
Abstract
Abstract
Purpose:
In February 2002, the palliative care team was established in Ikeda Municipal Hospital to improve palliative care. We investigated changes in the incidences of side effects related to opioids, and evaluated palliative care team activities.
Methods:
Regarding inpatients for whom narcotics were prescribed in our hospital in the years of 2002 (from October 1, 2002 until September 30, 2003), 2004 (from October 1, 2004 until September 30, 2005), and 2006 (from October 1, 2006 until September 30, 2007), we surveyed the rates at which laxatives or antiemetics were prescribed, frequency of defecation/its state before and after the start of narcotic therapy, frequency of nausea/vomiting, and dietary intake.
Results:
The proportions of patients in whom laxatives were simultaneously prescribed during opioid therapy in 2002, 2004, and 2006 were 43.5%, 78.7%, and 75.6%, respectively. The proportions of those in whom antiemetics were combined with opioids were 45.7%, 78.7%, and 78.0%, respectively. The incidences of constipation were 50.0%, 39.3%, and 37.8%, respectively. Those of nausea/vomiting were 30.4%, 21.3%, and 9.8%, respectively. Those of anorexia were 65.3%, 39.4%, and 15.4%, respectively.
Conclusions:
These results suggest that palliative care team activities facilitated appropriate drug prescription during opioid therapy, reducing the appearance of side effects, with likelihood of improved quality of life.
Introduction
In our hospital, Ikeda Municipal Hospital, the palliative care team, consisting of physicians, pharmacists, and nurses was established in February 2002 to improve palliative care. There is no social worker or chaplain on our palliative care team, as is the case for many palliative care teams in Japan. This team has designed the usage of agents for pain/adjuvant analgesic agents and strategies to reduce the side effects of opioids based on the World Health Organization (WHO) system.2,3 It was recommended that laxatives and antiemetics should be combined with opioids from the start of opioid therapy to prevent constipation and nausea/vomiting, respectively. Strategies to prevent opioid therapy-related side effects have been conducted. 4 In this study, we investigated changes in the incidences of opioid-related side effects after the start of palliative care team activities and evaluated the activities.
Methods
Survey subjects and period
The subjects were inpatients for whom narcotics were prescribed in our hospital in 2002 (from October 1, 2002 until September 30, 2003), 2004 (from October 1, 2004 until September 30, 2005), and 2006 (from October 1, 2006 until September 30, 2007). However, we excluded patients treated with narcotic injection and those in whom the survey interval before and after the start of narcotic therapy was less than 3 days. We also excluded patients who received cancer chemotherapy during the survey period.
Evaluation of opioid-related side effects
As background factors, we surveyed the number of patients, male-to-female ratio, mean age, proportion of patients with digestive cancer, department, type of opioid, and rates at which laxatives or antiemetics were prescribed. Concerning the state of side effects, we investigated the frequency of defecation/its state, frequency of nausea/vomiting, and dietary intake based on charts for 7 days each before and after the start of narcotic therapy (when the survey interval was less than 7 days, it was established as 3 days or more each before and after the start of narcotic therapy). Each parameter was evaluated using the following methods.
Constipation
When the ratio of the number of defecation-free days to the survey interval (number of defecation-free days/survey interval) was 0.5 or more, or when laxatives were administered if necessary, constipation was regarded as (+). In other cases, it was regarded as (−). Among patients with constipation (+) before the start of narcotic therapy, it was evaluated as (++ ) in those in whom the ratio of the number of defecation-free days became 0.5 or more after its start, and in those in whom the management of severe constipation (stool evulsion, glycerin enema) was conducted. In patients who showed a change from (−) to (+) or from (+) to (++ ) after the start of narcotic therapy, the influence of opioids was regarded as present. In others, it was regarded as absent.
Nausea/vomiting
When the ratio of the number of days with a complaint of nausea to the survey interval (number of days with a complaint of nausea/survey interval) was 0.5 or more, or when vomiting was noted at least once during the survey period, nausea/vomiting were regarded as (+). In other cases, they were regarded as (−). Among patients with nausea/vomiting (+) before the start of narcotic therapy, they were evaluated as (++ ) in those in whom the frequency of vomiting or ratio of the number of days with a complaint of nausea increased after its start. In patients who showed a change from (−) to (+) or from (+) to (++ ) after the start of narcotic therapy, the influence of opioids was regarded as present. In others, it was regarded as absent.
