
Abstract
Abstract
Background:
People with intellectual disabilities (ID) experience many barriers in accessing quality health care for serious and terminal illness, including delayed diagnosis, as signs and symptoms of illness are misinterpreted There is growing evidence that palliative care services are underused by people with ID.
Methods:
A 3-year project aimed at exploring ways of increasing access to palliative care services by people with ID in South West London was conducted. A project group designed training sessions for both ID and palliative care staff involving four hospices and 228 care homes. Evaluators used interactive cycles involving discussions and interviews to map learning and identify constructive ways forward.
Results and conclusion:
In general, the study found that there was a lack of understanding of each other's role between palliative care professionals and ID staff, with each unsure of what the other service is providing and how it is run. Recommendations include securing a development worker for ID and end-of-life care; conducting training for ID care staff; establishing how ID services are organized within the local area; linking to national training programs; ensuring that senior management is proactively involved; and ensuring that the goals of any initiative are clear and measurable.
Introduction
They experience many barriers in accessing quality health care for serious and terminal illness, including delayed diagnosis, as signs and symptoms of illness are misinterpreted. 3 There are several significant issues in the care of this client group including communication difficulties and consent issues, 4 and crucially for the provision of end-of-life care there is often a lack of understanding and collaboration between palliative care services and ID services.5,6,7 There is growing evidence that palliative care services are underused by people who have a learning disability.8,9 Policy and legislative agendas now recognize that hard-to-reach groups such as people with ID should have access to equitable health care (including palliative care services) and have provided a framework to do so.10,11,12
The need is growing, with an aging population: by 2021, the number of people with ID in England over the age of 50 is expected to have increased by 53%. 13 There is a growing incidence within this group of life-limiting illness associated with old age, such as cancer5,14 and Alzheimer's disease.15,16
One of the key barriers to people with ID accessing palliative care is the lack of understanding and training of the staff working with them. In England, ID care staff are often young, lacking in training and experience; staffing levels are often low; and turnover can be high. In contrast, palliative care staff are highly qualified, are able to offer considerable expertise, and palliative care services have an infrastructure for providing training. 8
To improve end-of-life care for people with ID, it could be suggested that ID staff as well as unpaid carers need access to accessible palliative care training. One way this is happening in the UK is through the Gold Standards Framework, 17 a progam of palliative care training for generalist providers that is being rolled out to ID care homes. At a local level, the needs of ID staff to access palliative care training and support may be met through closer links between ID and palliative care services.
We report on a 3-year project aimed at exploring ways of increasing access to palliative care services by people with ID within one geographical area. A grant was awarded by the King's Fund within its “Partners for Health in London” program designed to enable partner organizations to learn, disseminate, and implement more effective ways of improving health and health care. The work was conducted in South West London (2006–2010). It was supported by the South West London Cancer Network and hosted by Trinity Hospice, drawing on well-established links and networks across South West London, involving four hospices and 228 care homes.
An important focus of the project was to assess the effectiveness and sustainability of three different approaches: (1) training of ID staff on basic end-of-life care; (2) training of palliative care staff on how best to meet the needs of people with ID; and (3) a link-worker scheme where professionals from both professional areas would have a designated point of contact for support and information. This paper aims to capture the learning from the project, focusing on how successful and constructive were each of these elements. It will be of particular interest to commissioners and providers of health and social care services for people with ID, and to both general and specialist palliative care services; those concerned with developing and implementing end-of-life care strategy locally and nationally; and key training providers working with care staff and professionals in both ID and palliative care services.
Methods
Project assumptions
A project steering group was established comprising experts from the fields of ID and palliative care, people with ID, and carer representatives. The desired pathway from terminal illness diagnosis through to death is reflected in Figure 1, highlighting the presumed importance of both training and a collaborative approach toward achieving our desired end goal.
