
Abstract
Abstract
Background:
Families of patients with advanced dementia need to be informed about the course of the dementia and comfort care. Conditional for health care providers educating families is their knowledge and comfort in family education.
Methods:
Perceived usefulness and acceptability of a Canadian family booklet explaining possible complications and comfort care in dementia was assessed by physicians and nurses caring for dementia patients in 14 nursing homes in Lombardy, Italy and 21 in the Netherlands. The practitioners received a questionnaire and translated versions adapted to local practice where needed. In 10 of 21 Dutch homes, physicians evaluated only the original Canadian version in English. A 15-item scale assessed the booklet's acceptability, for example, to inform families, or for educational purposes. Perceived usefulness referred to proportion of families of dementia patients for whom the booklet would be useful. A total of 168 evaluations were available for multivariable regression analyses.
Results:
The practitioners anticipated that the booklet would be useful for most families. Evaluation of the Dutch translation of the booklet was similar to the English version. Country (Netherlands) and profession (nurses) were independently associated with better acceptability. Usefulness was perceived as better by Italian respondents and nurses, but only in analyses unadjusted for the higher educational needs of these respondents.
Conclusion:
Overall, the concept of written information on comfort care was appreciated by practitioners of European countries differing in attitudes toward end-of-life care. A booklet may help practitioners, and in particular nurses, in providing comfort care for dementia patients and their families.
Introduction
Several studies in long-term care settings identified strong educational needs regarding end-of-life issues among families of dementia patients.5–9 Although this is an understudied area, in most studies on cancer patients' satisfaction with care, the information provided by medical staff about illness and treatment was important. 10 Moreover, studies have shown that with progression of the disease, patients' wishes for information may decrease, whereas families may wish for more. 11
Providing families serving as proxy decision makers with information on end-of-life issues may be a particularly sensitive issue. Families may feel guilty about their relative's admission to long-term care and suffer from pre-grief with disease progression.7,12–15 Therefore, conditional for health care providers educating families is not only having access to provide sensitive information, but also feeling comfortable in doing so. In previous work, physicians' intentions to use a decision aid were related to their comfort with offering it to patients. 16 Further, a similar booklet was withheld in some cases because staff opposed it. 8 In general, attitude is a well-studied factor that determines use of clinical guidelines. 17
The different roles physicians and nurses have in decision making and care may affect how they educate families. Physicians may focus on decision making, and nurses on the end-of-life experience. 18 Further, families frequently consult with nurses about prognosis because they see families often. 19 In a community study, most families of dementia patients wished to receive information from a practitioner, backed up by written information. 20
To educate families of nursing home residents with dementia on comfort care, a booklet has been developed for use in Canada with substantial input from families and experts. 21 It has been translated in Italian, Dutch, and Japanese. While upholding core issues about comfort care, it required adaption to local cultural, ethical, and legal standards. We evaluated the booklet with clinicians practicing in nursing homes, physicians and nurses in a northern and southern European country, assessing perceptions of usefulness and acceptability of the family booklet. We also examined if profession, country, or other respondent characteristics were related to respondents' perceptions of the booklet.
Methods
The booklet
The original Canadian booklet was developed in English and French, and based on qualitative study of decision making in dementia with input from families,22,23 literature, and expert opinion. It has been accepted as best practice by WHO. 24 The booklet informs on the course of the dementia, expected complications, decision making (e.g., regarding antibiotics and feeding tubes), comfort care, and dying and grief (Fig. 1). It differs from the regular decision aid in that its main goals are not neutral in terms of presentation of treatment options or eliciting of individual preferences. 25 By contrast, it was based on consensus that, at least for end-stage dementia,1,2 comfort/palliative care is best practice. More adaptations regarding contents and style of the booklet were made in the Dutch version. Most adaptations were minor, to better suit Dutch language style. Further, adaptations were made to conform with Dutch law on, for example, representing patients, and we expanded on palliative sedation and euthanasia. In the Italian version, the layout including colors and photographs was modified.
