
Abstract
Abstract
Background:
Palliative care is part of comprehensive family practice; however, many physicians do not feel confident in the biomedical and psychosocial realms. Although improving residency training to address this is necessary, there is little consensus on the best education methods.
Objective:
To conduct a systematic review of postgraduate curricula in palliative care to incorporate the most effective components into a family medicine education program.
Methods:
Studies of palliative care curricula conducted in postgraduate medical training programs that contained an evaluative component and published since 1980 were systematically examined by investigator pairs using standard selection criteria and data collection forms. Discrepancies were resolved by consensus. The outcomes examined were communication skills, knowledge, attitudes, and comfort/confidence level.
Results:
28 studies were included after reviewing 174 abstracts. Most studies (n = 21) used survey pre–post design with no control group. Outcomes were grouped into communication skills, knowledge and attitudes and confidence. Workshops with simulated patients or role plays improved communication skills. Relatively brief strategies such as short workshops showed objective improvements in focused knowledge areas. Either clinical rotations or multi-faceted interventions were required to produce improvements more broadly in knowledge base. Only a few studies examined the sustainability of outcomes.
Conclusions:
An effective palliative care curriculum will need to use a multifaceted approach, incorporating a variety of intentional strategies to address the multiple competencies required. There is a need for more rigorous curricular evaluation.
Introduction
With the shift in medical education toward measurable competencies, national organizations such as the College of Family Physicians of Canada, Educating Future Physicians in Palliative and End of Life Care (EFPPEC), and the American College of Graduate Medical Education have identified palliative and EOL care core competencies for residents.16,17 Despite these initiatives, there is no consensus as to the most effective methods by which to educate future physicians about palliative care. There have been two recent systematic reviews of teaching and learning in palliative medical education.18,19 The first review of 43 English-language articles of interventions targeted to undergraduate medical training, revealed a paucity of good quality quantitative and qualitative trials. 18 These articles were categorized by the authors as descriptive, with limited discussion of curricular outcomes. The second, more recent review was limited to studies conducted in the United States, examining only 7 articles across heterogeneous curricula. 19 Only 2 were at the postgraduate level. In those articles with an objective measure of attitudes or knowledge/skills, all curricula produced improvement. There were no conclusions drawn by either review about the optimal timing, length or format of curriculum. No comments were made with regard to sustainability of educational impact. Thus, there appears to be little in the literature targeted specifically at the postgraduate level that could guide the development and evaluation of an optimal residency curriculum in EOL care for future physicians.
In keeping with a recent emphasis on the importance of systematic, evidence-based research within medical education,20,21 this article presents the results of a systematic review examining studies of postgraduate curriculum in palliative and EOL care that report an evaluation/intervention. In addition, the impact of the type, intensity, duration or frequency of the learning intervention on different educational outcomes was examined as well as the sustainability of positive results.
Methods
Study selection
We conducted a systematic review of published English-language journal articles that described palliative and EOL care curriculum programs in postgraduate medical education that also included evaluation of the curriculum.
In August 2008, the following databases were searched from 1980 to 2008: MEDLINE, Cumulative Index to Nursing and Allied Health (CINAHL) and Exerpta Medica (EMBASE). The search combined MeSH terms pertaining to palliative, hospice, end-of-life care, and terminal care and death; internship and residency; and terms relating to educational measurement, knowledge, clinical competence and program evaluation. Additional studies were identified by hand searching bibliographies of included published articles. Grey literature, conference abstracts, books and technical reports were not searched. The complete search strategy is available upon request from the authors.
A two-step inclusion process was undertaken. After removing duplicate articles, two pairs of authors reviewed the identified studies and systematically assessed the study abstracts based on standardized selection criteria. Where inadequate information was provided in the abstract, the full article was reviewed to determine inclusion. Standard criteria were developed by the research group for full paper inclusion. Final article inclusion was determined by consensus among all four authors.
