
Abstract
Abstract
Few dying patients undergoing dialysis receive hospice care. An intervention to facilitate hospice referral was evaluated in a longitudinal prospective cohort study. Five hemodialysis units in Massachusetts were divided into intervention sites (N = 3 clinics) and control sites (N = 2 clinics). Five hundred twelve patients were screened to identify those with indicators of poor prognoses; 133 met the eligibility criteria and consented to participate. Eighty-two intervention subjects and 51 control subjects were followed for a median of 17 months. During that time, 45 died and 16 received hospice services. Directors from the community hospices were approached by the researchers and agreed to provide an educational outreach to the intervention clinics. Renal supportive care teams (RSCTs) consisting mainly of volunteer health-care providers recruited from the dialysis clinics and local hospices were notified about the high-mortality patients. Staff met periodically to discuss their contacts with subjects and/or family members from the intervention clinics, The subjects were encouraged to participate in advance care planning, and they were provided information about hospice resources. The control clinics did not have RSCTs, and their subjects received standard treatment. At the conclusion of the study, hospice services had increased at the intervention sites (p = 0.09), and the subgroup of ≥65-year-old subjects had undergone a significant increase (p = 0.05) in obtaining hospice care. Greater familiarity between hospice and dialysis staff along with outreach to patients with poor prognoses holds the promise of expanding hospice use—especially for the elderly.
Introduction
Background
Geriatrics and ESRD
In the United States, there has been steady growth in the number of older adults receiving HD, and the median age of the ESRD incident population is now 64.5 years old. 2 The death rate of prevalent dialysis patients ≥65 years old is four times higher than that of the general Medicare population. 8 The elevated mortality is understandable since approximately 40% of patients with ESRD are diabetic, 30% suffer from congestive heart failure and ischemic heart disease, and 10% have significant cerebrovascular disease.9–13
Geriatrics provides a model of care for patients with chronic disease in all its complex aspects, including optimizing functionality, treating symptoms, establishing goals, minimizing the hazards of hospitalization, and increasingly relying on palliative medicine and hospice referral.2,3 Over-reliance on the technological advances in nephrology has hitherto delayed application of basic geriatric principles to ESRD.14,15
Hospice, palliative medicine, and ESRD
Nephrologists are gradually coming to understand that death is a regular and unavoidable visitor to dialysis clinics and that they are obligated to find new ways to ameliorate symptoms and minimize suffering. 16 A 1991 Institute of Medicine report urged the renal community to attend more to the complex concern of determining when the burden of dialysis outweighs its benefit. 17 In 1997, the American Society of Nephrology (ASN) and the Renal Physician Association (RPA) decided to jointly develop a clinical practice guideline, and this led to publication of Shared Decision Making in the Appropriate Initiation and Withdrawal of Dialysis.18,19 The guideline provided a comprehensive review of the existing literature and reinforced the conclusion that familiarity with modern palliative medicine is a necessary skill for nephrologists. After conferring with the American Nephrology Nurses Association, the National Kidney Foundation, the Council of Nephrology Social Workers, and the Forum of the ESRD Networks, the RPA and the ASN urged application of palliative medicine principles and hospice referrals for all patients who decline or are withdrawn from dialysis.20,21 The guideline is in the process of being updated, but these last recommendations will remain in effect in the new iteration (AH Moss, personal communication, August 31, 2009). There is now growing recognition that hospice services represent a widely available, but underused, resource for this aging population.22–26
However, there are a number of barriers to hospice use in the ESRD population in the United States. There is a life-saving “culture” in nephrology that often makes accepting death difficult. The hospice benefit requires a non–renal-related diagnosis to provide coverage that will not require the hospice to cover the cost of dialysis for those patients who choose to continue dialysis while enrolled in hospice. This has led many dialysis and hospice providers to erroneously conclude that hospice services were not available to dialysis patients.
