
Abstract
Abstract
Background:
Since 1999, there has been a significant increase in hospice providers and hospice use in nursing homes. A 1997 Office of Inspector General (OIG) report warned of possible kickbacks, monetary and otherwise, that might be paid by hospices to nursing homes in exchange for referrals. One possible kickback mentioned in the report was nursing homes receiving additional staff hours at no cost, which could lead to decreases in nursing home staffing. The purpose of this study was to determine if changes in nursing home hospice volume were related to changes in certified nursing assistant (CNA) staffing.
Methods:
The study included free-standing nursing homes with at least 3 years of observation between 1999 and 2006, no fewer than five deaths in any year, and between 30 and 500 beds (n=10,759). We examined the longitudinal relationship between changing hospice volume and CNA minutes per resident day (MPRD), utilizing nursing home fixed-effects regression analysis and adjusting for resident case mix and changing organizational characteristics.
Results:
The introduction of hospice services in a nursing home did not result in statistically significant changes in CNA staffing. Instead, increases in hospice volume resulted in small increases in CNA staffing. Specifically, the addition of 1000 hospice days, in a given year, resulted in an additional 0.79 (95% confidence interval [CI] 0.373–1.211) CNA MPRD.
Conclusions:
The proposition that nursing homes may be decreasing their staffing as a result of receiving additional hospice staff was not supported by this study and, in fact, nursing homes were found to only slightly increase CNA staffing with increasing hospice volume.
Introduction
Two earlier reports by the OIG that examined nursing home hospice provision during the 1990s detailed the potential conflicts that could enter into contractual arrangements between nursing homes and hospice providers.8,9 A main concern was the potential for decisions about hospice provision to be influenced more by financial considerations than by clinical considerations. 8 The OIG was particularly concerned with the possibility of kickbacks provided by hospice providers to nursing homes in exchange for referrals. One kickback mentioned in the OIG reports was the nursing home “receiving additional staff hours at no additional cost” (p. 6). 8 The suggestion here is that hospice staff could provide some of the hands-on care previously provided by nursing home staff, thereby allowing the nursing home to reduce staffing. However, no research has yet addressed this important issue.
When a nursing home resident receives hospice services, the hospice is expected to provide services, such as nursing care specific to the terminal illness, medical social services, counseling, occupational and/or physical therapy, and any other services necessary for the management of the terminal illness. The nursing home is expected to continue providing room and board and any hands-on care not related to the terminal illness. 10 OIG reports suggest that hospice staff could provide some of this hands-on care allowing the nursing home to reduce staffing as a means of incentivizing referrals to hospice.8,9
The purpose of this study was to determine if changes in nursing home hospice volume were related to changes in certified nursing assistant (CNA) staffing. We have focused on CNA staffing because these nursing home employees provide the vast majority of hands-on care in nursing homes. 11 This care would be most amenable to substitution by hospice employees or, specifically, hospice aides. We also sought to determine if increased competition among hospice providers in the nursing home's county led to decreased CNA staffing.
Methods
This cohort of nursing homes was defined utilizing the Online Survey Certification and Reporting (OSCAR) database and the Residential History File (RHF). The OSCAR data are available from the Centers for Medicare and Medicaid Services (CMS) and are based on data collected from each Medicare/Medicaid certified nursing home during annual survey inspections. The RHF is a unique data resource built using Medicare enrollment data, Medicare claims data, and Residential Assessment Instrument Minimum Data Set (MDS) data. 12 The RHF can be used to track individuals as they move through the long-term care system, including between different care settings and different care types (e.g., hospice). These data were obtained through a data use agreement (DUA) with CMS.
Over the 7-year study period, 131,458 nursing home observation years were identified. Nursing home observation years were excluded if the nursing home was hospital-based (n=15,464), had fewer than 30 beds or more than 500 beds (n=3337), had fewer than 3 years of observation (n=11,607), had fewer than five deaths in any year (n=17,167), or was missing data on covariates (n=11,776). This resulted in 72,107 nursing home observation years among 10,759 nursing homes.