Inclusion criteria were: English-language articles pertaining to any type of EOL care curriculum, and including a curriculum outcome measurement (e.g., knowledge, attitudes, or confidence). The population included, but was not exclusive to, postgraduate medical trainees (i.e., interns, residents, or fellows). Studies that met the above criteria but only described an evaluation of residents' satisfaction with the curriculum and no other outcomes were excluded.
Data extraction and synthesis
Articles were divided between four study authors (A.T., E.S., D.M., S.W.) who independently extracted data using the structured form developed by the research group. A check of the completeness and accuracy of the data extraction was done by one of two nonphysician authors (S.B., M.H.) who had training in research methodology.
Because of the significant heterogeneity of studies, results have been presented descriptively to provide an overview of:
Methodology and study design;
Curricula that had a positive impact on communication skills, knowledge, or attitudes and confidence;
Impact of the intensity (duration, frequency, number. and type of activities) of the program curriculum on its effectiveness; and
Sustainability of educational outcomes.
Results
Of the 175 titles and abstracts examined, 131 articles did not meet our initial inclusion criteria, leaving 44 for full article consideration. After examining the 44 articles in full, a further 19 did not meet inclusion criteria, leaving 25. Three additional articles were identified from the bibliographies of these 25, for a total of 28 articles from which data were extracted.22–49 Figure 1 summarizes the process and reasons for paper exclusion. A summary of the methodology, outcomes and conclusions of the included papers can be found in Table 1.
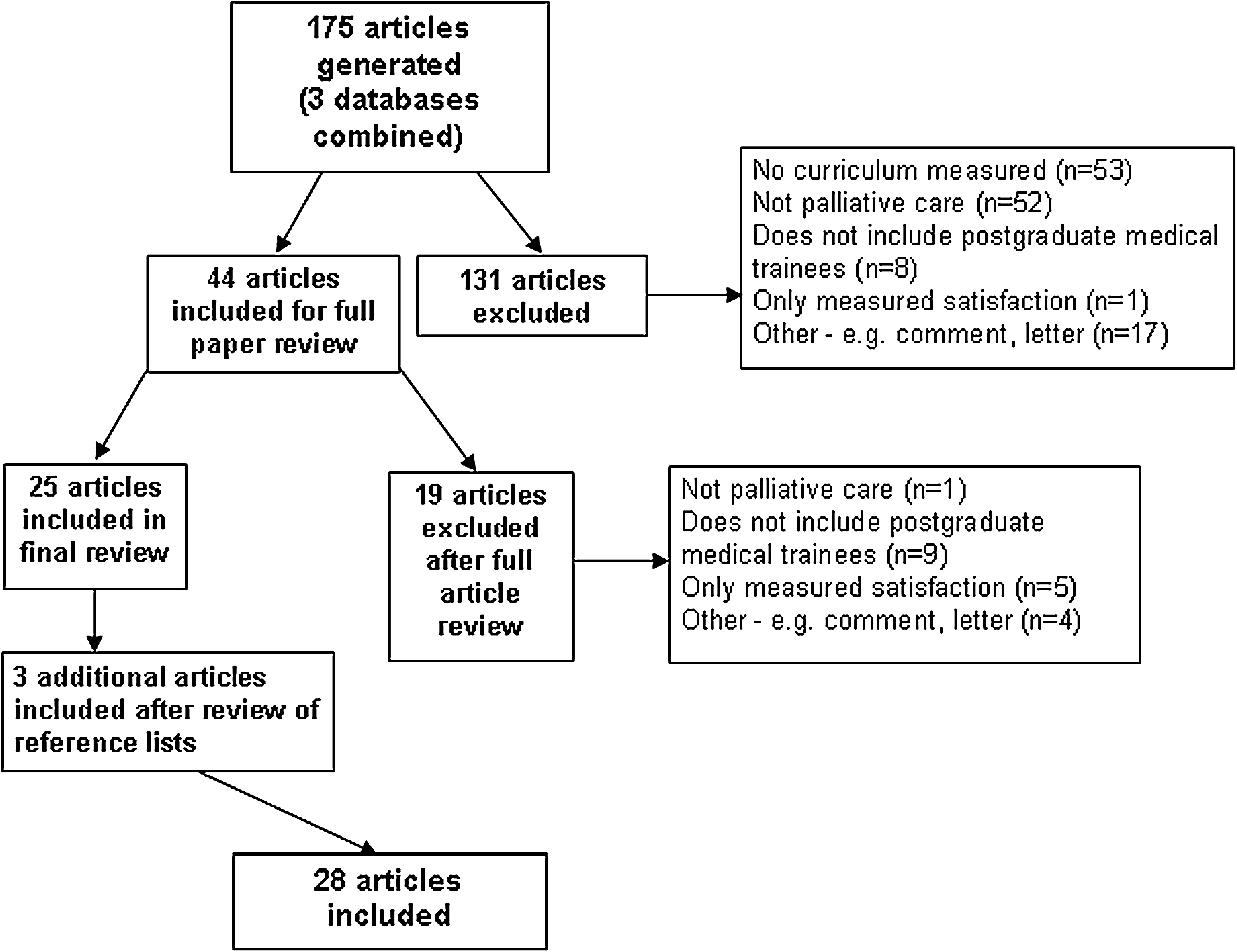
Flow diagram of studies included in the systematic review.
Methodology and study design
Twenty-five of the 28 papers22–44,47–49 used survey methodology that assessed either EOL care knowledge (20), confidence/comfort and attitudes (17), self-perceived competence (5), or a combination of these before and after the intervention. Most of the surveys were administered immediately to 3 weeks following the intervention. Only 7 of the 28 trials had a control group; 6 of these were prospective in design22,27,38,43,45,49 and 1 used national standard scores as the comparator group. 39
