
Abstract
Abstract
The medicinal and recreational use of cannabis has been controversial, especially in the United States. Marijuana for medicinal use is approved in 14 U.S. states and has recently been considered for legalization in several additional states. Given its demonstrated efficacy in symptom management, marijuana has a potential role in palliative care. This study utilized a 16-item questionnaire to assess the knowledge, experience, and views of hospice professionals regarding the use of marijuana in terminally ill patients. The study results revealed that, like the general public, hospice health care providers are generally in favor of legalization of marijuana and, if legalized, would support its use in symptom management for their terminally ill patients.
Introduction
Throughout history, the medicinal and recreational use of cannabis has been controversial, especially in the United States. Marijuana for medicinal use is approved in 14 U.S. states and has recently been considered for legalization in several additional states. Per federal regulation, however, marijuana is still a schedule I controlled drug substance. Recently, the American Medical Association, along with the Institute of Medicine and the American College of Physicians, has asked that the Drug Enforcement Administration consider downgrading marijuana from schedule I to schedule II to facilitate the development of evidence-based practices.5,6
Public support for medicinal marijuana use is also strong, with 70% to 80% of Americans supporting a policy for physicians to be able to prescribe marijuana.7,8 Recently, an ABC News/Washington Post poll reported that 81% of respondents support the idea of legalizing marijuana for medical use, compared with 69% of those similarly surveyed in 1997. 9
No studies have been done to date evaluating hospice health care professionals' knowledge, views, and experience with marijuana for symptom management. This study assessed the knowledge, experience, and views of hospice professionals regarding the use of marijuana in terminally ill patients.
Methods
Instrument
A 16-item questionnaire was prepared. Two open-ended questions solicited participant's knowledge of potential medical uses and adverse effects of marijuana. A series of multiple choice questions queried participants' experience and views regarding the use of marijuana to palliate symptoms. Several of the questions were adapted with permission from a 2004 American Association of Retired Persons (AARP) survey. Response options included “ agree,” “somewhat agree,” “somewhat disagree,” “strongly disagree,” and “no opinion/don't know.” The final questions collected demographic information, including hospice/palliative care experience, number of years in practice, discipline, age, gender, state of residence and knowledge of legal status of marijuana in that state.
Survey methodology
Approval for this survey was obtained through the institutional review board at the University of Maryland. A focus group of nine hospice professionals separate from the survey group provided feedback on the clarity and readability of the questionnaire. After minor changes, the survey was released via the online agent Survey Monkey. An invitational e-mail was sent to the “all clinical” listserv (n=400) of a hospice that provides care in 11 states in the United States. The survey was open for 10 days.
Data analyses
The most frequently mentioned symptoms and side effects were grouped into categories. Descriptive statistics including mean, median, or frequencies were computed. Age, gender, discipline, number of years in practice, number of years of experience, percent of time spent practicing palliative medicine, and state legal status of marijuana were evaluated with respect to participants' responses using the χ2 and Fisher's exact test.
For statistical analysis, response options “strongly agree” and “somewhat agree” were grouped into “agree,” and “strongly disagree” and “somewhat disagree” were collapsed to “disagree. The discipline category of physicians was grouped with nurses, and social workers were grouped with self-declared “others.” Age groups were categorized as 50 years and higher, or 49 years and lower. Years of practice and experience were grouped by <5 or ≥5 years. The amount of time spent practicing palliative medicine was grouped into <50% and ≥50% of time. The represented states in which marijuana was considered legal were Michigan and California.
Data were analyzed with MyStat (Systat Software Inc., Chicago, IL). The level of statistical significance was set at 0.05.
Results
Respondent characteristics
The response rate for initiating the questionnaire was 52% (209 of 400) and for completing the questionnaire was 48.5% (194 of 400). All responses were included. For respondent characteristics, please refer to Table 1.
Knowledge on marijuana
Respondents were familiar with the potential medical uses and side effects of marijuana (Table 2). Pain and mood were the most frequently mentioned uses for marijuana (87% and 55%, respectively), but mood was also mentioned as a side effect (16%).
Pain also includes headache and discomfort.
Mood also includes depression, anxiety, agitation, restlessness, stress, euphoria.
Sedation also includes fatigue, lethargy, sleepiness, somnolence.
Includes cough, breathing problems, lung irritation, pulmonary, cold symptoms, lung cancer, sore throat, choking, dry mouth.