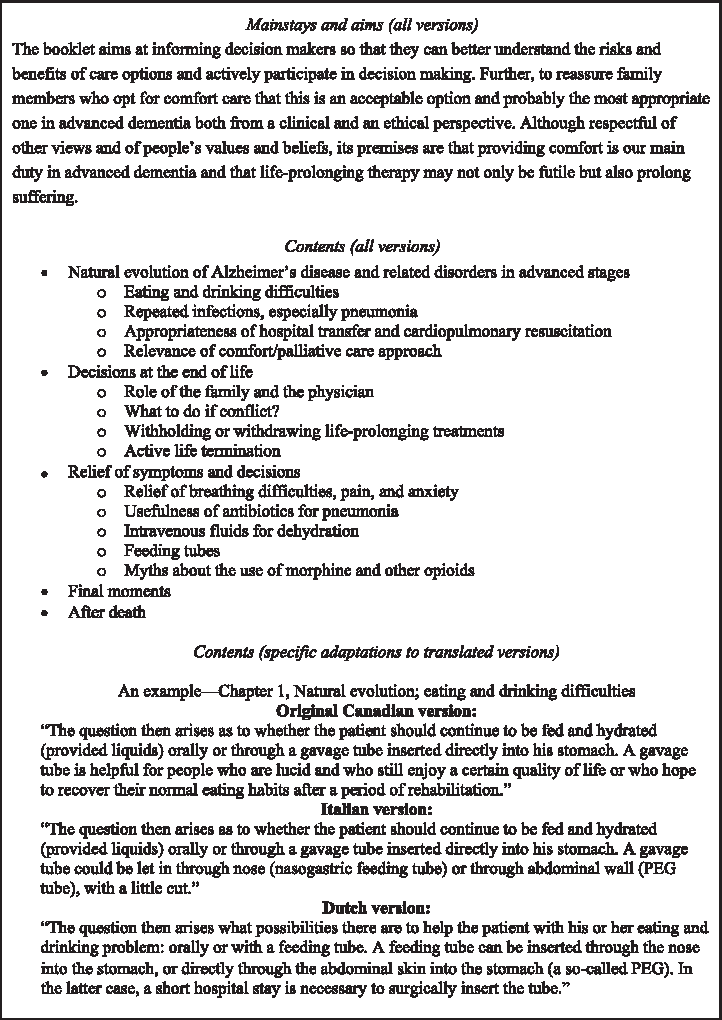
Contents and format of the booklet, “Comfort Care at the End of Life for Persons with Alzheimer's Disease or Other Degenerative Diseases of the Brain.”
Design of the evaluation study
Randomized trials or before-after study designs are recommended to evaluate decision aids. 26 However, because of the sensitive issues (e.g., guidelines regarded as controversial are half as likely to be followed) 17 and acceptability unknown in other cultures, an implementation study was regarded as more appropriate than an intervention study. Further, the importance of practitioners' roles in providing it was unclear, and criteria for aids require evidence of acceptability among practitioners. 25
To examine magnitude and direction of possible effects of different local adaptations, we compared the original English version from Canada with the Dutch version that was revised most extensively. Some Dutch physician respondents, who are generally capable of reading and understanding English, evaluated the original version blinded to the Dutch version. We provided four copies of the translated booklet to each practitioner relevant to intention to use the booklet.
Data collection occured between April 2009 and January 2010 in the Netherlands, and May and November 2009 in Italy. Physicians were on-staff. Fourteen nursing homes in Italy were recruited from a stratified sample of homes that participated in a prospective study and that was representative of the Lombardia region. All (100%) of invited practitioners returned the questionnaire. Dutch nursing homes were recruited via the university networks of homes and supplemented purposefully for a balanced geographical and urban-rural distribution across the country. Dutch procedures included at least two reminders (phone or e-mail) when unresponsive. We invited 25 Dutch homes to participate, and 21 (84%) agreed. Response rates were 70% to 76% per group.
Instrument for evaluation
A survey questionnaire was developed in English by the research team, and pilot-tested in Canada. Local national teams translated the instrument and it was back-translated by a professional translator. The back translations were evaluated by two team members (JTS and MA). The survey questionnaire was partly the same as for families 27 and addressed relevant user-centred concepts in study of information behaviors of caregiving in dementia 28 by, for example, the possibility to indicate preferred time to receive the booklet including open-ended options.