Seven papers used an objective, observable measure to evaluate target behaviors. Five studies22,28,30,46,48 used simulated patient interviews to measure communication skills and two studies44,45 used chart audits to examine prescribing behavior or referral to hospice.
Communication skills
Of the 6 studies that evaluated communication skills (5 by objective observation, 1 self-assessed), 4 assessed skills both preintervention and postintervention focusing on either the process of death notification or delivering bad news, and discussing patient preferences for treatment.22,28,31,46 Each of these included didactic sessions; all used either simulated patients (SP) or role play for skills practice. All of these interventions showed significant preimprovement/postimprovement in the specific communication skills examined as assessed using an objective behavior checklist with audio- or videotaped SP encounters. In the only article that used a control group, a 2-day retreat improved resident's ability to communicate bad news and discuss EOL preferences both preintervention/postintervention and compared with the control group. 22
Of the remaining 2 articles, the first assessed the impact of a 1-month hospice rotation on the ability of residents to talk with patients about goals of care and dying using a similar objective checklist with SPs. Although all of the residents were able to complete the tasks of the interview following the rotation, there was no prerotation assessment in this study. 48 The final article assessed the feasibility of using faculty assessment of actual patient interviews as an educational strategy, but did not assess the impact of the intervention itself. 30
Knowledge
Of the 20 studies that evaluated improvement in knowledge around various palliative care topics, 11 used a written examination,25,27,34,38–41,43,44,48,49 8 asked about self-perceived changes in knowledge24,29,31,33,35,37,42,47 and 1 used an objective chart review to examine prescribing behavior. 45 All but 2 of these 20 studies29,44 administered surveys preintervention and postintervention.
The educational interventions ranged from clinical rotations of varying length (1 week to 1 year longitudinal) combined with didactic teaching in 11 of the studies,25,27,29,34,37–40,44,47,49 seminar series or Web modules in 6,23,34,41–43,45 workshops or retreats in 2,26,36 and a brief 10-minute intervention and pocket card in 1 study. 24 All but one of these interventions measured improvements in either tested or self-perceived knowledge.