In October of 2004, the CMS 2746 Death Notification Form (completed by nephrologists for every patient receiving maintenance renal replacement therapy) was changed to include additional questions regarding whether the deceased had received hospice care, whether patients and families were involved in decisions to discontinue dialysis, and whether dialysis was withdrawn prior to death. Accuracy of the new information based on the CMS 2746 Form has been questioned, 27 but a recent U.S. Renal Data System study suggests a national hospice referral rate of 13.5% prior to death in patients receiving dialysis with marked regional differences. 6 These referral numbers contrast sharply with the overall use of hospice in the United States. 7
Given the increasing age of patients with ESRD, the continuing high mortality rate, and the low hospice referral rate, a pilot feasibility study of a communication and education intervention to increase access to hospice services for patients receiving HD in Massachusetts was conducted. The study objective was to develop, explore, and describe an intervention to facilitate hospice referral for ESRD patients who have life-limiting illness or are actively dying. The primary hypothesis was that hospice services rates will be higher among patients who get the intervention compared to control patients.
Methods
Study sample
Between July 2006 and September 2007, all patients (N = 512) receiving HD at five Fresenius Medical Care North American dialysis clinics in western Massachusetts directed by the nephrologists of the Western New England Renal Transplant Associates were screened for increased mortality.
Design, setting, and data collection
A longitudinal prospective cohort pilot study was conducted at the five HD clinics; three of the clinics were selected as intervention sites and two others as control sites offering usual care. The intervention chiefly entailed acquainting the dialysis staff (especially the social workers) and patients with the criteria and services offered by their community hospices. At the beginning of the study, the local hospice directors were contacted and agreed to provide educational outreach to the dialysis clinics. Renal supportive care teams (RSCTs) were organized at each intervention clinic and consisted of volunteer staff from local hospices, dialysis social workers and nurses, and a few community physicians and nurses who shared an interest in palliative care. The RSCT members underwent a 1-day training course that included lectures about hospice, palliative care, and ESRD end-of-life issues, such as symptom management. After being provided with a list of high-mortality subjects, each of the RSCTs developed its own individual approach to providing support. Each RSCT had monthly or every-other-month meetings or conference calls to review the cases, and the hospice members provided information about how to make referrals. The members of the RSCTs periodically contacted subjects and/or family members to encourage advance care planning, discuss hospice resources, and offer general support; support was intentionally never defined or operationalized. The control clinics did not have RSCTs, and subjects received standard treatment.
Actuarial and clinician predictors of poor survival were obtained from chart reviews and brief contact with the primary nephrologists. The presence of any of three prognostic indicators were used to select subjects with life-limiting illness:
The modified Charlson Comorbidity Index (CCI) predicts survival in both incident and prevalent dialysis patients and is a better predictor than age, diabetes, and alternate models, such as the Davies Stokes score.28,29 CCI scores were calculated using the methodology described by Beddhu et al.,
30
which factors in age and assigns scores to different comorbid disorders. Serum albumin (<3.5 g/dL) is associated with a 50% 1-year survival and a 17% 2-year survival rate.
31
Nephrologist estimates of prognosis were obtained by requesting the primary nephrologist to answer the Surprise Question (SQ), “Would you be surprised if this patient died during the next six months?”32–35
This combination of subjective and objective indicators was chosen so that the study cohort would have an aggregate 6–12 month mortality rate of approximately 50%. 36 Patients were considered to be eligible for recruitment and consent if they were adults (≥18 years old) receiving HD at one of the study sites and if they had a CCI score ≥9, decreased albumin, or a negative response to the SQ.
After screening, consenting subjects from the all of the clinics and their family members were contacted by the research associates for an initial battery of tests. Baseline measures of performance and perceived health included: Karnofsky Performance Index, Katz ADL (activities of daily living), Lawton IADL (instrumental activities of daily living), Self-Perceived Health Question, and CMAS (condensed memorial assessment scale).35,37,38 These measures are reliable, well validated, and extensively used in geriatric and palliative care research, although only the Karnofsky and CMAS have been validated in ESRD. 39 To reduce respondent burden, all subsequent contacts for data collection took place solely with family members; they were contacted every 2 months and information elicited about sources of support, new medical problems, and unexpected hospitalizations. Family members were recontacted following patient deaths, and information was compiled about mortality, discontinuation of dialysis, site of death, and hospice referral. Patient mortality data were collected through June 30, 2008.
