine the quality of care for patients dying in the hospital. The audit captured three consecutive months of patient deaths occurring in 2007 at RMH. Of 190 deaths, 171 records were successfully accessed and included in the final audit. The audit included 89 men (52%) and 82 women (48%). The mean age was 76 years (range 27–100 years), and the mean length of final hospital admission was 12 days.
Forty-four patients (26%) died under the care of a general medical unit, 35 patients (20%) under the stroke unit, 16 patients (9%) under neurosurgery, 14 patients (8%) under aged care, 12 patients (7%) under medical oncology, and the remaining 50 patients (30%) under a wide variety of other specialty units. In terms of location at the time of death, 46 patients (27%) died on a general medical ward, 33 (19%) in the intensive care unit, 32 (19%) on the neurology ward, 17 (10%) in the emergency department, and 13 (8%) on the medical oncology/hematology ward.
One hundred sixteen deaths (68%) were anticipated and 49 (29%) were not anticipated; chart review was unclear for nine (3%). Deaths were interpreted as anticipated if the chart indicated that there would have been time to make a referral to the palliative care service; i.e., the patient's deterioration occurred over a period of greater than 24 hours. Of the anticipated deaths, only 49 (42%) were referred to the palliative care service, with the remaining 67 (58%) not referred.
As shown in Fig. 1, individual units varied in their referral practices of dying patients to palliative care. Medical oncology referred 11 of 12 (92%) patients who died, the stroke unit referred 20 of 35 (57%) patients, aged care referred 6 of 14 (43%) patients, hematology referred three of four (75%) of patients, and general medicine referred 29 of 44 (66%) patients. Neurosurgery referred 4 of 16 (25%) patients, respiratory referred none of three (0%) patients, and cardiology referred none of six (0%) patients. Selected audit results using the LCP baseline audit tool are shown in Table 1.
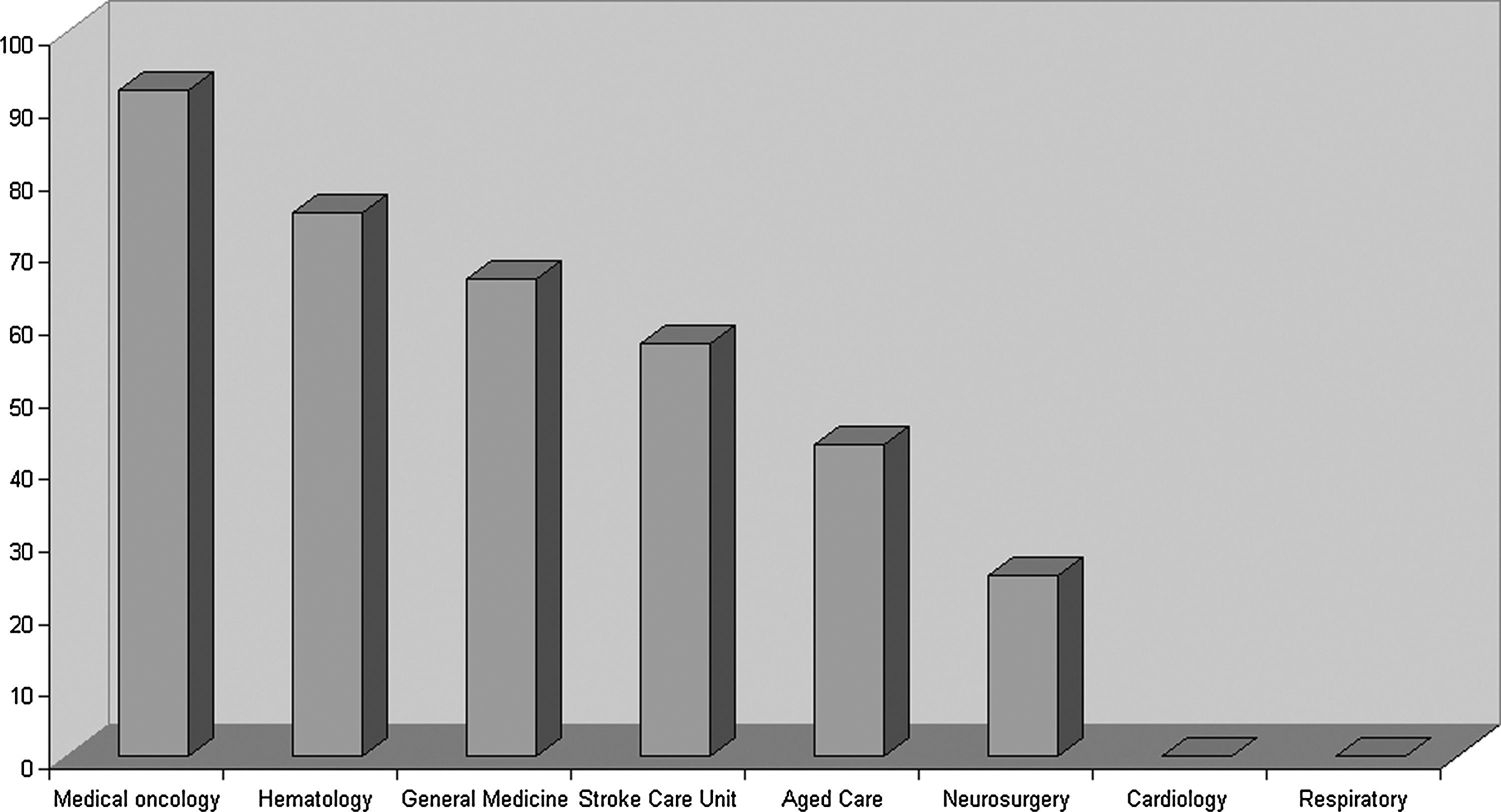
Percentage of patients referred for palliative care consultation prior to death according to parent unit.