Includes brain damage, memory, cognitive changes, impaired judgment disorientation, confusion, loss of consciousness.
Includes restlessness, anxiety, paranoia, hallucinations, psychological changes.
Includes giggles, bliss, peace, euphoria, laughter, well-being.
Views on marijuana
Approximately 90% of hospice care professionals were in agreement on legalization of marijuana (Fig. 1).
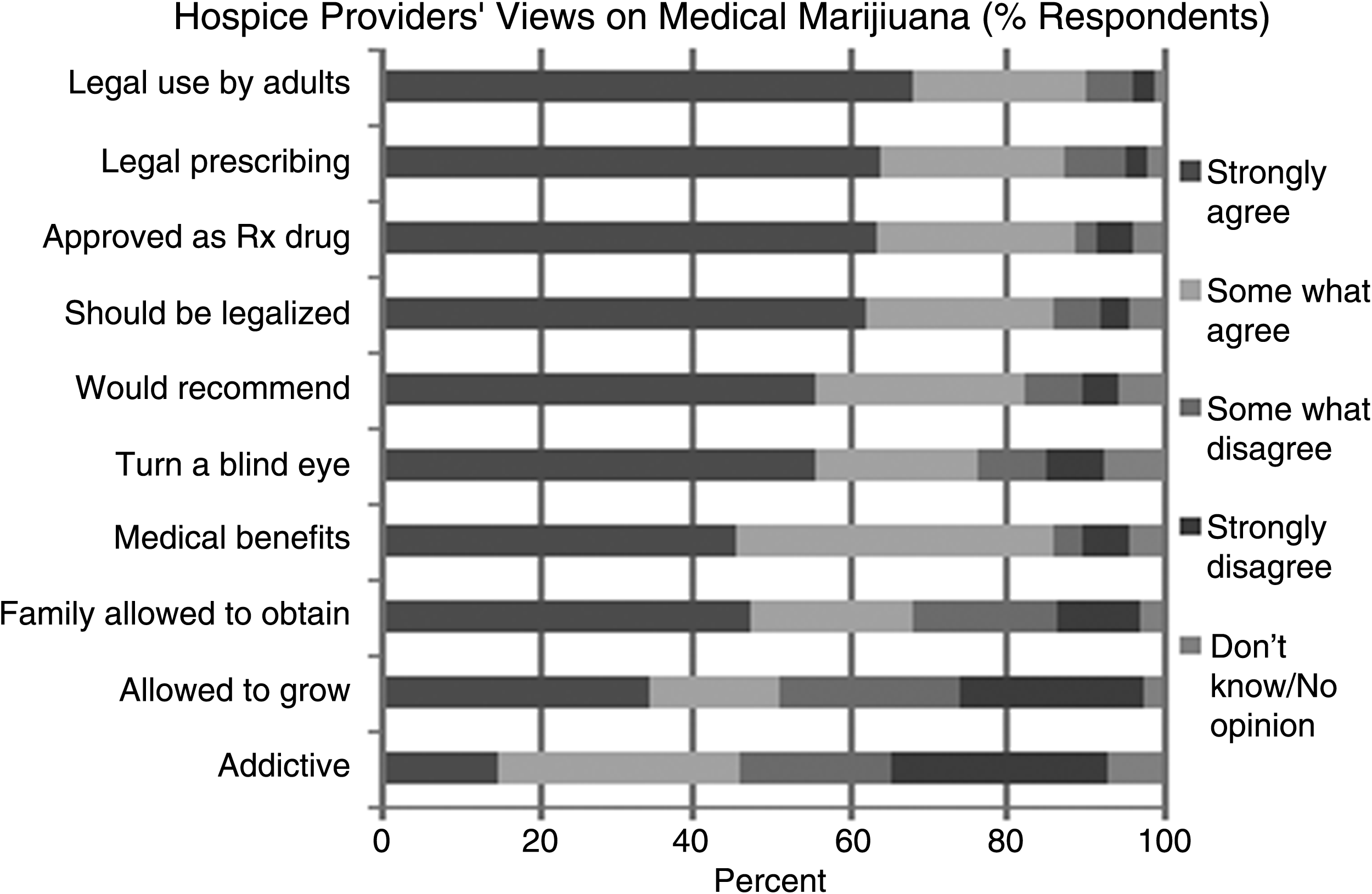
Hospice providers' views on medical marijuana (% respondents).