Acceptability has been referred to by O'Connor and Cranney 29 as “ratings regarding the comprehensibility of components of a decision aid, its length, amount of information, balance in presentation of information about options, and overall suitability for decision making.” Our main outcome measure “acceptability” refers more specifically to acceptability for informing families and supporting decision making, two main goals of the booklet. It further includes the themes communication with families, satisfaction with care, use in practice, and use in training. For this, we developed a 15-item scale summing rating of agreement with statements selected from the acceptability instrument by O'Connor and Cranney 29 and from a comparative evaluation of three decision aids, including on tube feeding in dementia evaluated by geriatricians (Graham et al.). 16 For the acceptability scale, we did not select items related to the categories of “development” because they did not apply to the adaptation process, or “content and format,” which was addressed with other measures, 29 but we selected from “meeting patients' need” and items “related to clinical practice.”
Item scores were 1 to 5 with extremes labelled “strongly disagree” and “strongly agree.”16,29 Higher total scores represent better acceptability. We regarded scores of 45 and higher as “acceptable” and 60 and higher as “highly acceptable” (mean item scores 3 and 4, respectively). The scales' validity and reliability were adequate and the concept addressed was rather homogeneous. Correlation with a 0–10 numerical rating scale for the booklet's overall evaluation with endpoints “not at all useful” and “extremely useful” was +0.68 (p < 0.001). Further, Cronbach's α was 0.93, which was just within the upper limit of 0.95 with higher values indicating redundancy. 30 Principal component factor analyses extracted a single main factor explaining 51% of variance, other factors explaining only 9% or less. Loadings between items and the main factor varied between 0.53 and 0.83. Properties were similar for nurses and physicians, and for the countries.
Perceived usefulness to families was assessed as proportion of families for which the booklet will be useful. Response options were: all families of dementia patients, the majority, about half, a minority, and not any family. This item correlated significantly with the numerical rating scale on overall usefulness (+0.22; p = 0.005).
The quality of the information overall was rated on a scale from 1 (poor) to 5 (excellent). We further used evaluation of amount of information, 29 intention to use, and need for a booklet. 16 We assessed preferences as to whom should provide it. We also assessed respondents' characteristics potentially affecting evaluations, such as experience 31 and religion, which may influence an individual's comfort in discussing comfort care. 32
Analyses: Descriptive and regression
Data were entered in the local study sites in EpiData (version 3.1, EpiData Association, Denmark, 2008). Double entry of 8% of Italian and Dutch records showed an error rate of 0.05%. Analyses were performed in the Netherlands, with SPSS version 15.0.1 (2006) (SPSS Corp. Inc., Chicago, IL). T tests for continuous data, and χ2 tests for proportions were used to compare respondent characteristics by country, profession, and version evaluated (English versus translated). For categorical variables, Mann-Whitney U tests were used.
Linear regression was performed with the acceptability scale as the dependent, performing bivariable and multivariable generalized estimating equations (GEE) regression analyses adjusted for clustering of practitioners within institutes. Coefficients (representing difference in score) and 95% confidence intervals (CI) were calculated. We also applied this technique with proportion of usefulness to families as the outcome after examining associations and distributions, and confirming that ordinal multiple regression provided similar results.
Missing data in independent variables used for adjustment in regression analyses were fewer than 5%. Variables were imputed with overall mean or mode as appropriate. In the 15-item acceptability score, 3 missing items were allowed and imputed with respondent means, leaving a single missing case (0.6%). Four cases (2%) missed usefulness.
Results
Table 1 shows nurses' and physicians' characteristics. Nurses were predominantly female (>90% versus 58%–67%), somewhat younger, and reported providing care to fewer dying patients.
When country of origin was different, it was Romania or Poland for Italian respondents, and Croatia, United States, or Belgium for Dutch respondents.
p < 0.05 difference nurse-physician.
p < 0.05 difference between countries (nurses vs. nurses, physicians vs. physicians; translated versions).
p < 0.05 difference English vs. translated version (Dutch physicians).
Most Italian respondents reported having educational needs regarding comfort care in dementia (>90%), educational needs were identified as lowest for Dutch physicians (<50%). Italian nurses more frequently originated from other countries. The great majority of Italian respondents (85%–88%) were Catholic, whereas among Dutch respondents a substantial proportion identified themselves as Protestant. Physicians frequently reported themselves as having no religious affiliation. The majority of both Italian and Dutch respondents (51%–71%) reported that their religious orientation did not affect their evaluation of the booklet.