Sixty-five percent of nonreferred patients had a subcutaneous analgesic prescribed, whereas 96% of referred patients had these prescribed. Anticholinergics, antiemetics, and sedatives were all more likely to be ordered for patients receiving palliative care consultation. Only 44% of nonreferred patients had their medications assessed with nonessential prescriptions discontinued. This increased to 90% for those patients reviewed by the palliative care service. Nonreferred patients were also subjected to higher levels of possibly futile intervention (monitoring of blood tests and vital signs, antibiotics, and intravenous fluids).
Although it was rarely documented that patients were aware of their terminal diagnosis, nonreferred patients' relatives were aware the patient was dying in 66% of cases. This increased to 91% with involvement of the palliative care team. Pain and agitation were assessed as being a problem in 31% of nonreferred dying patients but 74% of the referred patients were assessed as having pain and 69% as being agitated. Some basic areas of nursing care were deficient; for example, only 57% of nonreferred patients had documentation showing that mouth care was completed every 4 hours, rising to 89% for patients who received palliative care consultation.
Communication with general practitioners (GPs) was recorded infrequently for referred and nonreferred patients. Documentation across the board was poor regarding the assessment of religious and spiritual needs, which only occurred in 14% of patients referred to the palliative care team.
Interviews
Of the 34 staff contacted via e-mail, 27 responded and were interviewed (84%). Included were nurse unit managers (NUMs) and clinical nurse consultants (n = 10), senior medical staff (n = 11), social workers (n = 2), pastoral care staff (n = 2), speech pathologists (n = 1), and occupational therapists (n = 1). Only three staff reported previously working in palliative care. Staff from 15 departments were represented: medical oncology, clinical hematology, aged care, anesthetics/pain service, general medicine, respiratory medicine, cardiology, neurosurgery, renal, neurology, infectious diseases, general surgery, trauma, intensive care, and head and neck surgery (Table 2).
