
Abstract
Abstract
Context:
Palliative care consultation teams in hospitals are becoming increasingly more common. Palliative care improves the quality of hospital care for patients with advanced disease. Less is known about its effects on hospital costs.
Objective:
To evaluate the relationship between palliative care consultation and hospital costs in patients with advanced disease.
Design, setting, and patients:
An observational study of 3321 veterans hospitalized with advanced disease between October 1, 2004 and September 30, 2006. The sample includes 606 (18%) veterans who received palliative care and 2715 (82%) who received usual hospital care. October 1, 2004 and September 30, 2006.
Main outcome measures:
We studied the costs and intensive care unit (ICU) use of palliative versus usual care for patients in five Veterans Affairs hospitals over a 2-year period. We used an instrumental variable approach to control for unmeasured characteristics that affect both treatment and outcome.
Results:
The average daily total direct hospital costs were $464 a day lower for the 606 patients receiving palliative compared to the 2715 receiving usual care (p < 0.001). Palliative care patients were 43.7 percentage points less likely to be admitted to ICU during the hospitalization than usual care patients (p < 0.001).
Comments:
Palliative care for patients hospitalized with advanced disease results in lower costs of care and less utilization of intensive care compared to similar patients receiving usual care. Selection on unobserved characteristics plays an important role in the determination of costs of care.
Introduction
Hospital-based palliative care programs, focused on pain and symptom management, communication and goals of care, and assistance with transitions among sites of care, have become an increasingly common way to improve hospital care for patients with advanced disease and their families.9,10 Over 50% of hospitals with 50 or more beds have palliative care programs as do most VA hospitals. 9 Studies suggest palliative care consultation can improve patient symptom management and increase family satisfaction with care3,11–14 and may reduce costs.15–21
This study builds on and amplifies prior studies, including our own smaller study 15 by using a relatively large sample of 3321 veterans admitted with advanced disease to five VA medical centers and comparing costs for those receiving palliative and usual care. It addresses limitations of prior studies by using an instrumental variable approach to account for the selection into treatment on unmeasured patient characteristics.22–24 We compared average direct hospital costs for patients admitted with advanced disease who were referred for palliative care consultation with advanced disease patients not referred for palliative care consultation. We also examined the relationship between palliative care consultation and ICU admission because ICU costs are approximately 20% of overall hospital costs. 25 The findings from this study are relevant to current efforts by VA to expand palliative care services.
Methods
Study population
We conducted a retrospective, observational cost analysis using a VA (payer) perspective. The sample included all patients age 18 and older admitted to all five Veterans Integrated Service Network (VISN) 3 acute care facilities between October 1, 2004 and September 30, 2006 with at least one of the following advanced diseases measured with ICD-9 codes: (1) metastatic solid tumor, (2) central nervous system (CNS) malignancies, (3) metastatic melanoma, (4) locally advanced head and neck cancer, (5) locally advanced pancreatic cancer, (6) human immunodeficiency virus/acquired immune deficiencty syndrome (HIV/AIDS) and at least one of the following secondary diagnoses: hepatoma, cirrhosis, lymphoma, cachexia, or other cancer, (7) congestive heart failure (CHF) or chronic obstructive pulmonary disease (COPD) and either two or more hospitalizations in any 6 months of the study period or one or more ICU admissions for CHF or COPD during the study period. These diagnoses and stage of disease include those that are considered appropriate for palliative care by other palliative care researchers and clinicians.26–31 Patients were included in the sample if their ICD-9 CM diagnostic code for primary diagnosis (diagnostic code at admission) or principal diagnosis (ICD-9 code responsible for the major part of the stay) or any secondary ICD-9 code indicated any of the seven advanced diseases listed above. Patients were excluded if their hospital length of stay (LOS) was less than 48 hours or the hospitalization was for routine chemotherapy.
Sources of data
We obtained administrative and clinical data for the sample from the Veterans Health Administration (VHA) national database accessed through the VA Information Resource Center (VIReC). The VHA Medical SAS inpatient dataset has files with one record for each hospital stay with patient demographic, clinical and diagnostic information, admission and discharge dates, and date of death if appropriate. We obtained estimates of inpatient care costs from the VA Decision Support System National Data Extracts (DSS NDE). DSS is the system used by the VA to determine costs of patient care. 32 The NDEs summarize total costs for the entire inpatient stay. There are also subtotals of costs for laboratory, pharmacy, surgery, radiology, nursing, and all other care for the stay. The NDEs also identify ICU days during the stay and ICU costs.