We found strong support for all versions. For example, the quality of the information of the booklet overall was rated favorably, the Dutch version receiving the highest marks (mean of 4.3, stand deviation [SD] 0.5, versus 4.0, SD 0.8 for the Italian, and 4.0, SD 0.8 for the English version; p = 0.03). Further, most respondents (84%–93%) endorsed that information on decisions such as tube feeding was balanced (not slanted toward comfort or life-prolonging care), although overall, Italian respondents more frequently found that information on one or more of the decisions was slanted toward comfort care (30% vs. 9%, p < 0.001).
Most respondents (96%–100%) believed that in their country, families were in need of an information brochure on comfort care and end-of-life issues in dementia. Most respondents (96%; range 83%–100% for the five groups) also believed the booklet would be useful for at least half of families. Between 90% and 94% of practitioners intended to provide the translated booklet to families in the next 3 months.
Table 2 shows that all groups found the booklet acceptable, with high acceptability for Dutch nurses, which was significantly higher than for Dutch physicians. At the level of items, Dutch nurses were more positive about “improving a shared understanding of patient's preferences,” and Italian nurses about “increased understanding of dementia” than their physician colleagues. Overall, Dutch respondents were consistently more positive about the booklet's usefulness in decision making. Use of the booklet as a teaching aid for nurses received support among Italian and Dutch physicians and nurses (item scores 3.7–4.2).
Range: 15 to 60. Themes addressed: informing families, supporting decision making, communication with families, satisfaction with care, use in practice, and use in training.
p < 0.05 difference nurse-physician.
Unadjusted for potential confounders (the variables in Table 1), profession (nurse versus physician, β+4.5, CI+1.8; +7.3) and country (Netherlands versus Italy, β +4.2, CI +0.2; +8.2) were associated with higher acceptability. Table 3 shows that adjusted scores were not lower (nurses, +5.1 points, and Dutch respondents +7.5 points). Nonnative origin was strongly and independently related to acceptability (+9.7 points).
(Significant associations (p < 0.05) are italicized.)
Acceptability scores showed a low but significant correlation with usefulness to proportion of families (+0.17, p = 0.02). Nurses as a group, and Italian respondents indicated usefulness to more families. However, in adjusted analyses, neither profession (β for nurses +0.19; −0.07; +0.45), nor country (Netherlands: −0.18, CI −0.40; +0.04) were significantly associated with usefulness. Exclusive practice in a long-term care setting was associated with lower perceived usefulness of the booklet (β −0.36, CI −0.64; −0.07). Nurses being younger accounted to some degree for nurses' more favorable evaluations. Higher educational needs (among Italian respondents and Dutch nurses versus physicians, Table 1) was strongly related to usefulness (bivariable association: β +0.47 per point on 5-point scale, CI +0.22; +0.72) and explained a large part of the differences between unadjusted and adjusted results. A cross-national difference in educational needs is also shown by Italian nurses and physicians who reported more frequently (p < 0.01) that the booklet provided too little information (17%) versus too much (1%), whereas this was the reverse for Dutch respondents (1% versus 14%, respectively). Limiting analyses to evaluations of translated versions did not essentially change results.
Most respondents favored physicians (81%–100%) and nurses (54%–86%) to provide the booklet, and almost all (93%–100%) any of the two professions. However, Dutch nurses more frequently preferred nurses over physicians to provide the booklet to families (86% versus 81%). Other disciplines, such as social workers and psychologists, were preferred by half or fewer of the respondents. Availability not through practitioners (brochure cabinet or via Internet) was a preferred option to about half (44%–57%) of respondents with no significant differences between groups.
Discussion
Families involved in care for their relatives with dementia face complexities, which ultimately go back to the question of what a good death looks like. 33 To help families address difficulties when considering the best possible quality of dying, they need guidance from a professional caregiver7,34–38 supported with written material. 20 In our study, a Canadian booklet to inform families on the course of the dementia and comfort care was evaluated by professional caregivers in two European countries.
Overall, the booklet was well received by the physicians in our study, especially by nurses. The Italian and Dutch participants found the booklet acceptable, and useful to the majority of families, regardless of adaptations made to translated versions. Other published reports of evaluations of decision aids in palliative and dementia care were also favorable.8,39,40 These findings suggest that the concept of written information about sensitive issues in end-of-life care is endorsed regardless of the precise format.