Anorexia
We calculated the means of dietary intake (total daily intake: 10) before and after the start of narcotic therapy. We also calculated the ratio of postnarcotic to prenarcotic therapy dietary intake (postnarcotic/prenarcotic therapy dietary intake). When the ratio was 1.3 or more, dietary intake was regarded as being increased. When it ranged from 0.7 to 1.2, intake was regarded as showing no change. When it ranged from 0.3 to 0.6, intake was regarded as being decreased. When it was less than 0.3, intake was regarded as being markedly decreased.
Statistical analysis
Statistical analyses of the data were performed by the chi-square and Kruskal-Wallis tests using SPSS (SPSS Inc, Chicago, IL). p < 0.05 was regarded as significant.
Results
Background of patients receiving opioid preparations
There were no significant differences in the male-to-female ratio, mean age, proportion of patients with digestive cancer, nor department among the three groups. We compared components of opioid preparations. The proportion of patients receiving morphine sulfate gradually decreased, and that of patients receiving oxycodone hydrochloride increased. Furthermore, that of patients receiving fentanyl also slightly increased (Table 1).
Chi-square test.
Kruskal-Wallis test.
Laxatives were simultaneously prescribed during opioid therapy in 43.5% of the patients in 2002. In 2004, the percentage was 78.7%, showing a significant increase (p < 0.01). In 2006, it was 75.6%, showing no change. Antiemetics were simultaneously prescribed during opioid therapy in 45.7% of the patients in 2002. In 2004, the percentage was 78.7%, showing a significant increase (p < 0.01). In 2006, it was 78.0%, showing no change (Fig. 1).
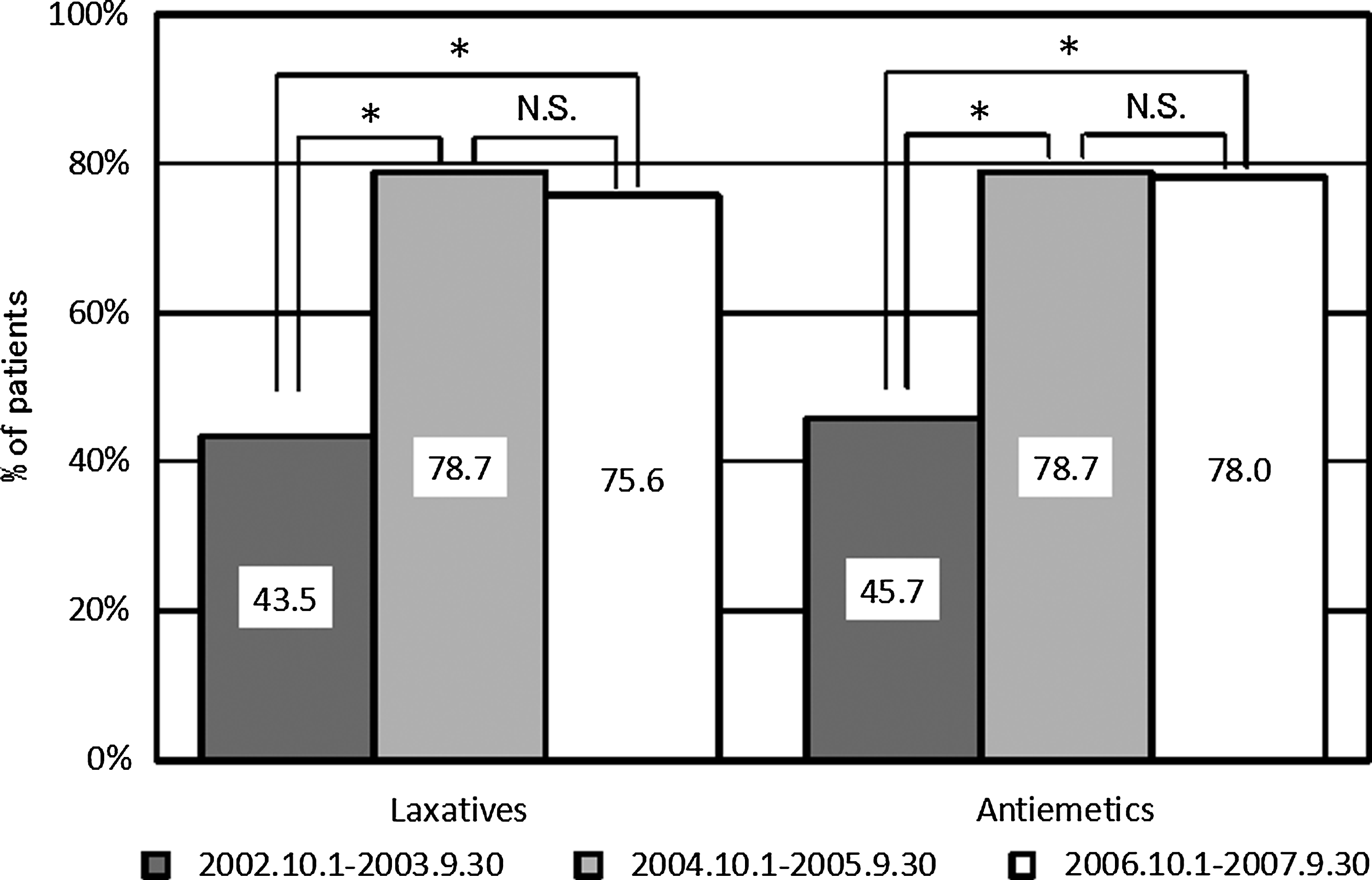
Percentage of patients prescribed laxatives and antiemetics after the beginning of opioid use. Each survey period was 1 year: October 1, 2002 to September 30, 2003; October 1, 2004 to September 20, 2005; and October 1, 2006 to September 30, 2007. *p < 0.01 by χ2 test. NS, not significant.
