
Abstract
Abstract
Background:
U.S. children with life-limiting illness face barriers to accessing palliative care. In 2006, Massachusetts signed into law a statute providing for the creation and funding of the Pediatric Palliative Care Network (PPCN). This innovative, exclusively state-funded program provides comprehensive direct and consultative community-based pediatric palliative care services including: (1) pain and symptom management, (2) case management and assessment, (3) social services, counseling, and bereavement services, (4) volunteer support services, (5) respite services, and (6) complementary therapies. Provision of care is through a network of state-licensed hospice programs, and an array of professional and volunteer services.
Objective:
To describe Massachusetts' experience in implementing a novel pediatric palliative care program.
Design:
Enrollment and service trends were identified using Massachusetts Department of Public Health administrative data. Responses to a written family satisfaction survey provided to each family enrolled on PPCN are summarized.
Results:
In fiscal year 2010, PPCN partnered with 11 hospice programs to provide services to 227 children with life-limiting illness. A total of $680,850 (86.7%) of state funding went to direct contract funds for hospices. Admitting diagnoses included cancer (30%), chromosomal abnormalities (17%), neurodegenerative disorders (15%), and other (38%). There were 11 deaths, 100% of which occurred in the family's requested location. Median length of stay on service prior to death was 233 days. Families most commonly implemented psychosocial and case management services, followed by complementary therapies, and volunteer services.
Conclusions:
Successful implementation of a statewide pediatric palliative care program as modeled in Massachusetts is highly feasible at relatively low cost.
Introduction
In 2006, as part of the state Health Care Reform Act, Massachusetts signed into law a statute providing for the creation and funding of the Pediatric Palliative Care Network (PPCN). 11 This unique, exclusively state-funded program is designed to overcome existing policy barriers and provide comprehensive direct and consultative palliative care services to children with life-limiting illnesses. This article aims to describe the Massachusetts experience in implementing this program with attention to both successes and challenges.
Formation of the PPCN
Driving forces behind the establishment of the PPCN included a state effort to address two central barriers identified by a grassroots community of parents of children with life-limiting illness: (1) requirement of physician certification that children have only 6 months left to live, and (2) loss of access to private duty nursing in the home setting.
These parental concerns reflect the U.S. reality that models for the funding and provision of pediatric palliative care are based upon adult policy. Pediatric and young adult patients under the age of 24 years account for a mere 0.4% of hospice patients in the United States. 12 Yet, rules governing eligibility, payment, and conditions of participation in the hospice benefit under both Medicaid and private insurance providers for children mirror the adult Medicare hospice benefit. 13 These rules include a requirement that a patient be documented as having only six months to live—a provision that excludes a vast proportion of children with life-limiting conditions. Such children include infants with congenital anomalies typically fatal within the first 2 to 3 years of life, children with chronic diseases such as cystic fibrosis whose disease trajectory is often unclear, and children with diagnoses such as cancer for whom, in a majority of cases, cure remains a realistic hope. Until the mandate for concurrent care for children receiving hospice benefits under the 2010 federal Patient Protection and Affordable Care Act, eligibility criteria further required that for children to receive palliation under hospice, they must relinquish all disease-directed therapy. 14 Implementation of the new mandate will vary from state to state, and continues to require eligible children to have a prognosis of six months or less. Thus, it remains to be seen to what extent the new provision will increase access to hospice for children.
In light of these limitations, individual states have experimented with models for the provision of comprehensive pediatric palliative care services. Beginning in 1995, $3.2 million in federal funding was earmarked for state demonstration programs—so called “waiver” programs—in pediatric palliative care. Three states—including Florida, California, and Colorado—received monies under the 1995 demonstration grant to create joint state and federally funded palliative care programs. To date, no published data are available on the Colorado or California programs. 15 Florida has published its experience with the demonstration program developed in 2005 and titled Partners in Care: Together for Kids (PIC:TFK). 16
In April 2006, the state of Massachusetts signed into law “An Act Providing Access to Affordable, Quality, and Accountable Care.” The Pediatric Palliative Care Program was established in Section 24K of Chapter 111 of the General Laws. 11 The statute provided for the creation and funding of a pediatric palliative care network administered by the Massachusetts Department of Public Health (DPH). Unlike prior Medicaid waiver initiatives, the program is entirely state funded. It is thus wholly independent from Medicaid, and beholden to no Medicare-derived eligibility or service provision regulations. Similar to Medicaid, PPCN is subject to government budgetary appropriations cuts. It does not, however, have the protected status of Medicaid programs and thus could in theory suffer complete dissolution in a fiscal downturn. Enrollment criteria for PPCN are intentionally more inclusive than the pediatric hospice benefit. As such, PPCN provides an alternative to the hospice benefit.