The two countries involved in our study differ widely in context regarding end-of-life issues.41–44 For example, in studies in several settings, withholding of life-sustaining treatment was more acceptable in the Netherlands.41,42 National differences in palliative care training have been noted; in Italy 35% of physicians have had formal training, which was the lowest of seven countries (Australia and six European countries), whereas the Netherlands had the highest percentage (78%). 45 In our study, Italian respondents reported higher educational needs regarding comfort care in dementia. Although found equally useful to families, Italian respondents found the booklet somewhat less acceptable. Italian physicians may prefer their own and colleagues' experience over practice guidelines; for example, only 65% endorsed that guidelines could help physicians make complex decisions, 46 and a similar critical attitude might have affected the booklet's evaluation.
Nurses' roles and attitudes differed from those of physicians in studies in different end-of-life care settings.18,47,48 Although culturally distinct from Western countries, a Japanese study found that doctors tended to take an active approach (talking), whereas nurses preferred listening and discussing of end-of-life issues. 47 In a Dutch study, only 37% of physicians agreed that an advance directive in nursing home residents with dementia should always be followed, but 88% of nurses and 88% of families agreed. 48 Ongoing evaluation of the booklet also shows that nurses' evaluations are closer to bereaved families' evaluations, and even more favorable. 27
Decision aids have effectively involved patients in decision making, 49 and this may extend to nurses. Lack of nurses' active participation in end-of-life decision making may cause moral distress. 50 The booklet may enhance nurses' role in decision making by educating them about treatment options, prognosis, and how to inform families. These are tasks traditionally within the physician's domain, but most respondents, including physicians, endorsed a role for nurses in providing the booklet, even in the two countries where physicians are on-staff at the facility, and therefore more available than in other countries. 38 The booklet may support nonnative practitioners, including nurses in particular, to overcome cultural and language barriers in communicating with families. A training program based on the booklet's contents may further support nurses. Physicians may also benefit from such training; this may promote teamwork and consensus on how to guide families, as nurses' and physicians' roles regarding informing on prognosis were unclear in recent Dutch work. 19 Further work on the booklet's use in training and implementation is particularly relevant in Italy.
The physicians and nurses almost universally endorsed a role for practitioners in providing the booklet, and so did families. 27 Physicians and nurses may prefer integration in clinical practice, or to tailor information individually. 51 This also allows for a step-wise approach that may avoid anxiety,20,52 as more knowledge may increase anxiety.53,54 Half of families that received an Australian booklet on comfort care early, with limited explanation, agreed that some sections increased anxiety. 8 Others found that practitioners were concerned about confronting patients with end-of-life issues early. 39
A limitation of our study was that sampling procedures were not necessarily representative of the two countries. Further, acceptability by practitioners is an important prerequisite, but only a first step to support families in practice. The booklet clearly needs further evaluation by families, revision in response to specific comments, and testing of effects, because despite successful involvement in decision making, actual patient outcomes may be unchanged. 55 Possible effects on families include lessening bereavement, 56 better preparation of death, which may relate to less anxiety, depression, and complicated grief, 57 and higher satisfaction with care. 58 Families' better understanding of prognosis may relate to fewer burdensome interventions, 59 and a perception of dementia as a terminal disease may even result in more comfort. 37
In conclusion, the concept of written information on comfort care was welcomed by practitioners of European countries widely differing in attitudes toward end-of-life care and decision making. Booklets may support practitioners, and nurses in particular, in providing comfort care for dementia patients and their families.
Footnotes
Acknowledgments
We thank Jurriaan P. Oudhoff, Ph.D., for his suggestions to an earlier version of the manuscript.
This work was supported by the Lino Maestroni Foundation-Palliative Medicine Research Institute, Italy (data collection in Italy); the national insurance companies Agis and Fonds Nuts Ohra, and by Fonds Sluyterman van Loo (national agency that supports projects focused on well-being of the elderly) (data collection in the Netherlands); the Netherlands Organisation for Scientific Research (NWO, the Hague; Innovational Research Incentives Scheme, a career award to JTS [grant number Veni 916.66.073]; and the Department of Nursing Home Medicine, and the Department of Public and Occupational Health of the EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam.
Preliminary results were presented at the Annual meeting of the Gerontological Society of America, New Orleans, November 20, 2010.
Author Disclosure Statement
No competing financial interests exist.