Incidences of side effects
The number of patients with opioid therapy-related development/deterioration of constipation [(−) → (+) or (+) → (++ )] in 2002 and 2004 were 50.0% and 39.3%, respectively, showing a decrease, although there was no significant difference. However, in 2006, the incidence was 37.8%, showing no change. Furthermore, the number of patients with opioid therapy-related development/deterioration of nausea/vomiting [(−) → (+) or (+) → (++ )] in 2002 and 2004 were 30.4% and 21.3%, respectively. In 2006, the percentage was decreased to 9.8% (Table 2, Fig. 2).
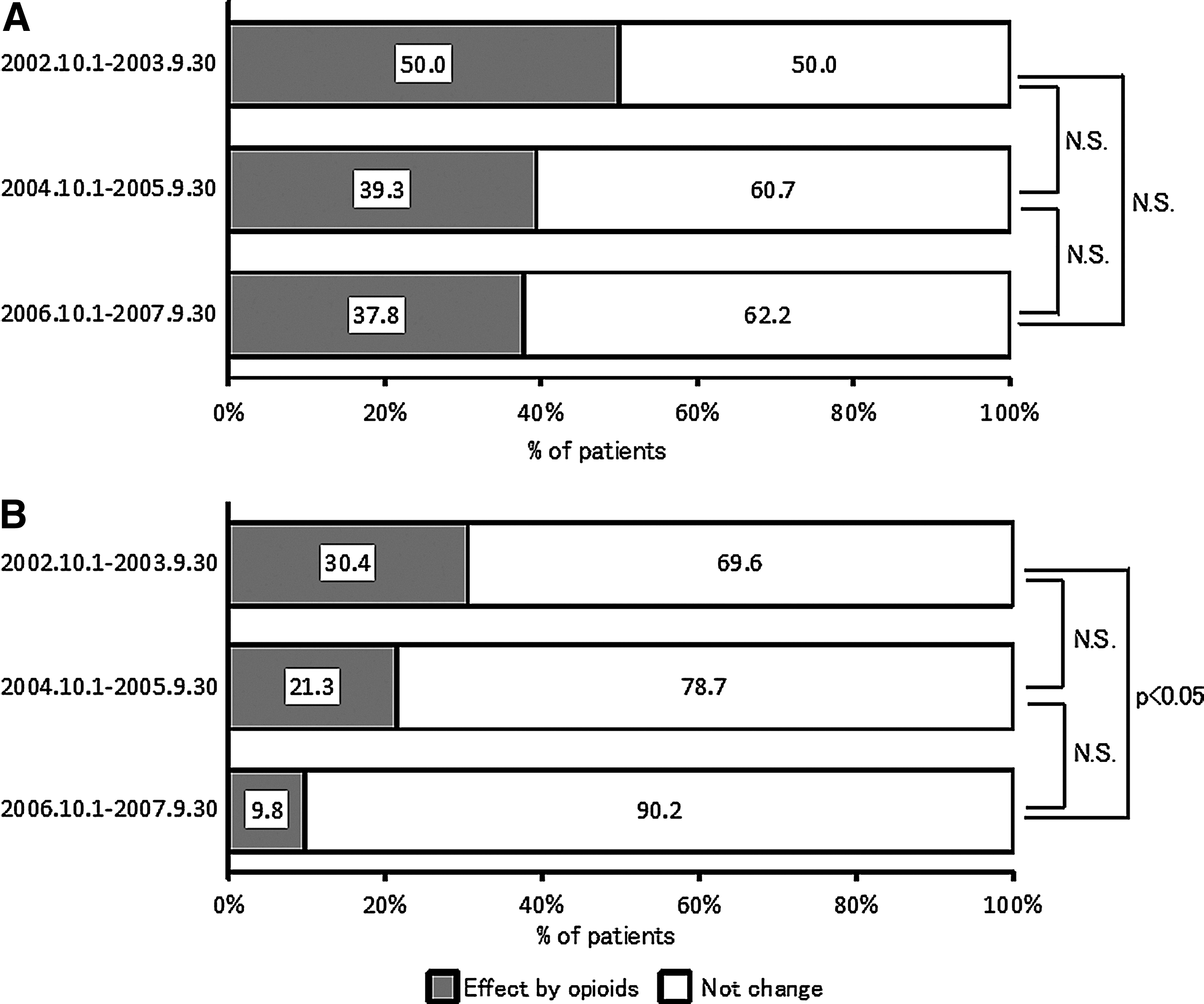
Percentages of patients influenced by opioids. Effect by opioids: symptoms of constipation (
Before: Immediately before the beginning of opioid usage. After: After the beginning of opioid usage. (−): Not having constipation or nausea/vomiting. (+): Having constipation or nausea/vomiting. (++ ): Their symptoms got worse. Effect by opioid: Each symptom caused or got worse after opioid usage. The each survey period was 1 year from October 1, 2002 to September 30, 2003, from October 1, 2004 to September 30, 2005 and from October 1, 2006 to September 30, 2007.
The percentage of patients showing an opioid therapy-related reduction in food intake to less than 70% in 2002, 2004, and 2006 were 65.35, 39.4%, and 15.4%, respectively, showing a significant decrease. The percentage of patients showing an opioid therapy-related reduction in food intake to less than 30% were 37.0%, 16.4%, and 2.6%, respectively, revealing a marked decrease (Fig. 3).

Percentages of patients classified by change of appetite before and after opiod use. Patients were classified by the ratio of food intake after/before beginning opioid use. Remarkable down: 0–0.3; down: 0.3–0.7; no change: 0.71.3; up: >1.3. Each survey period was 1 year: October 1, 2002 to September 30, 2003; October 1, 2004 to September 20, 2005; and October 1, 2006 to September 30, 2007. *p < 0.05 **p < 0.01 by χ2 test. NS, not significant.