Hospice providers frequently see marijuana being used in clinical practice, or receive questions from patients and families about its use (47.8%). Concerning ethical implications, more than 75% of hospice providers would “turn a blind eye” if they found that their patient was achieving symptom control with smoked marijuana (Fig. 1). The majority of respondents (86.1%) agreed that marijuana has medical benefits. Nonphysician respondents were strongly in agreement with this statement (49.6% of nurses, 45.2% of social workers), whereas physicians were more likely to “somewhat agree” with this statement (76.9%).
Regarding acquisition, respondents were more in favor of family members being allowed to obtain small amounts of marijuana for a loved one (70%) or procuring it from a pharmacy (88.7%) than of individuals growing their own supply (51.2%) (Fig. 1). Providers with fewer than 5 years of experience were more likely to agree that family should be allowed to obtain marijuana for a loved one than providers with more experience (78% versus 62%, p=0.023).
Respondents were equally divided on whether smoked marijuana is addictive (Fig. 1). Respondents over the age of 50 were significantly more likely than younger respondents to disagree that smoked marijuana is addictive (64% versus 47%, p=0.034).
Respondents were not unified on which division of government is responsible for the legalization of marijuana (Fig. 2). The legal status of marijuana was found to significantly influence respondents views when comparing states where marijuana is legal versus not legal (Table 3).

Percent breakdown of respondents' views on the government's responsibility for legalization of medical marijuana.
Discussion
This survey found that the majority of respondents (90%) felt that marijuana should be legalized for palliate symptoms, and that, when recommended by a prescriber, adults should be allowed to obtain marijuana. Almost half of hospice care providers have had experience with patients asking about or using marijuana to palliate symptoms. Marijuana is legal for medical use in California and Michigan, accounting for 15% of survey respondents. Given that almost 50% of respondents have treated patients who have either asked about or admitted to using marijuana, respondents in states where marijuana is not legal are most certainly coming into contact with these situations.
A recent telephone poll by ABC News/The Washington Post, which randomly sampled 1083 adults nationally, found that adults under 65 years of age were 83% in favor of medical approval, of which 75% said that if approved it should be limited to terminally ill patients. 9 Likewise, it would be interesting to know if hospice professionals feel this way for all patients or just the terminally ill.
Hospice healthcare providers were familiar with many of the uses and side effects of marijuana. Of note, more respondents listed pain control and mood elevation as uses, which are not indications for currently FDA-approved cannabinoids. Mood was also mentioned as a side effect by many respondents. This finding may be a reflection of the media attention paid to the role of marijuana in relieving pain and spasticity and the enhanced focus on its limitations due to psychiatric effects.
Respondents over the age of 50 were significantly more likely than younger respondents to disagree that smoked marijuana is addictive (64% versus 47%, p=0.034). Older respondents may have more experience in palliative care and are therefore less concerned with the risk of addiction compared with the younger, less experienced group.
In those states where marijuana is not legal, respondents were significantly more agreeable with the medical benefit, legalization, and acquisition of marijuana for palliative purposes. This may suggest that the legalization of marijuana is not as glamorous as the media suggests. Given the complexities of implementing the state laws, it is not surprising that those respondents living in states where marijuana is legal were also significantly more likely to have personal views on recreational marijuana that affect their professional views.
For all questions regarding legal matters, physicians were more likely to somewhat agree versus strongly agree. A survey conducted in 2001 on physicians' views toward prescribing marijuana revealed that only a third of physicians polled would prescribe marijuana if it were legal. 10 In the current survey of hospice providers, 69% of physician respondents “somewhat agreed” that physicians should be allowed to prescribe marijuana if legalized, and an additional 15% “strongly agreed.” Comparing these survey results, hospice physicians are seemingly more agreeable to prescribing marijuana, if it were legal, than general physicians. 10 This may be explained by differences in practice experience and the time interval between surveys.
There were several limitations in this study, including the ability to take the survey more than once from different internet protocol addresses and a limited age range between 24 and 68 years of age. Although conducted nationally, the sample size was limited and included employees of only one hospice program. Finally, in an effort to encourage completion of the questionnaire, we did not ask about personal use of marijuana, which may have missed a critical demographic.
This study is the first to evaluate the knowledge, experience, and views of hospice health care providers on marijuana for medical purposes. This survey revealed that, like the general public, hospice health care providers are generally in favor of legalization of marijuana and, if legalized, would support its use in symptom management for their terminally ill patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.