
Abstract
Abstract
Background:
The need for palliative and end-of-life care (PEOLC) education in prelicensure education has been identified. PEOLC requires effective collaborative teamwork. The competencies required for effective collaborative teamwork are only now emerging and methods to evaluate them must be developed.
Objective:
The adaptation of the traditional Objective Structured Clinical Examination (OSCE) for assessment of a student team addressing palliative care issues was undertaken. The McMaster-Ottawa Team Observed Structured Clinical Encounter (TOSCE) is intended as a formative evaluation tool for both competencies in interprofessional collaboration for patient-centered practice and PEOLC.
Methods:
Three stations based on palliative care scenarios were developed. From January 2007 to January 2008, a total of 141 students and 38 observers participated in the evaluation of three stations, with 6–7 students per group and two observers per station. Observers completed checklists for both PEOLC and interprofessional collaborative competencies and, after completing the TOSCEs, students and observers completed questionnaires on their feasibility and acceptability.
Results:
Eighty-nine percent of the students and 44% of the observers were from medicine. Students and observers found the TOSCE to be an acceptable and feasible assessment tool for both sets of competencies. Reliability and validity data show that the items in both the clinical and interprofessional checklists fit well together, and interrater reliability is readily achieved.
Conclusions:
The new formative evaluation TOSCE tool, adapted from the traditional OSCE, was acceptable and feasible to students and observers.
Introduction
Both PEOLC competencies and interprofessional collaboration practice competencies need to be integrated into all health care professionals' education.4–9 Health Canada funded a national 3-year project, Educating Future Physicians in Palliative and End-of-life Care (EFPPEC) 10 to enhance medical students' education. It sparked curricular reform and interest in PEOLC at academic health science programs across the country. The local EFPPEC committees at McMaster University and the University of Ottawa responded by creating new palliative care curricula. The work done at McMaster University led to the recently implemented, mandatory palliative care curriculum for medical students in their family medicine clerkship program. The University of Ottawa's academic interprofessional group has also developed a mandatory palliative care curriculum for medicine. Thus, both schools needed to develop tools to assess students' competencies in palliative care and in their abilities to work as a team. A literature review revealed a paucity of reliable, validated interprofessional education (IPE) evaluation methodologies for learners, regardless of the health care content area being assessed. The McMaster-Ottawa Team Observed Structured Clinical Encounter (TOSCE) was developed as a methodology for teams of students using palliative care scenarios as a formative evaluation experience, assessing both palliative care and interprofessional collaboration competencies.
This article reports on the piloting of the three stations with interprofessional prelicensure students, January 2007 to January 2008.
OSCE Adaptations for Team Assessment in the Literature
The traditional Objective Structured Clinical Examination (OSCE) developed by Harden 11 in 1974 is recognized as a reliable and valid performance based-assessment tool, sufficiently rigorous to use in certifying and licensing examinations for health professionals. 12 The OSCE assesses the learner's ability to show that he/she knows how to address the issues presented in the examination station, requiring a behavioral and cognitive demonstration of competence (level 3 of Miller's Pyramid of Clinical Competence). 13 The OSCE also has an important role in formative evaluation. ‘Teaching OSCEs’ have been well received by learners14–17 who consistently report that they value feedback provided by observers/assessors after completing the stations.
Singleton et al. 18 used an OSCE format to assess teams of third-year medical students, dividing tasks for each member of the team of students rather than focusing on collaboration and teamwork. They found it useful as a formative assessment tool and it enabled a limited number of staff at a clinic to assess a relatively large number of medical students who were completing a clinical placement.
Using an OSCE format to assess teamwork and interprofessional competencies is more recent, Cullen et al. 19 developed an IPE program for midwifery and medical students at the University of Nottingham. Using the OSCE format, teams of 6–8 medical and midwifery students experienced a series of five Interprofessional Team OSCE stations (ITOSCEs), based on complicated labor scenarios. 20 A facilitator from a variety of relevant disciplines, provided 5 minutes of formative feedback using a checklist as a guide. Resource implications were significant. The authors also noted the importance of activities to facilitate team building before students start the ITOSCE, recommending interactive workshops led by an interprofessional group of faculty.