Statistical analysis
Subject characteristics and outcomes were compared between the intervention and control groups using chi-square tests for categorical variables, two-sample Student t-tests for continuous variables, and nonparametric Wilcoxon rank sum tests for scale variables or continuous variables with highly skewed distributions. Data were summarized for the two groups as percentages, means (standard deviation), or median (interquartile ranges) depending on the analytic method used. Survival time at specific time points and 95% confidence intervals were calculated using the Product-Limit method, and survival curves showing estimated survival over time were compared between the two groups using a log-rank test to account for censored observations. The outcomes of hospice use and discontinuation of dialysis were compared between the groups using both the chi-square test and a random effects model to control for potential site effects using generalized linear mixed models. Outcomes were also reanalyzed separately stratifying subjects by age (≥65 vs. < 65 years old). These subgroup analyses were outlined in the analytic plan for this study prior to collecting any data, and thus no adjustments were done to p-values to account for multiple comparisons.
Patient survival over the follow-up period was also compared between patients who were screened and classified as eligible vs. not eligible for study enrollment. The log-rank test was used to compare the survival curves between eligible and noneligible patients to see if the screening criteria used for the study successfully identified higher risk patients. All analyses were done using the SAS system version 9.1 (or higher) for Windows. 40 A p-value of 0.05 was used to determine statistical significance for all analyses. This was a pilot study initially designed to enroll 64 subjects per group in order to have 80% power to detect a three- to sixfold increase in hospice utilization (depending on magnitude of within site clustering) above a hypothesized control rate of 10% hospice use.
Results
Figure 1 depicts a study flow chart, which shows how 133 subjects (82 intervention and 51 control) were recruited from the 512 screened patients. In Figure 2, separate curves are drawn for 244 patients who met the high-mortality eligibility criteria and 268 patients who did not fulfill eligibility. As expected, patients survival was significantly worse for patients who met the study eligibility criteria with 6-month and 12-month Kaplan–Meier estimates survival of 86% and 74% compared to those that did not with 6-month and 12-month Kaplan–Meier estimates survival of 98% and 95% (p < 0.0001 from log-rank test comparing survival curves).
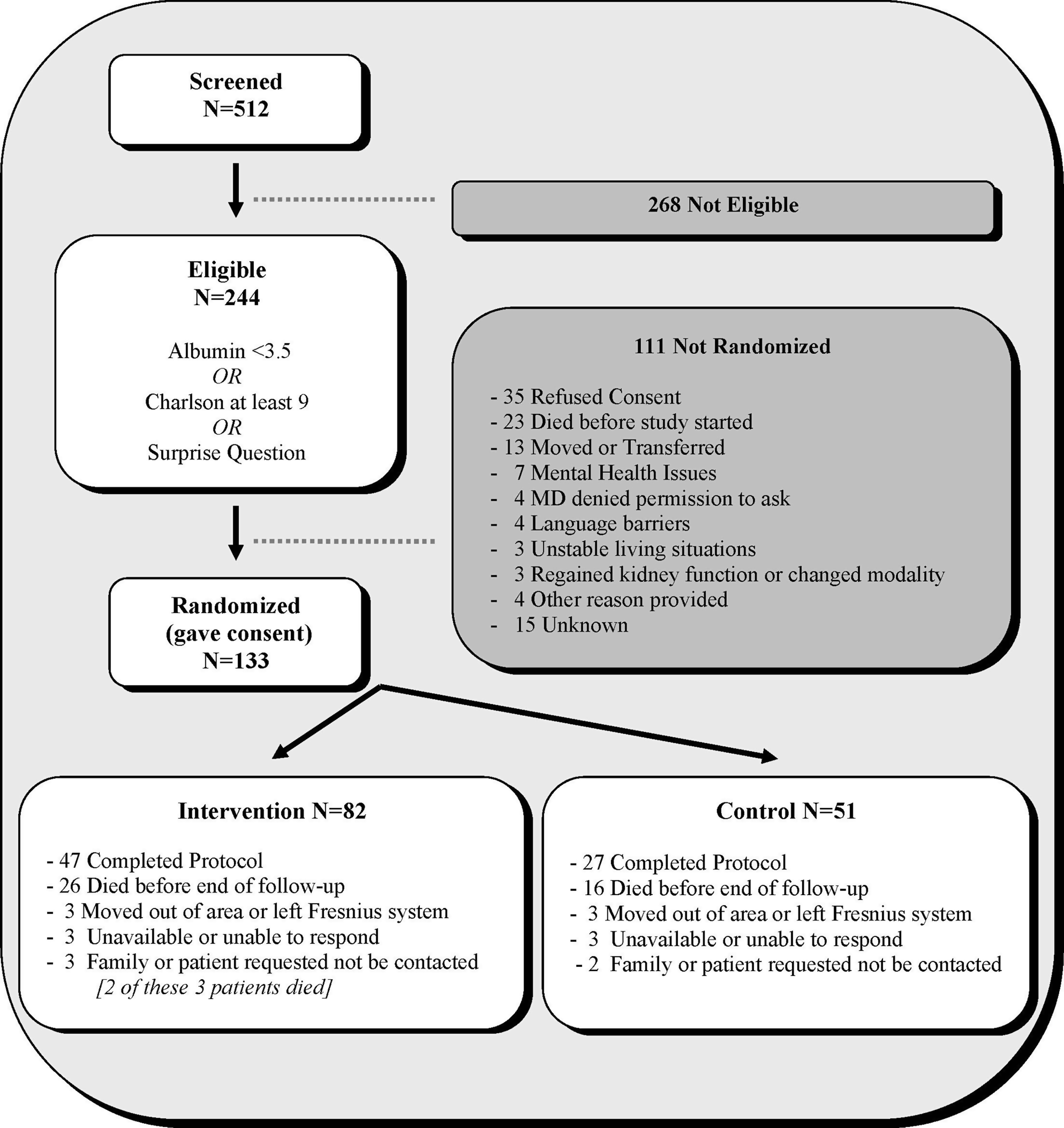
Study Flow Chart.
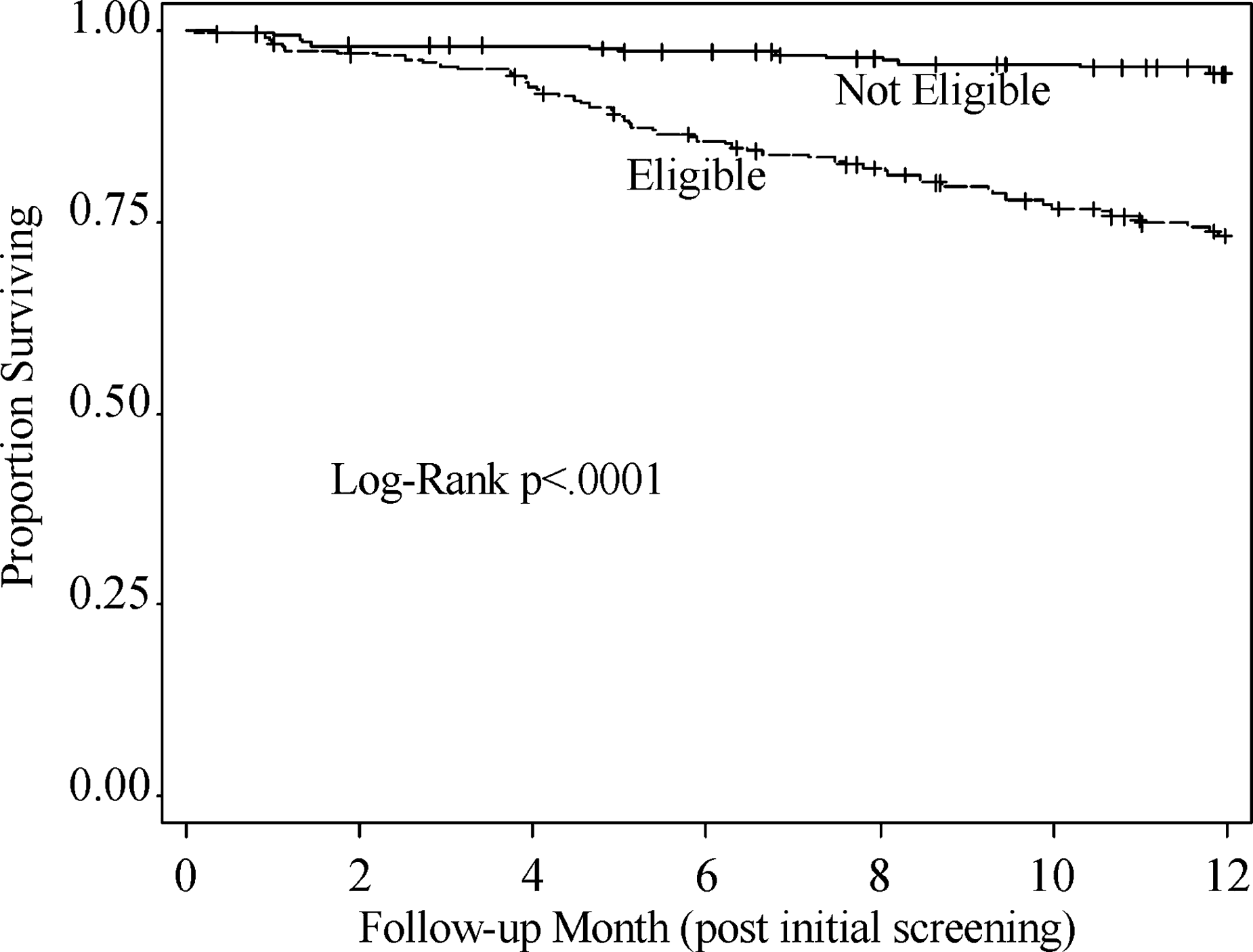
Survival of Eligible Cohort vs. Not Eligible Cohort–Kaplan Meier Survival Curves.