Measures
Outcomes
We measured direct costs of hospital care from VA cost databases noted above. In addition to total direct costs, we examined direct costs for laboratory, pharmacy, radiology, nursing, and surgery. Additionally, we measured each ICU admission and ICU length of stay (LOS) during the hospitalization.
Predictors
The key independent variable was a binary indicator for whether the hospitalization included a palliative care consultation. Subsequent hospitalizations were classified as palliative care for these patients. All palliative care teams in all inpatient VHA facilities in VISN 3 use a standardized consultation note in the electronic medical record. This was the source for the treatment indicators.
Other predictors measured demographic characteristics and current health status of the subjects. These measures included the primary disease (HIV/AIDs, advanced cancer, CHF, COPD), age, race/ethnicity, principal admitting diagnosis, hospital death, comorbidities, economic status, LOS, and site. Comorbidities were measured using the Elixhauser index, 33 an algorithm that includes 30 categories of comorbid illness identified by secondary diagnosis codes and discharge diagnosis-related group (DRG). Income status was measured using VA enrollment priority group that measures low income and higher levels of veteran disability. The natural log of the LOS was included because costs tend to be higher early in the stay. Because we were concerned about possible endogeneity for LOS, we conducted the analyses with and without LOS in the models. Last, we controlled for site differences using indicator variables for the five sites.
The study protocol was reviewed and approved by the Institutional Review Boards at all five VA study sites including the two VA medical centers where coinvestigators are located, and the Mount Sinai School of Medicine.
Statistical analyses
Instrumental variable methods can produce unbiased estimates of the treatment effect when they employ an appropriate instrument to adjust for unmeasured selection into treatment (i.e., when unmeasured characteristics of patients affect both the likelihood of receiving treatment (e.g., palliative care consultation) and the outcome).23,34–36 An appropriate and valid instrumental variable must be a measured factor that is substantially correlated with the treatment conditional on all other measured factors and is uncorrelated with the outcomes of interest except through its effect on the treatment. The nature and direction of the selection for palliative care is that we expect the sickest patients (based on unmeasured risk factors) to be more likely to be offered palliative care. Physician preferences for offering palliative care can be the source of valid instrumental variables if patients are randomly assigned to physicians, as is effectively the case in the VA. 37 Thus, we used indicators for the attending physicians as the instruments for patient selection into palliative care. We assumed that physicians vary in their preference for palliative care and a patient who would be referred to palliative care by some physicians would not be referred by others. Moreover, if physician tendency to refer patients is to be a valid instrument, then it must be exogenous. It should influence costs of hospital care only through the treatment choice, or more specifically, it should not be correlated with unmeasured characteristics in the patient's outcome (cost or ICU stay) equation. Because attending physicians were assigned to patients quasi-randomly (they were assigned on a rotational basis) in the hospitals in our study, physician characteristics are orthogonal to patient characteristics such as unmeasured health status. Thus, we exploited this quasi-experimental nature of the process of physician assignment to patient process to obtain a valid instrument. We expected it to substantially increase the reduction in utilization resulting from palliative care. We included one indicator variable for each attending doctor with 10 or more patients. Doctors who saw less than 10 patients were grouped together in the reference category.
We used gamma instrumental variable regressions to estimate treatment effects on health care costs38–40 and bivariate probit models to estimate treatment effects on ICU stays. 41
Results
Table 1 shows the characteristics of the 3321 veterans in the sample, 606 (18%) who received palliative care and 2715 (82%) who received usual hospital care. Palliative care patients were older, more likely to die during the study, and had more hospitalizations during the study period compared to usual care.
Does not add up to 100% because veterans could have more than 1 advanced disease.
HIV/AIDS, human immunodeficiency virus/acquired immune deficiency syndrome; SD, standard deviation; ICU, intensive care unit; LOS, length of stay.
The bottom portion of Table 1 shows the characteristics of the 6595 hospitalizations of the 3321 veterans. Palliative care patients averaged approximately 2.2 hospitalizations over the study period compared to 2.0 for usual care patients (p = 0.004). We did not find any differences in the results when we restricted the analysis to the first hospitalization for all patients. Hospital and ICU LOS stay were significantly longer for palliative care patients compared to usual care but a significantly smaller proportion of palliative care hospitalizations included an ICU stay.