Morison and Stewart 21 developed an 8-week pediatric educational program for fourth-year medical students and third-year nursing students, which included a role play with “parents” of an ill child and a team task to complete at the end of the placement. A traditional OSCE station assessed students' skills common to both professions. The student team was assessed by three interprofessional observers, during the role play acted by senior house officers. A checklist assessed each student's ability to provide quality information, to communicate effectively, and to demonstrate knowledge of professional team roles and teamwork. This format successfully demonstrated the assessment of more than one student from two different professions as well as the ability of an interprofessional team of assessors to work together to determine a standard that applied to both professions. Gaps in students' knowledge were identified through the role play, and the assessors felt able to differentiate between effective student teams and a “team” that was simply a collection of individuals.
Other studies have successfully used interprofessional faculty as observers/assessors15,22 or have received positive feedback from both students and faculty for stations that incorporate another discipline/profession as a standardized role.17,23
The studies above have two things in common: the importance of involving an interprofessional team representative of the clinical area being tested; and the importance of the feedback session for the learners following the station.
Development of the McMaster-Ottawa TOSCE
The EFPPEC committees at both universities began this joint initiative in 2005. The two schools agreed to focus on the core competencies identified through the national EFPPEC Palliative Care Competencies document 2006. 10 The competencies corresponded to palliative care curriculum and required a collaborative patient-centered team approach. Core interprofessional collaborative practice competencies were articulated and implemented at both schools based on the emerging literature and national/international experience regarding basic prelicensure competencies in interprofessionalism for health care students.24–27 Based on their current educational experiences and literature review, the McMaster-Ottawa team agreed there was value in adapting the OSCE format to become a tool that could assess team function on complex health care problems requiring a team response. To emphasize the formative nature of the tool, it was named the TOSCE, removing the formal connotations of “objective” and “examination.” Three stations were created. The Observer Score Sheets followed the format of the traditional OSCE, and included subject content and the team's agreed-upon core interprofessional collaborative competencies.
The scenarios
The TOSCE stations were based on guidelines for OSCE stations 11 and were representative of common clinical experiences in palliative care where team work was particularly important. In stations requiring patient/family interactions, the roles were played either by standardized patients (SP) or by palliative care staff and faculty. Each scenario was designed as a 30-minute station:
1. Suffering: The student team must discuss an approach to the care of Neil, a young patient who is suffering physically, psychologically, socially, and spiritually and is requesting assistance to die. Neil is presented through a video clip viewed by all the team members. Each member then receives a different excerpt of the patient's monologue for additional insight into the multiple dimensions of his suffering. They must effectively share what they know about Neil to develop an approach to address his suffering;
2. Pain: The student team must meet and interview Sue, a woman with metastatic breast cancer, presenting with uncontrolled pain. Sue is played by an SP.
3. Cross-cultural communication: The student team has requested a family meeting with Mrs. Zeibarth and her adult child, both played by SPs. The team wants to discuss the results of the mother's biopsy that will confirm a malignancy has been found. The daughter insists on meeting the team before they meet with her mother to emphasize that the bad news must be broken with cultural sensitivity, respecting the norms of this family.
The TOSCE Process
Observers
Two observers, one physician and one nurse or other nonphysician health professional, were recruited from the palliative care and interprofessional faculty at each university for each of the three stations. Observers were provided with a 2-hour teaching orientation to the TOSCE and the Observer Score Sheet.
Methods
Prior to the TOSCE experience, students were provided with a 20- to 30-minute orientation. Each station was scheduled for 30 minutes, followed by 10 minutes for feedback. When prepared, the student team and observers assembled in the meeting/examination room, and the SPs (if needed for the scenario) waited outside the room for the students to initiate interaction with them. Similar to the traditional OSCE, the student team received the instruction sheet, which briefly introduced the clinical scenario. If the station required a patient encounter (e.g., inviting the SP(s) into the room; viewing a video clip), the team was expected to first strategize its approach to the patient scenario before proceeding.
Medical students doing their 6-week clinical clerkship in family medicine participated in the pilot. Students from other health sciences programs were invited to participate on a voluntary basis. Given this limitation, students could choose to act as team members from their own profession or to role play another profession. They also decided what kind of health care team they would be (i.e., acute care team, homecare team). They were expected to make these decisions as soon as they had read the scenario. If requested, the observers would keep track of time and alert the team when 5 minutes remained in the session. The students were expected to end the interview/team discussion appropriately and to finalize their plans. After the observation and for approximately 10 minutes, the observers and SP, if present, provided individual and group feedback. The student teams rotated through three TOSCE stations over a 3-hour period. The observers also completed their scoring for the individuals and groups after each station.