Program Design
The mission of PPCN is to serve the unmet physical, emotional, social, and spiritual needs of children in Massachusetts with life-limiting illnesses. The program is structured with oversight centered in DPH with provision of care by community hospices. PPCN is thus an enhancement and coordination of pre-existing services within the state. As such, it provides a model of care replicable in other states.
PPCN is a community-based program that provides services to families in their homes. It thus complements, but does not replace, existing hospital-based palliative care services. It is administered through the Massachusetts DPH Title V Children and Youth with Special Health Care Needs Program. PPCN receives an annual budget as voted and approved by the state legislature. PPCN contracts with a network of 11 state-licensed hospice programs throughout Massachusetts (Fig. 1). Each hospice receives a contract funded for a fiscal year, but develops its own budget reflective of services. State budgeting for individual hospices evolved over the lifetime of the PPCN. For the first two years of PPCN's existence all hospices were flat funded at $55,000 per year. Hospices with a higher census were then provided with contract amendments to meet higher costs at the conclusion of the third quarter. By 2009 the decision was made to link hospice contracts to census. Subsequent contract amounts were based on the prior year's enrollment numbers.
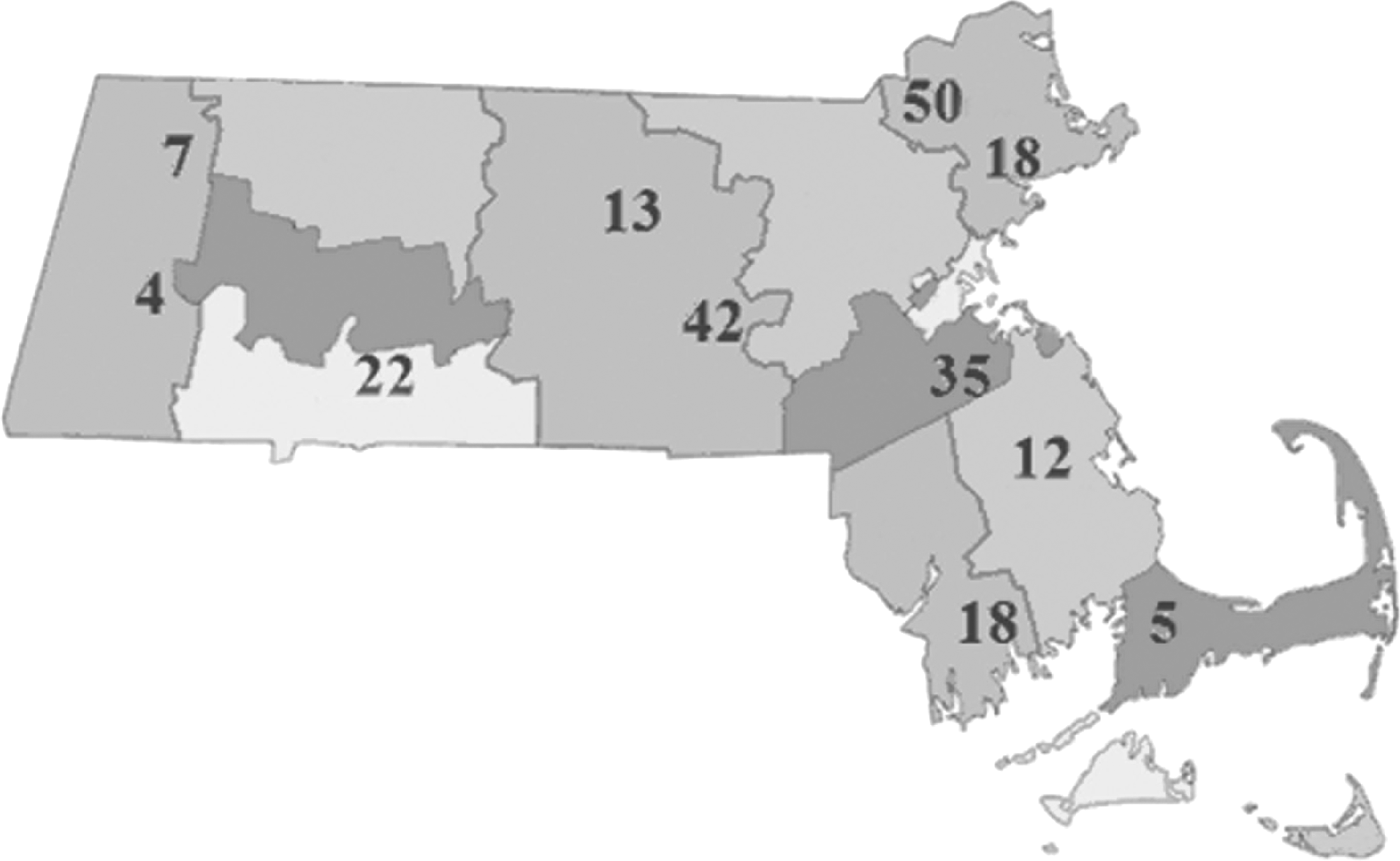
Distribution of hospices throughout the Commonwealth of Massachusetts. The geographic location of each hospice is depicted on the map by the number of children served in 2010. Notably, hospices are not distributed evenly throughout the state, with clusters in some counties.
Eligibility criteria
Eligibility criteria for enrollment on PPCN are intentionally broad. Enrollment on PPCN provides an alternative to enrollment on the more restrictive hospice benefit. To enroll on PPCN children must be residents of the state of Massachusetts, ages newborn until 19 years, and diagnosed as having a life-limiting illness as determined by a physician with no requirement regarding life expectancy imposed. Children enrolled on PPCN may continue to receive cure-directed care.