Six articles compared knowledge gained using an objective examination administered pre and post intervention with a control group.27,38,39,43,45,49 Four used residents as controls,27,38,45,49 one used faculty, 43 and one compared resident participant scores with those of the national standard average. 39
One of these studies was unable to find an improvement in knowledge compared with a control group. However, 53% of control versus 37% of intervention group reported prior palliative care experience, which was the factor most predictive of the final knowledge score. 27
Of the remaining controlled studies, relative knowledge improvements were 18, 46 and 28% (p = ≤ 0.0001 for all), respectively for clinical rotations of 1 and 4 weeks and a 14-week series of small group sessions.38,43,49 The sixth study used chart audits to show a 40% decline in meperidine use and a 30% improvement in the use of bowel regimens compared with controls, 6 months after exposure to 2 case-based modules in pain management. 45
Attitudes, confidence/self-perceived competence and comfort
Given that the majority of these articles addressed both attitudes toward EOL care and comfort levels or confidence/self-perceived competence in providing this care, these outcomes were combined. One article that examined critical appraisal confidence only is not included here. 35 In five of these studies with either internal medicine or family medicine residents, the preintervention attitude or confidence scores were very positive, thus, there was either little postintervention change, or the authors did not remeasure attitudes.26,27,30,38,47 Where residents' preintervention assessment of confidence was lower, virtually all educational interventions were effective at increasing resident confidence/self-perceived competence and comfort in the area addressed by the curriculum. Only one study compared the observed attitude change with a control group, and did not find a difference between groups. However, as previously mentioned, significantly more residents in the control group had prior palliative care experience. 27 A 1-week combined chronic pain/palliative care rotation for critical care fellows, resulted in some attitude measures moving in the opposite direction to that expected. 25 In this very small study, the curriculum was not evaluated positively by the participants, as the fellows felt that it was not relevant to their future practice.
Impact of the intensity of the educational intervention
There was no apparent association between the type of intervention and either its length or the educational outcome. However, the length of an intervention is only one component of educational intensity. Because there appears to be no definition for “educational intensity” in the medical education literature, our project team defined intensity levels based on frequency and duration of the intervention as well as the number and type of educational strategies used. Low intensity was defined as a short (less than 8 hrs), single teaching strategy (e.g., workshop, seminar series, educational handout); moderate intensity as longer and/or multifaceted educational strategies, such as simulated patients or a clinical component less than 2 weeks; and high intensity as substantial clinical exposure (greater than 2 weeks), in addition to multifaceted educational strategies such as rounds, and case discussion. Studies are presented by intensity of educational intervention in Table 2.
EOL, end of life; EPEC, Education on Palliative and End-of-Life Care; DNR, do not resuscitate.
There was significant heterogeneity of intensity of the educational interventions in the studies. Self-reported outcomes, including confidence, improved with any level of intensity of intervention. Low intensity interventions objectively improved focused knowledge (i.e., use of pain medication, or hospice care).41,45 Moderate intensity interventions which included simulated patients, showed objective improvements in EOL communication skills.22,28,46 Both moderate and high intensity interventions improved objective assessments of broad knowledge in EOL care.