Student evaluation and feedback
A standardized McMaster-Ottawa TOSCE Observer Score Sheet was developed for each station, based on the core interprofessional collaboration competencies and the specific set of palliative care competencies being addressed. This score sheet included a checklist in table format with a column for each student, where the observer could comment and record if a competency was addressed or not. Each observer also gave each student and the team as a whole an overall global numerical score based on the guidelines provided on the same page. The score sheets served as a basis for constructive feedback to individuals and teams.
Evaluation Methods
Research Ethics Boards at both institutions approved a formal evaluation of these sessions. The evaluation consisted of questionnaires for students and observers assessing their satisfaction with the process and their perceptions of the overall acceptability and feasibility of the TOSCE and asking for additional comments. Students had 19 five-point Likert scale statements (1 = strongly agree, and 5 = strongly disagree) and observers had 21 statements. These questionnaires were completed at the end of each TOSCE session. The questionnaires were developed specifically for this program evaluation and were not piloted.
Results
Psychometric testing demonstrated validity and reliability. A total of 158 students participated, and each station was observed by two observers. Interrater reliability was 0.916, and internal consistency for the IPE scales (checklists) of the three stations ranged from 0.725 to 0.865 for both observers. These results show that the IPE and clinical scales seem to fit together conceptually for this sample. Correlation between the two observers for the teams' global scores for all three stations combined was very good at 0.844.
Between January 2007 and January 2008, nine half-day TOSCE sessions with three separate groups were held at McMaster to pilot the three stations. In Ottawa, one group of volunteer students was recruited from the University of Ottawa and Saint Paul University (responsible for the training of counselors in spiritual care) for one half-day to pilot the same three stations. Of the 158 students who participated; 141 agreed to complete the evaluation. The professions of participants and observers are listed in Table 1. Medicine had the highest number of participants: 89.4% of students; 44.7% of observers.
University of Ottawa or Saint Paul University, Ottawa, Ontario, Canada.
TOSCE, Team Observed Structured Clinical Encounter.
The majority rated the stations as fair (73.0% agreed or strongly agreed, n = 141) and manageable (81.8%). Approximately half (43.3%) agreed that the stations were appropriate for demonstrating their knowledge and skills, and 46.1% agreed that the interprofessional student mix was manageable (Figs. 1 and 2). Additionally, a majority agreed that the TOSCEs allowed them to demonstrate: their professional skills (73.75%, n = 133); shared decision making (72.8%, n = 136); and key elements of collaboration (65.2%, n = 135). Many agreed they could articulate appreciation of other professions (71.8%, n = 135), and discuss interprofessional collaboration (IPC) as a key part of the care plan (76.9%, n = 134). Analysis of their written comments on the evaluation forms indicated the 10-minute feedback portions of the TOSCEs were both informative and highly relevant to their learning, and that they had learned about palliative end-of-life care and interprofessional collaboration through the TOSCE experience.