The dependent variable was defined as the number of CNA minutes per resident per day (MPRD), a measure of nursing home direct-care staffing. Facilities report the number of CNA hours during the 2 weeks prior to their annual survey. CMS converts the number of hours into full-time equivalents (FTEs; based on a 35-hour work week) and this is reported in the annual OSCAR data. Nursing home staffing data derived from OSCAR have been used in numerous previous studies. 13
For this study, we converted the FTEs back into hours, by multiplying by 35, and divided the total number of CNA hours by the number of residents in the facility (also drawn from the OSCAR) to arrive at the CNA hours per resident day (HPRD). For ease of interpretation, we further transformed HPRD into MPRD by multiplying by 60. We also cleaned this variable when the FTEs reported were implausible (when total FTEs were 995 or higher or if there were more than three times the number of CNAs reported than the number of beds in a facility). If data were missing in a particular year, we imputed the values by randomly choosing a value from the quartile of nursing homes having the most similar values (to the “missing value” nursing home) in the subsequent year. Less than one-half of 1% of facilities had missing values each year (and in most years it was between 0.1% and 0.2%).
We operationalized the introduction of hospice services as a nursing home transitioning from having less than 1% of its total resident days in a calendar year covered by hospice to more than 1%. The RHF was used to identify the number of nursing home days for all residents in each facility in the calendar year as well as the number of those days that were hospice days. The proportion of days that were hospice was calculated using these two counts. A dichotomous variable was then created to indicate when a nursing home reached the 1% threshold that signified “adding hospice.” Hospice volume was operationalized by totaling the number of resident hospice days in the nursing home in a calendar year. For ease of interpretation, this variable was standardized to 1000 nursing home hospice days.
We controlled for numerous nursing home attributes including the total number of resident days per calendar year, and for other time varying nursing home characteristics including a yearly indicator of whether more than two thirds of a nursing home's hospice residents were cared for by for-profit hospices, the proportion of residents on Medicaid, the proportion of residents on Medicare, occupancy rate, resident case mix, nurse staffing, existence of a special care unit, and existence of a physician extender (nurse practitioner or physician's assistant). To control for secular trends, we also included indicator variables for each year. We included two measures of resident case mix, one based on all MDS admission assessments (i.e., the case mix for all newly admitted residents in a year) and one based on all MDS annual assessments (i.e., the case mix for long-stay residents). We used the resource utilization group (RUG III) system, which classifies residents into categories based on their estimated resource utilization. This approximates the relative staff time associated with caring for the average resident in each group. Thus, the higher the case mix score, the more severe the average acuity profile of the residents in a nursing home. These measures were standardized, so that the regression results reflect the influence of a one standard deviation change in case mix.
To examine the influence of hospice competition, we included a variable indicating the number of hospices in the nursing home's county providing services in nursing homes each year. We identified hospice providers who provided services to nursing home residents each year as identified on Medicare claims in the RHF. We then grouped residents by their nursing home's county and added up the unique number of hospices that were providing care to those residents.
We performed panel multivariate regression analysis using a facility fixed-effects model. A panel fixed-effects model controls for unobserved time-invariant nursing home characteristics that may be correlated with CNA MPRD, and allows for a difference-in-difference model causal interpretation of our results. We used the XTREG (cross-sectional time-series linear regression) procedure available in Stata statistical software version 10, which fits regression models to panel data. 14
Results
Table 1 presents the descriptive statistics for nursing homes included in the fixed-effects analysis. Additionally, this table identifies the dataset from which the variable was derived. As shown in Fig. 1, about 45% of nursing homes had at least 1% of their resident days covered by hospice at the beginning of the study period. This proportion increased only slightly in 2000 and began to increase dramatically after that point, with about 80% of nursing homes reaching the threshold by 2006.