Examination of the seven studies that used both a control group and objective outcome measurements revealed that all but two of the interventions were of high or moderate intensity.22,38,39,43,49 Where knowledge was measured, all of these studies showed improvements from baseline compared with the control group. The two lower intensity studies showed mixed results. As previously mentioned, the single study of low intensity using a case-based module to teach pain management did show knowledge improvements in this specific area. However, four 1-hour discussions during a general internal medicine rotation did not improve knowledge or attitudes about EOL care. 27
Sustainability
Only five papers examined the sustainability of positive outcomes beyond the immediate post-intervention period.31–33,39,45 Three of these assessed outcomes 3 months following the intervention. A 2-hour workshop involving SPs, a new symptom management order set, and a 3-hour workshop for surgical residents showed sustained improvements in confidence and self-perceived EOL care competence, comfort with symptom management discussions and speaking with patients about EOL care issues, respectively.31–33 Two educational modules on pain and symptom management produced improvements in opioid prescribing at 6 months when assessed by chart audit. 45 Finally, an intensive inpatient experience and series of educational rounds sustained knowledge improvement with various broad palliative care topics 1 year after the rotation. 39
Discussion
This systematic review appears to be the first attempt to examine the literature regarding postgraduate medical education in palliative care where evaluations of the educational intervention are described. Overall study quality was poor, with only 7 of 28 studies including a control group and a significant number of studies using self-report to assess acquisition of knowledge and competency. Recent literature, including 2 systematic reviews, has called the value of professional self-assessment into significant question.50–52 Indeed, the worst self-assessment accuracy has been found among those who were the least skilled and the most confident. 52 Knowledge-based activities may be particularly poorly self-assessed, as compared with practical skills based activities. 50 In this review, virtually any amount and type of educational intervention was shown to improve resident's reported confidence to provide EOL care. No studies compared reported change in attitude or confidence with a control group of residents. Additionally, no studies compared confidence with an objective assessment of clinical competence. This lack of robust outcome measures is consistent with a review of 599 medical education studies, where learner performance was assessed in only 49.4% of articles and patient care outcomes in only 0.7%. 53
This review may be limited in its generalizability, given that the vast majority of papers were from North American residency programs. It is also possible that significant literature may have been missed, despite the comprehensive search strategy.
Despite these limitations, several conclusions may be drawn by examining the best quality studies, and those using objective outcome measures. Communication skills in palliative care can be effectively taught with the use of simulated patients in a short 2-hour to full-day workshop. It is difficult to determine if these skills can be maintained, however, as only confidence and not competence in EOL communication was assessed 3 months postintervention. The use of actual faculty observed patient interviews appears feasible and acceptable, but needs to be evaluated using a reliable tool to assess observable behaviors. Educational modules can produce improvements in focused areas of knowledge such as appropriate use of opiates, and criteria for hospice care, with the former showing sustainability at 6 months. Moderate- or high-intensity interventions with longer seminar series or a clinical component appear to be necessary to more broadly improve knowledge base in EOL care. No conclusion can be drawn regarding the exact length of the clinical rotation necessary, as rotation lengths between 2 weeks to a longitudinal 1 year rotation all have a positive impact on objective measures of knowledge.
It is possible that the intensity of the intervention may have a significant impact on sustainability of knowledge, confidence or attitude; however, this was measured infrequently. The one study that demonstrated improved EOL care knowledge one- year after the activity was a high intensity intervention that included a clinical rotation supplemented by interactive rounds and resources.
It appears that a multifaceted approach with some intentional focus on individual competencies will be necessary to meet all of educational requirements of postgraduate learners in EOL care. This would potentially involve simulated patients and role play to address communication skills, and some highly relevant clinical exposure supplemented with academic sessions, resource material, or educational modules to address knowledge and other clinical skills. This approach is supported by the literature from continuing professional development. A recent systematic review of educational interventions to increase primary care physicians knowledge and skills in palliative care, suggested that a multifaceted approach may be most effective. 54
In conclusion, given the recent shift to an outcomes or competency based paradigm in medical education,55–57 with increasing emphasis on patient care outcomes,20,21,58 curriculum planners in EOL care will need to change the focus from time-based clinical rotations toward a variety of educational experiences designed to meet the expected competencies of the graduating resident. It will be important to incorporate external, objective evaluations for both resident and curriculum assessment. To address ongoing gaps in our understanding of optimal EOL residency training, new curricula need to be described and their effectiveness and sustainability robustly evaluated using objective outcome measures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.