Children may be referred from any source, including family self-referral. All children referred to PPCN who meet the above three criteria are enrolled. Services are available to all eligible families regardless of ability to pay. PPCN is a payer of last resort such that services will first be reimbursed through private or government insurance with a palliative care benefit. Families lacking insurance coverage do not contribute out-of-pocket for program services.
Services provided
Service provision begins with a multidisciplinary assessment of a child and family by hospice staff within 48 hours of referral. A resultant formalized care plan is provided in writing to the family and primary care provider. Parents may choose to receive any of the PPCN services available through their hospice. For non-English speaking families interpretive services vary by hospice depending on resources. They range from interpreter phone services, to volunteer interpreters from within the local community. PPCN services are summarized in Table 1. PPCN services do not include provision of medications, durable medical equipment, personal care assistants, home health aides, or financial assistance. A child may continue to receive these services through her health insurance.
PPCN, Pediatric Palliative Care Network.
Methods
Enrollment and service trends were identified using Massachusetts DPH administrative data. All PPCN hospices maintain medical records documenting care and decision-making for each enrolled child. Hospices submit electronic reports on a monthly basis to the DPH PPCN director. These reports are tied to invoice billing and include: cost of services for previous 30 days, census, referrals, deaths, discharges, and volunteer hours.
A written family satisfaction survey is provided to all families with the goal of facilitating programmatic improvements. This survey was designed by the PPCN director and is administered in person by a hospice staff member or volunteer after 3 months on service or following a child's death—whichever comes first. Surveys are currently available in English. Surveys are returned to the hospice, deidentified, and submitted to the PPCN director. Parents are asked to answer a total of sixteen questions spanning three domains. In two domains, survey questions assess the impact of PPCN services on a child's comfort, access to services, and parental comfort with caring for the child. In the final domain, questions assess the impact of PPCN on reducing the need for other medical services.