Discussion
Opioids play a primary role in cancer pain treatment. In Japan, the amount of prescribed opioids has also increased year by year with the widespread use of cancer pain strategies. 5 However, in many cases, it is impossible to avoid the appearance of side effects even at a dose necessary for pain relief; therefore, it is difficult to continue administration without close strategies to reduce side effects. 6 Furthermore, the preventive management of frequent side effects is necessary rather than management after their appearance. 7 The palliative care team in our hospital also recommended that laxatives and antiemetics should be combined for opioid therapy. The rates at which these agents were prescribed have gradually increased. 4 In this study, we investigated changes in the incidences of opioid-induced constipation, nausea/vomiting, and anorexia after this team was established, and evaluated the influence of palliative care team activities on the incidences of side effects.
Concerning the patient background, there were no marked differences in the items other than the type of opioid among the groups. In 2002, morphine sulfate was administered to most patients. However, the proportion of patients receiving oxycodone hydrochloride markedly increased in 2004 and 2006. In Japan, a sustained-release oxycodone hydrochloride preparation became commercially available in 2003, and was used in our hospital. In our palliative care manual, it was recommended that a low-dose oxycodone hydrochloride preparation should be selected as a first-choice agent at the start of opioid therapy. This possibly contributed to the marked increase in the proportion of patients receiving oxycodone hydrochloride. Furthermore, the number of prescriptions regarding fentanyl was small because of the restricted use of fentanyl patches (a switch from other opioid preparations) in Japan.