Baseline characteristics for the intervention and control subjects are presented in Table 1. The mean age in the intervention group was a little older than in the control group (73 vs. 68, p = 0.06) and there was a higher percentage of white patients in the intervention vs. control group (93% vs. 63%, p = 0.0001). There were no significant differences between groups with respect to marital status, months of HD, or cause of ESRD. Baseline values of functional scales and measures of performance and perceived health are presented in Table 2. The control group had a significantly higher Karnofsky Performance index than the intervention group (p = 0.0176), but no other significant differences were found in the Katz ADL, Lawton IADL, Self-Perceived Health, or CMAS scales. In summary, the two groups were reasonably similar at baseline, and the median follow-up for both was 17 months. Kaplan–Meier curves were used to get estimates of survival over time and the survival between the Intervention and Control groups was compared by using the log-rank test to compare the two survival curves. The estimated Kaplan–Meier 6-month survival rates from the intervention and control groups were 80% and 84%, while the estimated 12-month survival rates were 71% and 72%. There was no significant difference in survival over the follow-up period between the two groups (log-rank p-value = 0.67). These data are presented in Table 3.
p-values are either from the student t-test (age), Wilcoxon rank-sum test (months of hemodialysis [HD]), or the chi-square test (all other variables).
p-values comparing intervention and control group results are from the Wilcoxon rank-sum test.
Missing data for one person.
Student t-test.
Wilcoxon rank-sum test.
Log-rank test comparing survival curves.
Chi-square test.
A random effects model where a random intercept term was included to adjust for site effects used to compare outcome percentages between the intervention and control groups.
The primary outcome of this study was the use of hospice services. Discontinuation of dialysis and hospice utilization were also examined as a composite outcome. Table 3 shows that hospice was used in 16% of intervention subjects compared to 6% of control patients with an unadjusted p-value of 0.09. After adjusting for site as a random effect the p-value increased to 0.19. The composite outcome of hospice or discontinuation of dialysis showed a similar pattern with rates of 22% vs. 12% in the intervention and control groups respectively (p = 0.14 unadjusted, p = 0.15 adjusted for site). To further explore these outcomes, data were separately reanalyzed for older (≥65 years) and younger patients. Among the older subjects (representing about 70% of the total sample), the hospice usage rates were 18% vs. 3% (p = 0.05 unadjusted) in the intervention and control groups, respectively. These data were too sparse to perform a site-adjusted analysis. The hospice usage rate was 10% for younger subjects in both the intervention and control groups, but the small sample size limits our ability to draw meaningful conclusions for this subset. Another analysis examined hospice or discontinuation of dialysis in the first 6 months after the study began; results were similar and slightly attenuated with 12% of intervention patients getting hospice services and/or having dialysis discontinued compared to 2% of control patients (p = 0.04 unadjusted, p = 0.07 adjusted for site).
Discussion
Although there is a growing body of literature emphasizing the need to increase hospice services for dying dialysis patients—and especially the elderly—this is the first research study to prospectively use prognostic indicators and implement a renal supportive care intervention targeted to this high risk subgroup. The RSCTs consisted of interdisciplinary volunteer staff drawn primarily from the dialysis clinics and local hospices, who were encouraged to contact, educate, and facilitate discussions of advance care preferences with the subjects and their families. The staff familiarized each other and the subjects with renal palliative care and the availability of community hospice services. This research study found that the prognostic eligibility criterion was successful at identifying patients at high risk of mortality. The increased use of hospice in the subjects from the intervention sites approached statistical significance (p = 0.09), while a significant increase (p = 0.05) of hospice services was found in the ≥65-year-old subgroup.