Results
Enrollment data
In fiscal year 2010, PPCN provided services to 227 children with life-limiting illness. This represented an 11% increase in census from the prior year. These children came from 224 individual families. The program also provided support services to 95 healthy siblings. Demographic characteristics of children and families are summarized in Table 2.
The Department of Children and Families (DCF) is the Massachusetts state agency charged with the responsibility of protecting children from child abuse and neglect.
Approximately 10% of families spoke a primary language other than English—including Spanish, Portuguese, Japanese, Mandarin, Polish, Arabic, and Hindi. Race and ethnicity data were not collected.
As documented in DPH administrative records, in 2010 there were 11 deaths on service (4.8% of annual census) following a median length of stay on service of 233 days (Table 2). An additional 6 children were discharged to hospice and 4 of these children later died. One hundred percent of deaths occurred in the location requested by the family.
Children ranged in age from newborn through 18 years. The three most common diagnoses included approximately 30% malignancy, 17% chromosomal abnormality, and 15% neurodegenerative. Recent efforts to offer support to parents with a prenatal terminal diagnosis have resulted in the enrollment of three families. The largest referral source was the DPH Care Coordination Program which accounted for a full 37% of all referrals (Fig. 2). Families referred through DPH are typically receiving additional state services. Consequently, the social demographics of families served by PPCN reflect a truly underserved population (Table 2).

Breakdown of referral sources for all children enrolled on Pediatric Palliative Care Network (PPCN) in 2010.
Nonclinical service utilization
Nonclinical volunteer services constitute an essential element of palliative care. In 2010, volunteers provided a total of 2296 hours of care to families on PPCN. Nine of 11 hospices offered at least three complementary therapies. Percentage of hospices offering complementary therapies were as follows: massage therapy (82%), music therapy (73%), art therapy (64%), reiki (55%), and pet therapy (36%). Nearly all families whose child died participated in bereavement programs targeted at siblings. Of the numerous services available, families most commonly implemented psychosocial and case management services, complementary therapies, and volunteer services.
Cost
Since its inception in 2006, state funding for PPCN varied from $785,000 to $800,000 per fiscal year. Funding in fiscal year 2010 was $785,000 of which $680,850 (86.7%) constituted direct contract funds to hospices. An additional $42,000 (5.4%) went to community outreach and program marketing. This demonstrates a very low state administrative overhead. A breakdown of hospice use of these funds is presented in Table 3 and reveals a significant administrative overhead at the level of the hospices.
Includes: hospice program coordination, payroll taxes, fringe benefits, staff travel, clerical staff, facility maintenance.
DPH, Massachusetts Department of Public Health.
In 2010, individual hospice enrollment varied from 4 children to 50 children. Individual hospice contracts in 2010 reflect this range and varied from $14,300 to $127,000. This translates into a significant variation in the cost per child depending on the hospice—with a range of $1,520 to $7,421. Cost variability is in part reflective of hospice census and the subsequent diminution of overhead costs when census is increased.
Family satisfaction
As described in the methods section, DPH requires that all families enrolled on PPCN be offered a family satisfaction survey. In 2010, 36 of 227 families (16%) completed the survey. This limited response rate makes interpretation of results extremely difficult given the likelihood of responder bias. Family responses are summarized in Table 4. Of the sample who responded, a majority felt that their child received “excellent” care from PPCN and that PPCN improved their child's quality of life and access to resources.
PPCN, Pediatric Palliative Care Network; NA, not applicable.
Provider assessments
PPCN additionally relies on annual feedback from its hospice providers to identify successes and programmatic challenges. Feedback is collected as an open-ended survey. Many hospices identified maintenance of adequate census, and the need to “educate families and referral sources that palliative care IS NOT hospice care” as challenges. Additional challenges included meeting the needs of families struggling to pay bills and provide for the basic care of their children (including housing and food), as well as communication barriers with non-English speaking families.