Analysis of the interview transcripts revealed the following eight themes:
Introducing palliative care and the language of palliative care Providing information and meeting with families Giving support and confidence to staff • Managing without palliative care Clarifying goals of care Providing continuity of care Knowing when to refer Suggesting referrals—nursing and allied health
Themes are explored and illustrated using key excerpts from the transcripts.
Introducing palliative care and the language of palliative care
The use of the term “palliative care” and talking about palliative care to patients came up frequently with many of the respondents and seemed to generate a degree of anxiety or concern for non–palliative care clinicians. Having conversations with patients and finding the right words were seen as a particular skill of the palliative care team.
I think there's a lot of anxiety for anybody when someone's dying about how to word that correctly … (social worker).
Providing information and meeting with families
Linked with issues around language was the perception that the palliative care team was effective at addressing the informational needs for patients and their families.
I think their questions get answered faster, they get answered a lot quicker. I think they ask certain types of questions that I don't know would've come out if the palliative care team hadn't been involved (NUM).
This ability to provide information about the disease and treatment was seen as psychologically beneficial in allowing patients to move towards acceptance of their diagnosis and being prepared for the future.
… the family members are a lot more accepting I find when palliative care is involved because they're aware that this is what's going to happen and they're better prepared for it (NUM).
Giving support and confidence to staff
Making decisions about providing palliative care for patients was seen as a difficult and burdensome part of non–palliative care clinicians' work.
I think that's one of the reasons why doctors avoid thinking about it because I think it weighs very heavily on your mind as to, well how do you know, how can you be so certain that this is it (Physician).
However, the palliative care team was seen as having an important role in supporting other teams to do their work and absorbing some of the stress.
… I think that there's a lot of anxiety for anybody when someone's dying … and I think that in my experience palliative care are very good at helping staff to manage that situation, whether it's helping junior medical staff knowing how to language it well for families and patients, or whether it's helping staff to manage their own anxiety about how much to be doing or not doing in different situations (social worker).
Managing without palliative care
The role of the palliative care team in supporting staff was widely reported from nursing and allied health staff. However, medical staff reported higher levels of autonomy and confidence when it came to providing palliative care without the involvement of the palliative care team.
… but the medical decision was no, we don't need palliative care, we'll sort it out ourselves (social worker).
In some instances teams felt the need to protect patients from the palliative care team.
… so some people find it too confrontational … they don't want to know about it … so sometimes we will try and do our own sort of palliation … (physician).
Clarifying goals of care
The transition from acute to palliative care was seen by the respondents as a difficult phase in the patient's care. However, palliative care team members were seen as being helpful in reducing the ambiguity, especially for staff, during this time.
But I think also just having staff who are experienced in dealing with death and dying issues both for the patient to help them move into a palliative care mode rather than an active treatment mode. But also for their family and friends as well, assisting them moving in that direction as well, that takes considerable skill and time and purpose to do that (NUM).
Some clinicians acknowledged that making the shift to palliative care and “letting go” was difficult.
It's very difficult to let go as well as a clinician and to be clear headed about it (physician).
Providing continuity of care
A major reason why teams referred to palliative care was to access community support and to provide some continuity of care as people moved in and out of the hospital system. This aspect of care was seen as very important, especially by medical staff, and a key role of palliative care services.
… management of symptoms, management of environment, transition of care, upgrading from home to hospice at the appropriate time, and also after hours access to assistance … (physician).
Knowing when to refer
Respondents varied in their opinions about when referral should be made to palliative care. The majority advocated for early referral.
I think as early as practical as possible … We've felt our patients don't have access to palliative care when they should do … (social worker).
… involvement of some specialist expertise in palliation at an early phase would be helpful … (surgeon).
… the appropriate time for consultation is when it is clear that symptom control either is, or is going to become, too complex to manage … (physician).
But I think people need to be dying, really, I think things need to be on a fairly terminal path … (physician).
Some nursing respondents indicated that in reality referrals to palliative care occurred too late.