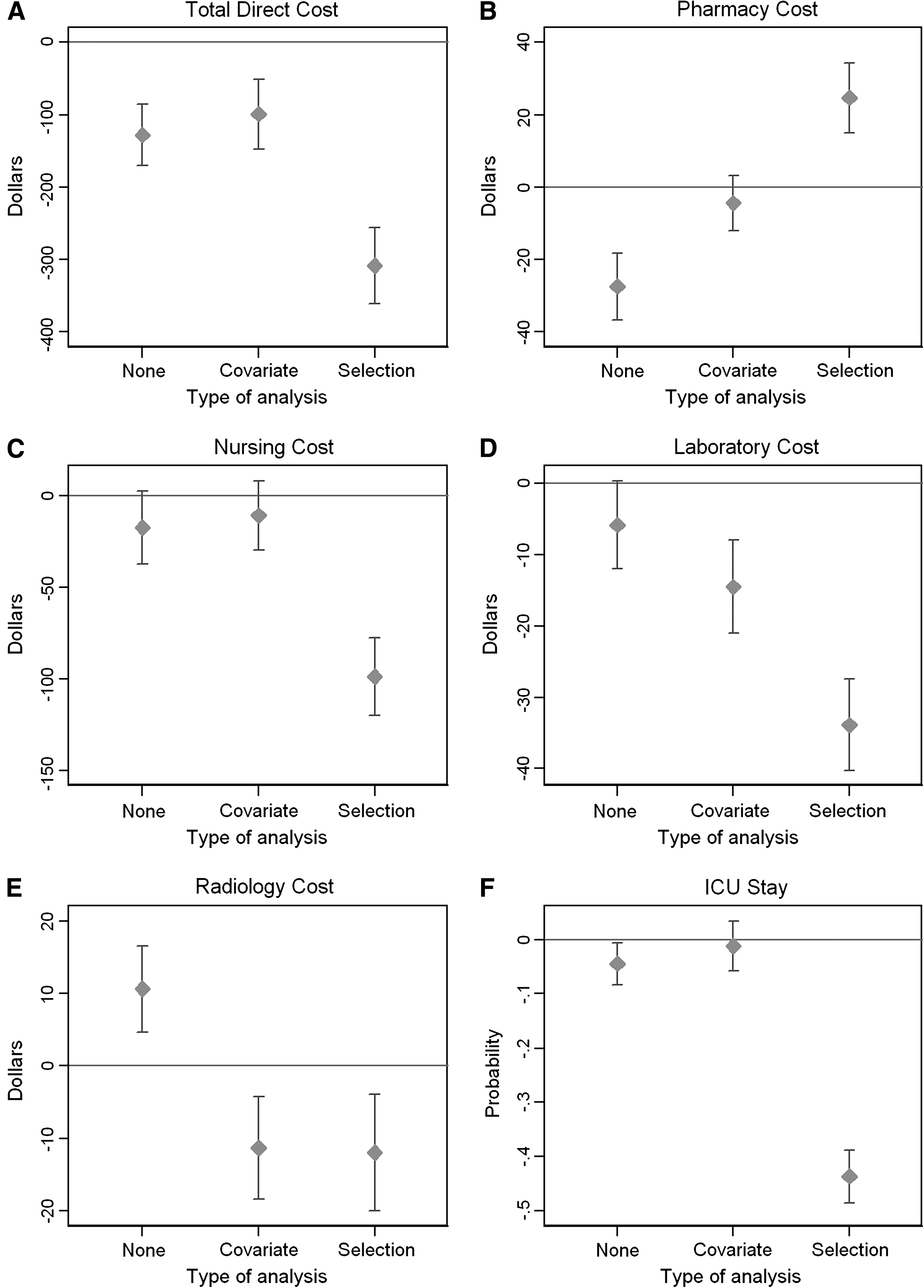
The results from the unadjusted, standard regression analyses with covariate adjustment and instrumental variables analyses are shown in Figure 1. Both the standard and instrumental variables models controlled for advanced disease conditions, age, whether the patient was married, race, whether the subject was Hispanic, principal diagnosis for the stay (infection, cancer, cardiac, pulmonary, gastrointestinal, or genitourinary), comorbidities, death before end of the study period, days between discharge and death, enrollment priority group, hospital and ICU LOS and site. Adjusted costs for hospitalizations for palliative care patients with advanced disease were significantly lower than costs for hospitalizations for usual care patients with advanced disease. Specifically, hospital daily total direct, pharmacy, nursing, laboratory, and radiology costs were $464 (95% confidence interval [CI], $515 to $413), $51 (95% CI, $60 to $43), $182 (95% CI, $201 to $164), $49 (95% CI, $57 to $41) and $11 (95% CI, $19 to $3) lower, respectively, for patients receiving palliative compared to usual care. Palliative care patients were 43.7 percentage points (95% CI, 48.6% to 38.8%) less likely to be admitted to ICU during the hospitalization than usual care patients. Except for radiology costs, the impact of selection on unobserved risk factors on each cost measure was significant and substantial.