The greatest strength of this pilot research is recognition that integration of geriatric care principles, palliative medicine, and nephrology can be implemented in HD clinics. The interdisciplinary staff became better acquainted with each other, at-risk patients and families were regularly contacted, and greater use of hospice services was found in the intervention cohort with the difference in the latter reaching statistical significance in older (≥65 years) subjects.
The present study successfully used two actuarial measures (LA, CCI), along with a new tool that relies on the clinician's prediction of survival (SQ). Further development and use of an integrated instrument based on this prognostic model has the potential to become an important starting place for palliative medicine discussions with patients and an empirical basis for advanced care planning with consideration of appropriate hospice referral. 41
There are a number of limitations to this study's design. The trial was clinic-centered rather than randomized at the patient level. The investigators recognized that there are some limitations in this choice of design, although most analytic disadvantages can be accounted for by using statistical methods such as multilevel or mixed models. 42 From a practical standpoint, a clinic-centered intervention was appealing because it took advantage of the fact that most dialysis units rely primarily on protocol-driven models of care, and the proposed intervention was not directed solely at patients and families but also intended to catalyze a cultural change in the clinic. The other problem with randomization at the patient-level is contamination; once the intervention is implemented in a particular HD clinic, it is unlikely that control subjects will be treated any differently than those who receive the intervention.
The study sites were not randomly selected to be an intervention vs. a control site; one large and one mid-sized clinic were selected for each of the two groups. However, in retrospect there was no statistical difference between control vs. intervention sites as to the hospice referral rate prior to the study.
Another limitation of this type of study is that when studying a high risk population some subjects may die shortly after the study begins and before the intervention may have time to even have an impact. This can possibly result in the intervention appearing less effective.
The study was limited to a small sample of patients drawn from five Massachusetts dialysis clinics—although their demographics are comparable to those of the region and the nation. It is gratifying that there were no significant differences between the characteristics of the intervention and control groups with respect to marital status, months on HD, cause of ESRD, and most of the measures of patient health and function. There were potentially important baseline differences between groups (more whites and lower Karnofsky scores in the intervention group) that may have biased hospice use to the intervention group. A series of logistic regression models were run for the composite outcome of hospice or dialysis discontinuation to check interactions of the treatment effect with other baseline characteristics, including race and functional status. None of the tests for interactions reached statistical significance. In addition, although p-values were not adjusted for multiple testing and this may result in an inflated alpha error, this is balanced by the analyses having been preplanned. Lastly, the reproducibility of the intervention can be legitimately questioned. Nevertheless, this was a pilot study, and the common theme was clearly that every dialysis clinic is situated in a community with hospice resources and that they will mutually benefit by becoming acquainted with each other.
In conclusion, it bears stating that a hospice referral rate of 18% for the dying elderly HD patients from the intervention cohort may be statistically better than the 3% found among the elderly controls, but it is still pitifully small compared to what one would consider to be a reasonable goal. A number of hospice referral barriers for patients receiving HD have now been identified, some of which can hopefully be overcome in the future.43–46 These begin with a lack of familiarity between hospice and dialysis unit personnel, 6 but also include a need for more accurate prognostic models to identify HD patients who are unlikely to survive 6 months,47,48 local hospice concerns over Medicare reimbursement for patient's who continue dialysis,49,50 and an absence of training or experience by dialysis staff in the communication of bad news. 51 There is no tradition within nephrology for referring dialysis patients for hospice services, there are distinct knowledge deficits and reimbursement barriers as to how to carry this out appropriately, and all the while there is a growing appreciation of the potential value of hospice for this population and especially the elderly subgroup that discontinues renal replacement therapy. 52
Footnotes
Acknowledgments
The project described was supported by Grant Number 5 R21 DK076563-02, “A Hospice Intervention for Older Adults with ESRD: Sharing the Caring” from the National Institutes of Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
Dr. Cohen, Ms. Ruthazer, and Dr. Germain have no commercial associations to disclose. None of the authors have any actual or potential conflict of interest in connection with the manuscript.