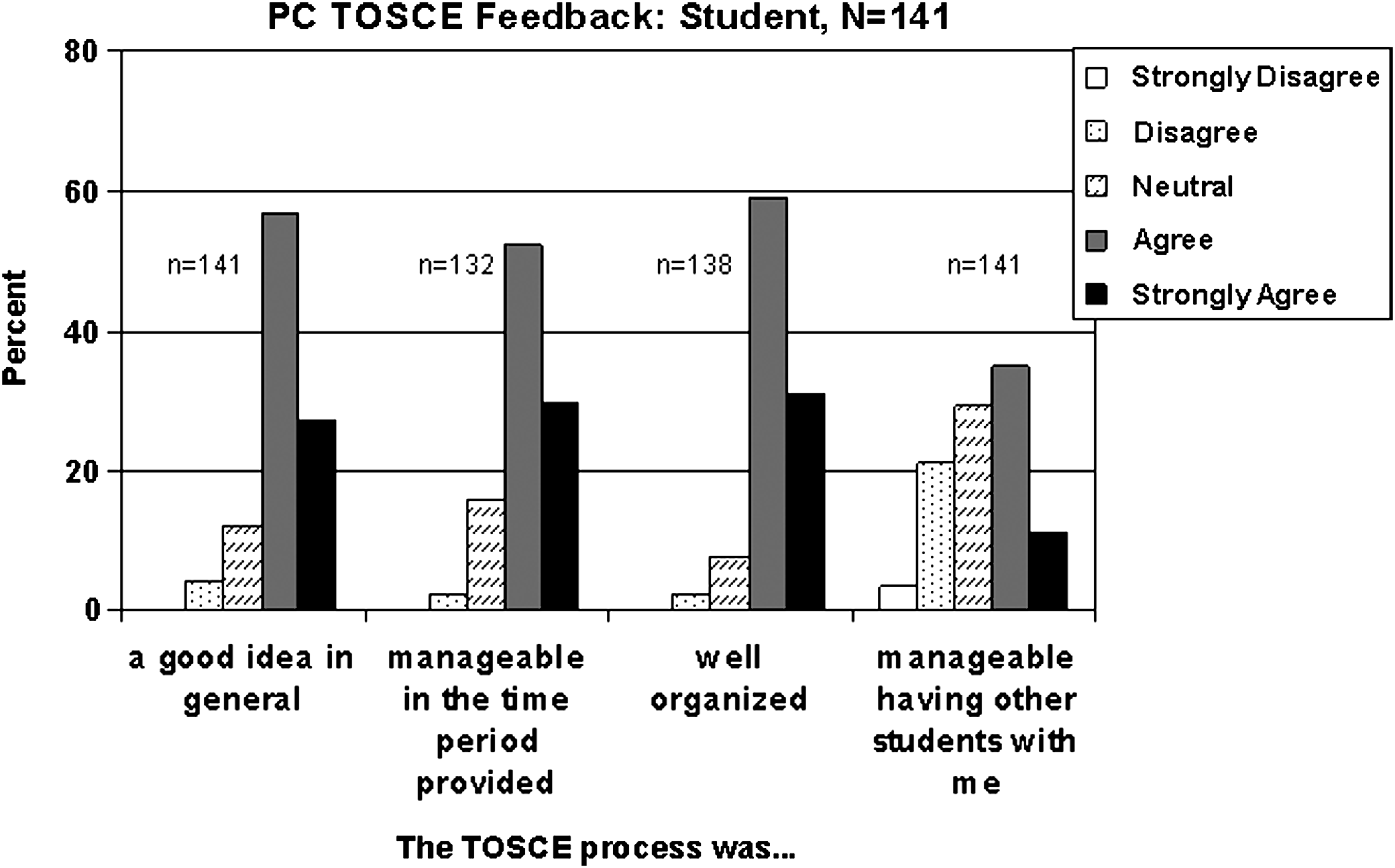
Selected student ratings of the process of the McMaster-Ottawa Team Observed Structured Clinical Encounter.
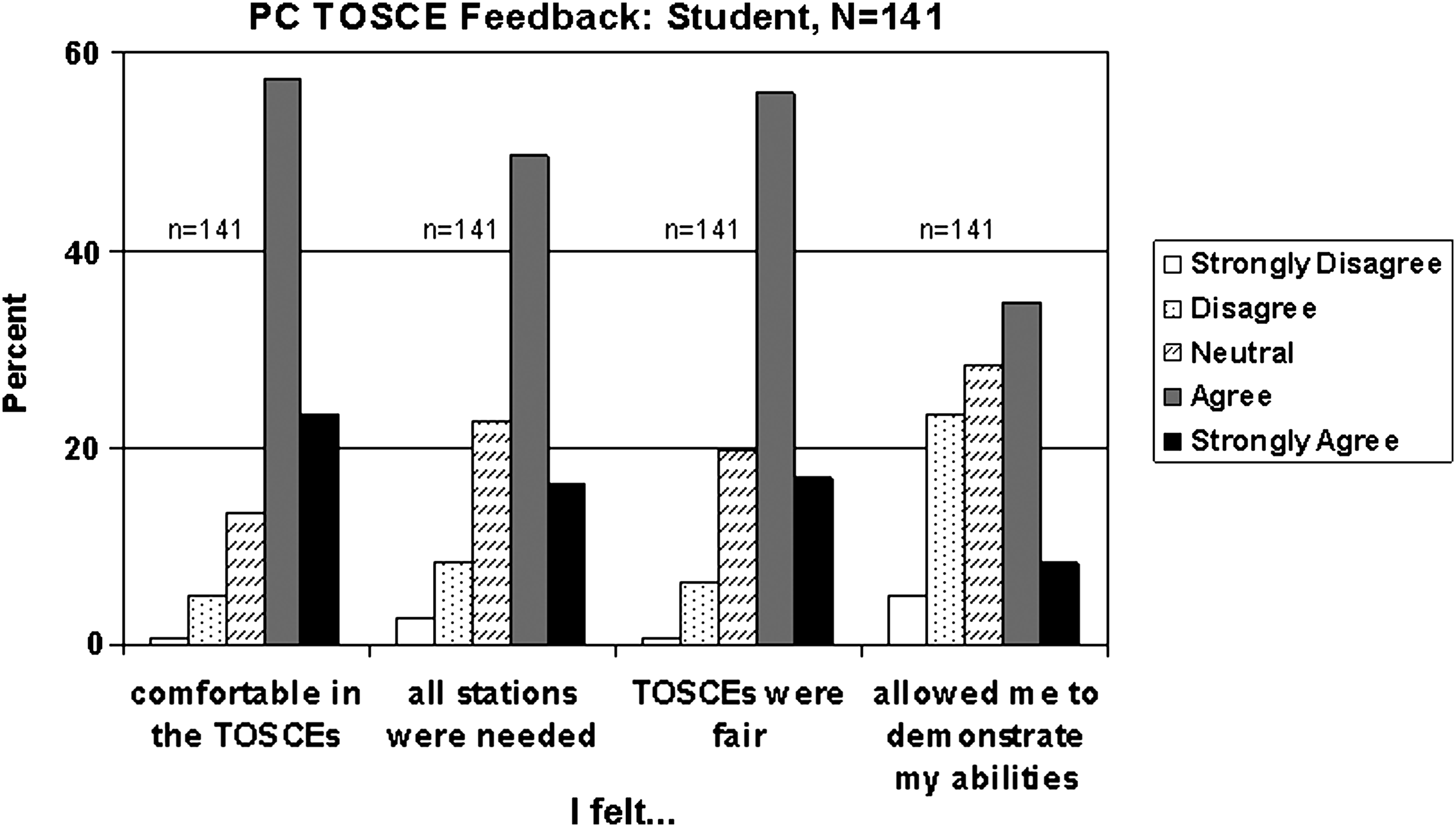
Selected student ratings of the acceptability of the McMaster-Ottawa Team Observed Structured Clinical Encounter.
Of the 38 observers who answered the questions, all rated the TOSCEs as a good idea (100%, n = 35) and inline with their expectations (75.8%, n = 33). Most (82.6%, n = 23) agreed it was manageable to assess students from differing professions, and many (63.4%, n = 30) agreed it was reasonable to assess more than one student at a time. In total, 43.8% (n = 32) agreed they were able to assess students' abilities in an appropriate manner (Fig. 3). Also, most agreed that the TOSCEs allowed students to demonstrate: their professional skills (66.6%, n = 30); shared decision-making (80.6%, n = 31); and key elements of collaboration (73.4%, n = 30). Most agreed the students could articulate appreciation of other professions (73.4%, n = 30), and discuss IPC as a key part of the care plan (67.8%, n = 30). From their written comments, observers noted the main limitation for this study was the lack of interprofessional student mix.