Difference in cost for (
Discussion
Palliative care during hospitalizations for advanced disease was associated with significantly lower direct hospital costs, including costs for pharmacy, nursing, laboratory, and radiology compared to costs for usual care patients with advanced disease. Our findings are consistent with a recent multicenter randomized controlled trial (RCT) showing that patients with life-limiting illness randomized to an inpatient palliative care service had fewer ICU admissions on readmissions and lower costs compared to patients randomized to usual hospital care. 42 Our results also fit with a large multicenter observational study by Morrison and colleagues 43 demonstrating significantly lower overall hospital, ICU, and laboratory costs for patients receiving palliative care consultation compared to propensity score matched usual care patients.
This is the first study of palliative care costs to use an instrumental variables approach. Instrumental variable methods are becoming increasingly useful to answer health services questions not amenable to randomized controlled trials to account for unmeasured selection into treatment bias. Such biases in observational studies can be substantial and instrumental variable methods are better than standard analyses. 23 Thus, our finding of cost savings lends additional credibility to similar findings in the literature that did not account for unmeasured selection. Moreover, the magnitude of the effect on cost savings from our study is likely to be more accurate.
The impact of differences in the separate effects of the covariate adjustment and the selection adjustment are informative. Because palliative care may lead to use of more pain and other palliative medications, the covariate adjustment for pharmacy costs is higher then the unadjusted average. In contrast, radiology costs were not impacted by selection and the covariate adjustment captures the entire difference. The results for all the other measured factors were the same. Covariate adjustment had no effect while the selection effect was large, significant, and negative, as we initially hypothesized.
We think it likely that palliative care consultation during an inpatient stay for advanced disease influences costs, in part, through the focus of palliative care providers on meeting with patients and/or families and the medical team to establish goals of care and treatments that are concordant with the goals, including lower intensity treatments. Indirect evidence for this is the lower laboratory and radiologic testing and decreased use of the ICU for patients receiving palliative care consultation. This is consistent with a recent study of the clinical and economic impact of palliative care consultation reporting that 88% of 304 referrals were for “end-of-life decision-making.” 44 Some of the decisions made by these patients/families and the palliative and primary care teams included lower intensity treatment, discharge home for 35% and to home-based or nursing home hospice for 27% of patients. 44 Palliative care consultation teams work with patients/families to establish treatment goals and review currents treatments with those goals in mind. This frequently leads to decisions to discontinue treatments or tests that do not meet the newly established goals. 43
The study has several limitations. The data are not derived from an RCT and thus, the results may be due to unmeasured differences between the groups not captured by the instrumental variable approach. However, we established advanced disease criteria to obtain our sample so that patients would have specific advanced diseases appropriate for palliative care. Most importantly, we used instrumental variable estimation and the model to address selection bias performed well. Finally, our data are from a VA network with a well-organized palliative care program with relatively consistent operating parameters. Thus, the results may not generalize to newly established palliative care teams and/or less organized palliative care programs. Intervention studies may need to be conducted to test how sensitive these results are to the methods and sustainability of palliative care introduction.
In conclusion, this study adds to prior research on the benefits of palliative care consultation by showing that palliative care is associated with substantial reductions in hospital costs of patients with serious, life-limiting illness, a growing proportion of admissions. The findings provide support for expansion of hospital-based palliative care consultation teams. Effective palliative care programs can make a big difference in hospital financial performance.
Footnotes
Acknowledgments
Funding for this study came from the Department Of Veteran Affairs, Health Services Research and Development Service (grant # IAD-06-060-2). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Author Disclosure Statement
No competing financial interests exist.