When asked to identify goals for the coming year, many hospices focused on service expansion. One hospice is developing a community education program to aid in efforts to reach more children. Another hospice described multiple initiatives: development of a monthly newsletter for families, and pursuit of grant funding for “quality of life programs” including recreational family outings and funds to support such basic needs as utilities and rent.
Discussion
Massachusetts has implemented an exclusively state-funded, community-based pediatric palliative care program. The program's aim was to ameliorate overly restrictive eligibility criteria as a barrier to access. The fact that fewer than 5% of children on service died in the past year speaks to the reality that PPCN is truly meeting the goal of the American Academy of Pediatrics in providing compassionate palliative care “throughout the course of illness, whether the outcome ends in cure or death.” 7 As such, the program has proved successful. Furthermore, that 100% of those children who died did so in their families' location of choice is evidence that this compassionate care is benefiting families.
These successes notwithstanding, PPCN has faced several challenges over its first four years of existence. Enrollment trends proved both surprising and challenging. At its inception in 2006, approximately 400 children were estimated to be dying annually in the state of Massachusetts of nontraumatic causes—this was PPCN's target population. 17 Initial expectations were that loosened eligibility criteria would allow the state to capture a greater proportion of children with a steadily declining disease trajectory, and anticipated death over 6 to 12 months. As evidenced by the extremely low rates of death on service, it has become clear that a different population of children with life-limiting illnesses is being captured—and it seems to be a far larger one. This population is one whose disease trajectory is more chronic. No good data exist on the number of Massachusetts children experiencing “life-limiting illness” with chronic trajectories. Furthermore, data on the number of children enrolled on the hospice benefit are not available. This poses a significant barrier to program evaluation, making it impossible to measure the success of PPCN in capturing this population. A greater epidemiologic understanding of this eligible population is essential for programmatic evolution, as is the need for more comprehensive data collection on the population currently served by PPCN—including information on race, ethnicity, and insurance status.
Identification of appropriate children for enrollment, and variability in strategies for outreach by individual hospices proved particularly challenging as evidenced by significant variation in enrollment hospice to hospice. This variation is partly responsible for a seven-fold difference in cost per child between the highest and lowest census hospices by the end of 2010. Efforts to standardize costs across providers are ongoing, and DPH is currently projecting a move to a unit rate reimbursement by fiscal year 2013. This effort would ideally result in a more consistent cost per child, and encourage individual hospices to modify their outreach practices.
From a global programmatic perspective, overall enrollment on PPCN has steadily increased each year. State funding, however, has remained static. The exclusively state-funded nature of the program, and its availability to all families regardless of insurance status or ability to pay, are both strengths and weaknesses in terms of program model. As a relatively wealthy state, Massachusetts has demonstrated both an ability and willingness to expand the provision of palliative care to more children in line with American Academy of Pediatrics and National Institutes of Health goals. Less wealthy states might be challenged to implement similar programs. Future efforts to collect data on comparative cost expenditures between children enrolled on PPCN, those with similar illnesses receiving the hospice benefit, and those with similar illnesses not enrolled in either program will be essential to demonstrate the fiscal viability of this model for other states.
Finally, the program has had limited success in collecting comprehensive family satisfaction data. Response rates of less than 20% from participating families provide inadequate data on which to assess the success of the program in meeting the needs of its patients. Future efforts to increase response rates, and gather more quantitative measures of quality—including pain and symptom management, spiritual/emotional support, and preferred location of death—are necessary for systematic evaluation of PPCN.
Conclusions
Policies defining broader palliative care eligibility criteria for reimbursement under health insurance programs are essential to achieving improved care. The current federal health care reform bill goes as far as allowing children to receive concurrent palliative care and care with curative intent, but does nothing to ameliorate the overly restrictive requirement that children have only six months to live. 14 Massachusetts has created what appears to be a sustainable model to comprehensively meet the needs of its children with life-limiting illness. Whether models incorporating the inclusive eligibility requirements and breadth of services available under PPCN can be replicated in other states remains to be seen.
Footnotes
Acknowledgments
The authors express their gratitude to the providers, families, and children on PPCN.
Author Disclosure Statement
No competing financial interests exist.