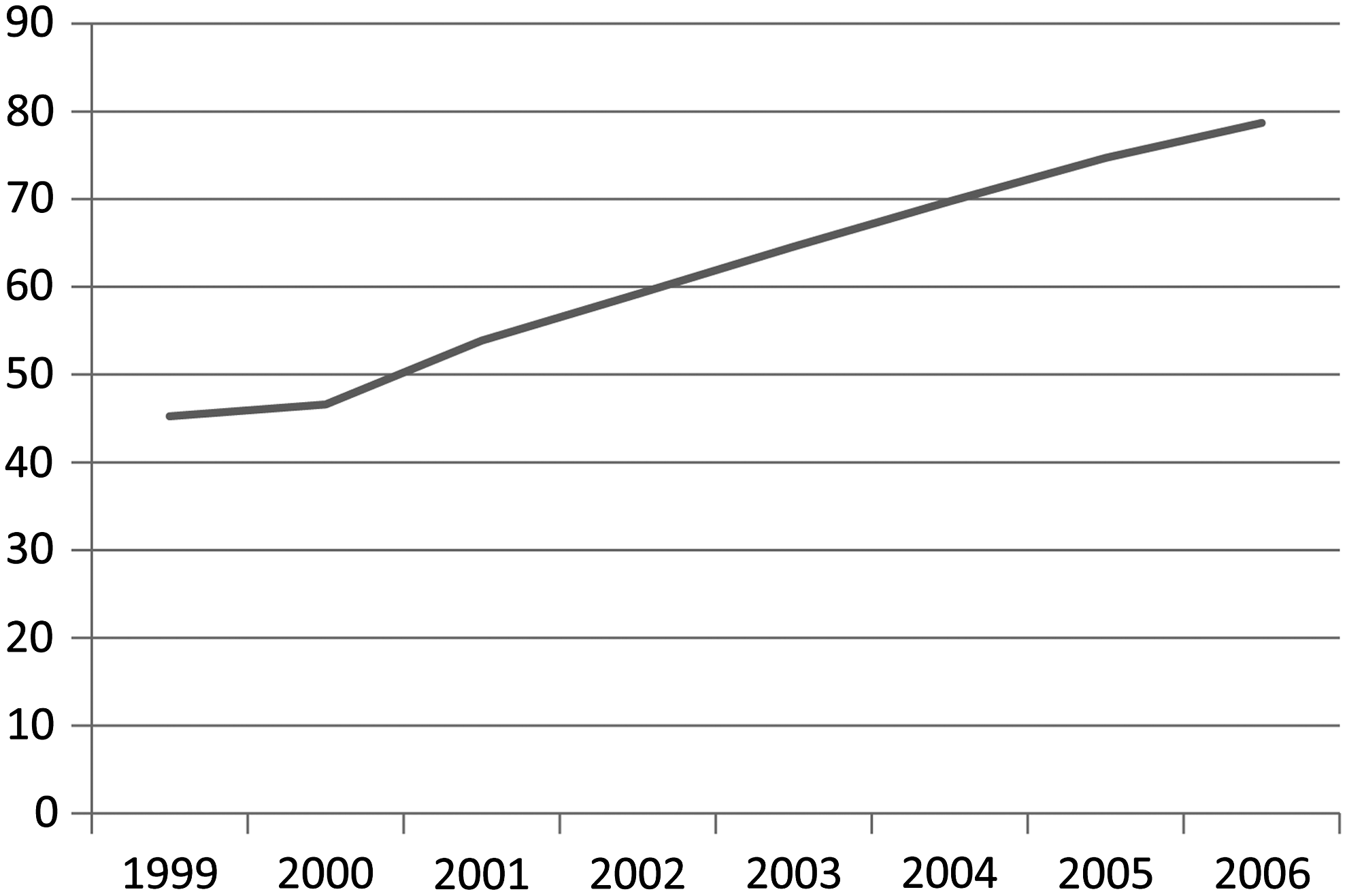
Proportion of Nursing Homes with at least 1% of Resident Days Covered by Hospice.