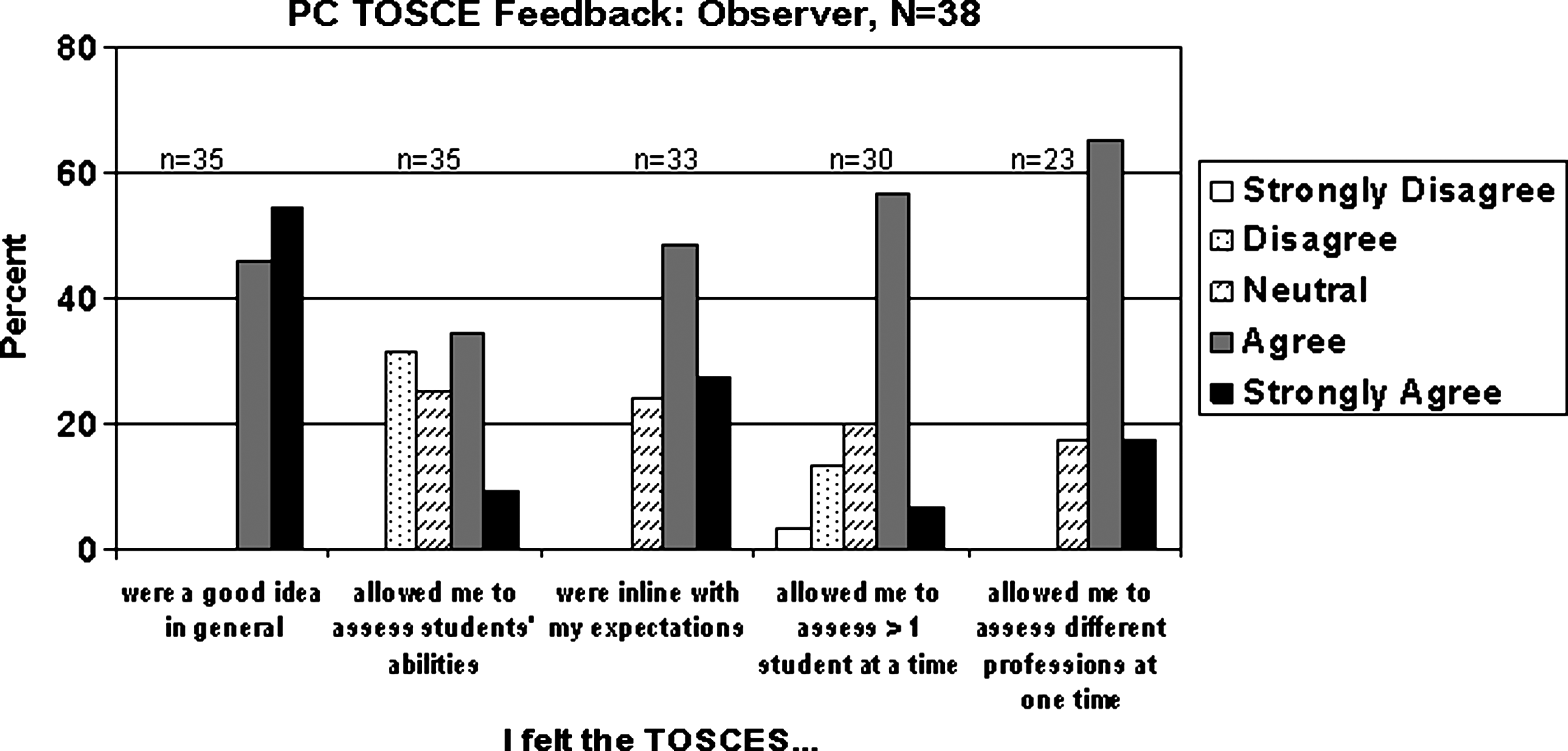
Selected observer ratings of McMaster-Ottawa Team Observed Structured Clinical Encounter (TOSCE) experience.
Limitations
This pilot study was integrated into the regular clinical clerk rotation in family medicine for medical students at McMaster University. Due to scheduling challenges, students from other professions participated voluntarily. The results mainly reflect the feedback of medical students and cannot be generalized to other professions. Assessing medical students as they play roles of other professions is questionable, although the experience may be educational. The interprofessional competencies used in the pilot study were precursors of the recently published national collaborative competencies and, thus, limit any generalizations. This pilot consists of only three stations, which is likely an insufficient number to show appropriate validity and reliability.
Discussion
In our initial publication, students reported finding the McMaster-Ottawa TOSCE format acceptable and feasible. 28 The results of this trial demonstrate that students and observers recognized the potential of this assessment tool for both teamwork and palliative care competencies. These results correspond with Cullen, 19 Symonds, 20 and Morison and Stewart 21 who reported that students found the interprofessional TOSCE format promoted a team attitude toward problem management, a useful skill for intraprofessional and interprofessional teamwork.
Despite the lack of students from professions other than medicine in this pilot evaluation, the potential for IPE was recognized. Some compensated for the lack of diversity by role-playing other professions or discussing how they planned to incorporate other health care professionals into the care plan. Often, this served to highlight gaps in their knowledge of the roles of other health care professionals, and the feedback sessions helped address these deficits. Assessing the clinical skills of students playing a different role is questionable; however the role-playing would still allow observers to assess interprofessional competencies.