The most frequent side effect of opioids is constipation. A study reported that constipation was noted in 82% of patients treated with morphine sulfate. 8 Opioids inhibit peristalsis via continued tension of the digestive tract smooth muscle, causing constipation. A laxative protocol is almost always necessary to overcome constipation as long as opioids are needed for pain. The results of this study showed that the number of patients with opioid therapy-related development/deterioration of constipation in 2004 was smaller than in 2002, although there was no significant difference. There is no special laxative to relieve opioid-induced constipation. 9 Osmotic or stimulant laxatives are mainly used. In our hospital, magnesium oxide is simultaneously prescribed for opioid therapy. When it is impossible to prevent constipation despite this combination therapy, or in patients receiving magnesium oxide, sennoside or sodium picosulfate is additionally administered. These agents are selected because combination therapy with agents exhibiting different actions may be more effective than the administration of several agents showing the same actions. 6 It may also be necessary to select a laxative and regulate the dose based on the patient's defecation status, for regular bowel opening.
The incidence of nausea in patients with terminal cancer ranges from 40% to 70%. Nausea control is important.10,11 In particular, opioid-related nausea occurs in approximately one third of all opioid-treated patients.11,12 Based on these findings, antiemetics should also be prophylactically administered. 13 In this survey, the number of patients with opioid therapy-related development/deterioration of nausea/vomiting decreased annually. Opioid administration-related nausea/vomiting develop via the following central mechanism: opioids directly stimulate dopamine D2 receptors in the chemoreceptor trigger zone (CTZ) of the medulla oblongata, transmitting the stimulation to the vomiting center. 10 Therefore, in our hospital, a dopamine D2 receptor blocker, prochlorperazine maleate (tablets), is combined with narcotics. However, when refractory/intolerance-related nausea develops despite the administration of antiemetics at a sufficient dose, opioid rotation may reduce the symptom. 14 In patients in whom the administration of antiemetics does not relieve nausea, it is important for the palliative care team to propose opioid rotation and other necessary strategies in accordance with the condition.
In 2006, the number of patients with opioid therapy-related development/deterioration of nausea/vomiting was lower than in 2004, although there was no difference in the rate at which antiemetics were prescribed. As a reason for these, a difference in the incidence of nausea/vomiting between morphine and oxycodone can be considered since the prescription rate of oxycodone increased in 2006. However, there are no marked differences in the target area or pharmacological effects between the two drugs. Several studies compared the incidence of nausea/vomiting between oxycodone hydrochloride and morphine sulfate, and reported that the incidence of morphine sulfate-related vomiting was significantly higher, 15 and that there was no significant difference in the incidence of nausea. 16 In addition, another study indicated that, in the oxycodone hydrochloride-treated group, a lower proportion of patients complained of nausea/vomiting. 17 In this survey, when comparing the incidence of oxycodone hydrochloride-related nausea/vomiting between 2004 and 2006, the results were similar to those of comparison for all opioids between 2004 and 2006 (data not shown). As other possible reasons for the decrease in the incidence of nausea/vomiting, the effects of antiemetics and interventions by the palliative care team are considered. The palliative care team has designed the usage of agents for pain/adjuvant analgesic agents and strategies to reduce the side effects of opioids based on the WHO system.2,3 In addition, the palliative care team has studied various kinds of data on palliative care and provided care to patients. Over the years, palliative care has been enriched. The decrease in the incidence of nausea/vomiting may be associated with an increase in interventions by the palliative care team, such as a reduction in nausea/vomiting by improving meals and oral care or intervention in mental care. However, in this survey, interventions such as a reduction in nausea/vomiting by improvements in meals and oral care or intervention in mental care could not be evaluated.
The number of patients with opioid-related anorexia also decreased annually. This was possibly because the incidences of opioid therapy-related side effects, such as constipation and nausea/vomiting, decreased, as described above. The decrease in patients with anorexia may also be associated with pain control and activities by the palliative care team such as improvement in meals and mental care, although these items could not be evaluated in this study.
This survey facilitated an understanding of palliative care team activities and our pain control program utilized by medical staff in our hospital, contributing to optimal drug prescription for opioid therapy. This survey also suggested that an increase in the prescription rate of prophylactic drugs is closely associated with a decrease in the side effects of opioids, and the combination of opioids with prophylactic drugs is essential for the prevention of the development of side effects. Thus, palliative care team activities may markedly contribute to prevent the side effects of opioids such as constipation, nausea/vomiting, and anorexia, leading to improvement in the patients' QOL. The role of the palliative care team in cancer pain treatment in which drug therapy is essential may become more important with an increase in the number of patients with cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.