OSCAR, Online Survey Certification and Reporting; RHF, Residential History File; CNA, certified nursing assistant; MPRD, minutes per resident day; LPN, licensed practical nurse; RN, registered nurse.
Table 2 shows the results of the fixed-effects regression analysis. Our main independent variable of interest, adding hospice, was shown to not significantly affect CNA MPRD (95% confidence interval [CI]: −1.19–0.01). However, increasing hospice volume in nursing homes was related to statistically significant increases in CNA MPRD. Specifically, for every 1000 hospice days added in the nursing home during a calendar year, CNA MPRD increased by more than three-quarters of a minute (95% CI: 0.37–1.21).
LPN, licensed practical nurse; RN, registered nurse.
Hospice competition in the county, as measured by the number of hospice providers in the county providing services in nursing homes, was found to significantly decrease CNA MPRD. Specifically, the addition of one hospice provider in the county was related to a 0.29 minute decrease in CNA MPRD (95% CI: −0.4 to −0.19).
Discussion
Study findings show there is no decrease in nursing home CNA staffing when a nursing home introduces hospice or uses a higher volume of hospice care. Therefore, these findings do not support the OIG's concern of staff substitution with nursing home hospice use. Instead, findings show that adding hospice services (i.e., transitioning from less than 1% of resident days in a calendar year covered by hospice to more than 1%) does not significantly affect CNA staffing, as measured by CNA MPRD. Further, findings show that every additional 1000 hospice days nursing home residents use annually result in a three-quarters of a minute increase in CNA MPRD. For a nursing home with 120 residents, this increase translates to an additional hour and a half of CNA staffing time each day.
These findings are consistent with what would be expected in terms of direct-care staffing as a nursing home increases its hospice use. By definition, residents receiving hospice services are at the end-of-life and likely suffering from multiple comorbid conditions. These residents are sicker and in need of more care than nursing home residents not at the end of life, so a nursing home caring for more of these residents will need additional direct-care staff. That is as long as the hospice provider is not supplying the nursing home with substitute staff, and our findings support this contention.
Our findings regarding the impact of hospice provider competition on CNA staffing are less straightforward. We found that with each additional hospice provider in the county, CNA MPRD decreased by just over a quarter of a minute. For example, again considering a nursing home with 120 residents, this would translate into a reduction of just over 15 minutes of CNA staffing each day. However, this would apply to all nursing homes in the county, not just those providing hospice services. Our measure of hospice competition, the number of hospices in the county providing services in nursing homes, is somewhat crude and does not take into account differences in county populations or the number of nursing homes in counties. Additional research that more precisely measures hospice competition is needed.
Consistent with any observational study, our study is limited by data constraints. Specifically, our observations began in 1999 and hospice provision in nursing homes began growing well before 1999; therefore, many of the nursing homes in our study had added hospice prior to our study period. These early adopters may have been different from later hospice adopters in important ways and hospice relationships with nursing homes may have been different during the early years of hospice provision in the nursing home setting. In addition, our results may have been affected by the nature of the nursing home staffing data. Staffing is self-reported by nursing homes as part of the annual inspection process and could, therefore, be biased. However, there is no reason to believe that this reporting bias would change over time. Therefore, the study's longitudinal design, and examination of change, serves to lessen concerns about reporting bias.
In conclusion, the proposition that nursing homes may be decreasing their staffing as a result of receiving additional hospice staff was not supported by this study and, in fact, nursing homes were found to slightly increase CNA staffing with increasing hospice volume. Therefore, the OIG concern that hospice staff substitution may incentivize hospice referrals in nursing homes was not supported by this research.
Footnotes
Acknowledgments
This research made possible in part by the Shaping Long Term Care in America Project funded by the National Institute on Aging (1P01AG027296). Drs. Leland and Lepore were funded through the Agency for Healthcare Research and Quality (AHRQ) National Research Services Awards (NRSA) postdoctoral fellowship training grant (5T32HS000011-24) during this study.
Author Disclosure Statement
No competing financial interests exist.