Students' poorer ratings for the TOSCE to be manageable with other students (Fig. 1) may be reflective of the lack of students from professions other than medicine. Both students and observers rated the TOSCE as not quite able to allow them to demonstrate their abilities. This is consistent with findings that indicate more than three stations are required to fully observe students' competencies.
For student groups without previous opportunities to work together as a team before the TOSCE experience, an introductory session to help them form relationships may be necessary to facilitate the forming stage of group development. 29 Recognizing this fact, it remains appropriate for groups with little or no experience as a team to come together for the TOSCE, as this mirrors the real world where teams need to form spontaneously around emerging patient care needs without the luxury of team-building exercises. For students, the introductory session may alleviate some stress and provide them with a better learning environment.
The value of the feedback portion of the TOSCE, highlighted by participants, reflects the positive effect of formative feedback in the teaching OSCE format described by others.14,15,17,19–22 As a result of this information, we have extended the time available for feedback from 10 to 20 minutes, depending on the needs of the learner team.
Our ongoing experience suggests that these TOSCEs can be used for a variety of purposes. It appears to be a useful formative learning experience for an interprofessional group of learners who wish to assess and enhance their competencies in both palliative care and team functioning. This may apply to uniprofessional groups of learners. Reliability and validity data suggests that the TOSCEs may emerge as a useful summative evaluation methodology as well.
From the perspective of curriculum planning, resource requirements for running TOSCEs bear comment. In our experience, scheduling a half-day session of 3 hours regularly has been an efficient way to manage limited resources. Faculty development for observers is key, and the role of “observer” has emerged as a new teaching role with a dedicated group of interprofessional faculty and clinicians who enjoy this particular opportunity. TOSCE organizers need to bring together small groups of learners (ideally four to six in each group), with one to two interprofessional observers. Scheduling in advance is helpful. Separate rooms are required for faculty development (if done just before the TOSCE event) and for each group that is being run at the same time. The observers' job is complex and reiterates the need for training and preparation. A trained faculty to draw upon would maintain the quality of the observations year after year.
Addressing the scheduling realities of a variety of students and faculty across professional programs remains a challenge for all IPE initiatives. 1 For the McMaster-Ottawa TOSCE to become a standardized evaluation tool for students in several faculties across our institutions, it will be necessary to share resources and to have the events centrally supported.
Future Directions
Since this pilot, four additional palliative care stations have been developed and are being used by the McMaster-Ottawa palliative care educators. These scenarios focus on: dyspnea in a community setting; loss and bereavement issues; advance directives; delirium in a palliative patient.
Although the best available evidence was incorporated into this pilot,24,25,30 a consensus on the competencies necessary for effective patient-centered collaborative team work has just emerged, 31 and the Observer Score Sheet is being modified accordingly.
The McMaster-Ottawa TOSCE work group has also developed, piloted, and evaluated 10 stations for practicing primary health care teams (i.e., not students), using complex care scenarios common to primary care. The evaluation of these stations demonstrated that they are a reliable methodology for both formative and summative purposes for collaborative team competencies. 32
Thus, the McMaster-Ottawa TOSCEs hold promise for future development around discipline specific content areas, knowing that the team competencies evaluation portion can be imported into new station development.
Conclusions
The evaluation of the initial pilot project of three palliative care case scenarios, based on the national EFFPEC and emerging interprofessional competencies, demonstrated the feasibility and acceptability of using the McMaster-Ottawa TOSCE as a formative evaluation tool. Our ongoing use and development of more stations has ensured that the TOSCE is an integral part of our curricula.
As each professional school develops IPE curricula and as collaborative practice becomes the norm of care, the logistics of organizing interprofessional evaluation processes will need to be addressed. Many different IPE evaluation strategies are needed, and the McMaster-Ottawa TOSCE is emerging as a useful methodology.
Footnotes
Acknowledgments
We are grateful to the following for their participation and support: Peter Barnes, Lynn Casimiro, Susan Brajtman, Meridith Marks, Sue Humphreys, Luanne Waddel, Beckie Tingley, Clareen Akshinthala, Diane Gauthier, Kevin Eva, students and standardized patients, and to Jo-Anne Dusseault and Enkenyelesh Bekele for their editorial assistance. The project was supported through the financial contributions of the University of Ottawa Award of Excellence and the Health Canada EFPPEC Project.
Author Disclosure Statement
No competing financial interests exist.