As nurses we're with the patient, around them all the time, the patient requesting that they want treatment withdrawn and they want to die … and that not being really picked up by the medical staff or they're not willing to concede to that sort of point at that time (NUM).
Suggesting referrals—Nursing and allied health
Most believed the decision to refer to palliative care was made as a team at a multidisciplinary meeting or on ward rounds. For many it was also a decision made by a registrar or consultant. However, what emerged strongly was the role that nurses and allied health team members played in early identification of palliative care needs and in suggesting that a palliative care referral be made.
I just raise it as another option, you know, has this been thought about, that's what I try to do to get it on the agenda … often it's the first time that someone's ever thought of that … (NUM).
Reasons why suggestions were not taken up varied but seemed to include concerns about lack of experience or seniority, and difficulty in making the decision itself.
… the interns are young and they don't have a lot of experience, so they'll take it away and perhaps discuss it further but it seems to be not something they've thought of before and they're anxious that, you know, they're writing off the patient now and they've still got months to go (NUM).
Discussion
The audit confirmed that the majority of dying patients in the hospital were not referred to palliative care, with concerning evidence found for deficiencies in quality of care for patients dying in the hospital. The audit also showed that referral to the palliative care service resulted in key improvements in the care of dying patients, including implementation of appropriate end-of-life medication orders, cessation of futile treatment and interventions, and improved communication with families. Referral patterns around the hospital varied enormously with traditional referrers like medical oncology still referring nearly all their dying patients to the palliative care service. Areas such as the stroke unit, general medicine, and aged care were frequent referrers but appeared to manage large numbers of dying patients without referral. Cardiology and respiratory medicine teams rarely referred. These findings were consistent with the literature and reflect the well-described barriers to referral of patients without a malignant diagnosis to palliative care.17,18
The higher prevalence of symptoms such as pain and agitation in referred patients may reflect that teams refer patients with these symptoms more readily or that the palliative care service encourages and engages in more astute assessment of symptoms. The high levels of medical intervention up to the point of death may be partially attributed to the relatively large number of emergency department and ICU deaths (27% combined) for whom high levels of monitoring and intervention are possibly the expected norm. Deficiencies in core palliative care tasks in nonreferred patients such as mouth care is cause for concern, as was the lack of communication with GPs and the assessment of religious and spiritual needs for both referred and nonreferred patients, mirroring the findings of other studies. 10
The interview process provided a unique understanding about how palliative care was perceived by a wide variety of staff from around the hospital. Information was gained about how clinicians make referral decisions. These findings have given a basis from which to generate educational materials, and how to profile and sell the palliative care team. Key points are summarized in Table 3.
Conclusions
This quality improvement project was aimed at improving knowledge of, and access to, specialist palliative care at the RMH. The audit demonstrated that referral behaviors around the hospital varied enormously, as did the quality of end-of-life care received by dying patients. Referral to the palliative care service was shown to have a positive impact on a range of quality of care measures at end-of-life. These findings demonstrate both the need for more frequent and/or earlier referral of dying patients and the need for generalist staff to become more skilled in the delivery of palliative care. The interview data has emphasized the important role that the palliative care service provides around the hospital in decision-making, the care of patients' family members, and support of staff. Furthermore, this data shows why decisions for referral may be delayed and the challenges that exist when clinicians are faced with introducing a palliative approach. The project findings have provided insights into how palliative care education and the development of referral guidelines can be effectively approached. The interview process per se also raised the profile of palliative care around the hospital, with many staff using the opportunity to ask questions and learn more about the service.
Footnotes
Acknowledgments
The authors would like to thank Ms. Jackie Kearney and Mr. Gregory Dalton, of the Cancer and Palliative Care Unit, Victorian Department of Health for providing the support and funding to make this project possible. The authors would also like to thank the staff who volunteered their time to be interviewed.
Author Disclosure Statement
The authors of this work have no actual or potential competing financial interests, nor conflicts of interest to declare.