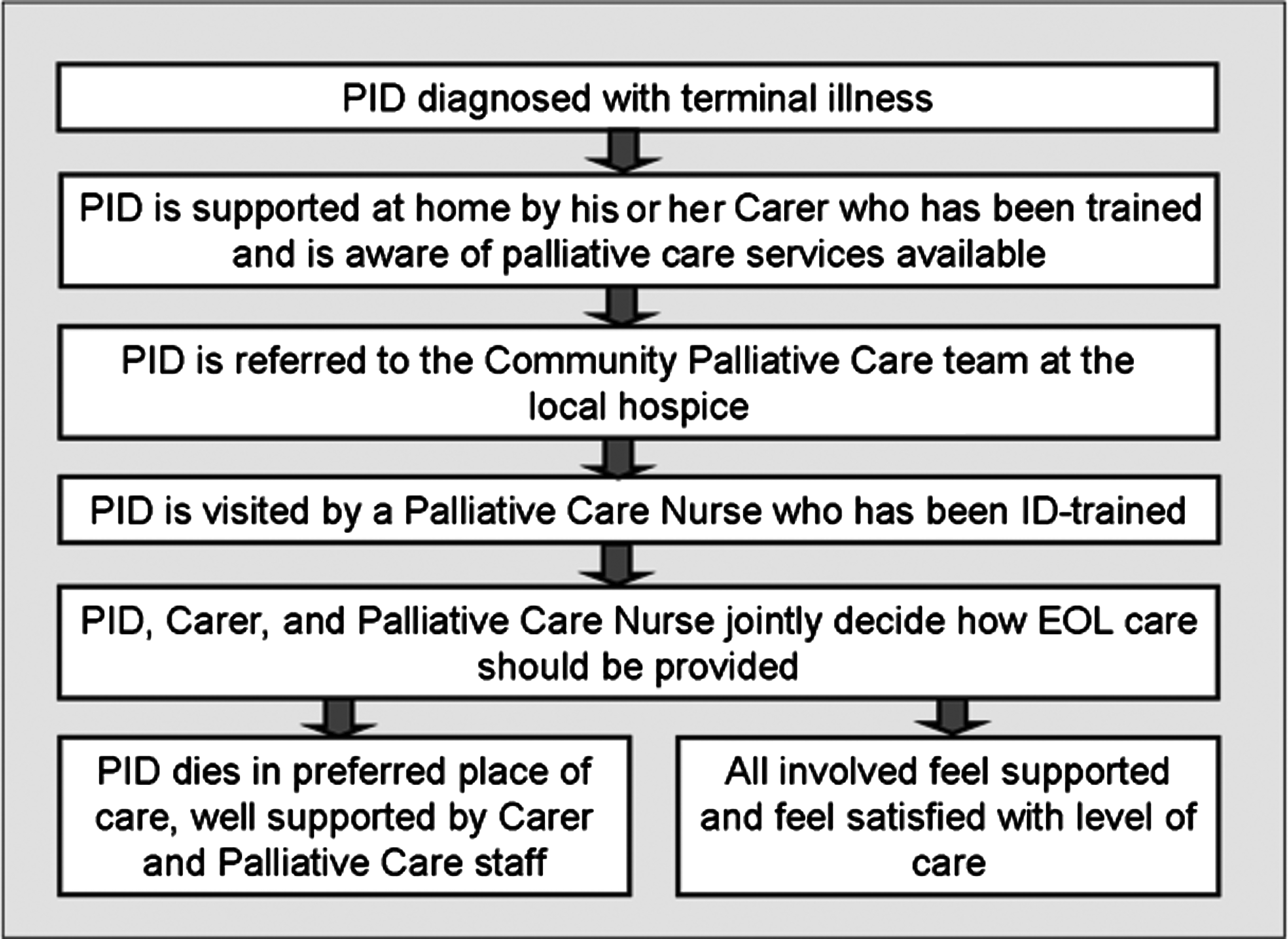
Flowchart illustrating the desired pathway for people with intellectual disability (PID) from terminal illness diagnosis through to end of life (EOL).
The steering group made assumptions about potential barriers to the project implementation, including (a) that ID staff may be prevented from attending training programs because they are short-staffed and underfunded, (b) that ID staff may feel unable to put learning into practice because of organizational constraints, and (c) that the link workers may not be motivated, having high work pressure and little support for what is essentially a voluntary role. To minimize these barriers, the steering group determined to (a) provide the training without charge (subsidized by the King's Fund grant), (b) ensure that the link workers made regular contact with homes with terminally ill people with ID in order to provide the relevant information and support, (c) encourage care-home managers to attend the training to enable the cascading down of the gained knowledge, expertise, and support, (d) offer accreditation for the training to increase staff motivation to attend, and (e) seek and encourage managerial support for the link workers to increase the role's professional relevance.
Project implementation
The training sessions for both ID and palliative care staff were run at each of the four hospices in turn. The steering group felt that inviting ID staff into a palliative care setting could help break down barriers.
• Thirty-one courses for palliative care professionals were run over 2 years. The initial program consisted of four separate afternoons; this was later changed to a more popular schedule of 2 full days. The program was based on training needs identified in previous research,
8
covering the following issues: communicating with people with ID (this session was co-facilitated by several people with ID); assessment of pain and other symptoms in people with severe communication difficulties; capacity and consent; and bereavement. • Training for ID staff consisted of 2 full days. The program covered the following issues: what end-of-life care is; who provides it; how to care for a dying person; exploring loss, talking about dying, bereavement, and remembering; and self-care strategies. A tour of a hospice was later added to the program by popular demand. The training was facilitated by an experienced bereavement counsellor and a social worker with ID experience, with contributions from palliative care nurses, palliative care professionals, and funeral directors. • A “link worker” scheme was developed so that professionals from both the ID field and palliative care field had a point of contact for information and support. In each community ID team and each hospice a professional either volunteered or was chosen by management to fulfil the role, yielding 10 link workers in total. The link workers met three times a year to develop the role, share skills, and receive relevant training. A leaflet and poster were developed to promote the role, made available to professionals attending the training, and to residential care homes in the area.
Project evaluation
Two independent evaluators were commissioned in the second year of the project. Their aim was to map the learning from the project and identify constructive ways forward. The evaluation used interactive cycles involving discussions with the steering group, and face-to-face and telephone interviews with a wide range of stakeholders (project manager, trainers, link workers, delegates of the training programs, hospice and care home staff and managers). The final cycle with the steering group worked on conclusions and recommendations.
Results
Training for palliative care professionals
Initially, training session attendance was very low. Discussions with the hospice directors indicated that there were low numbers of ID patient referrals; this resulted in unwillingness by palliative care providers to attend training until the referral numbers increased. This disinterest resulted in two of the four hospices withdrawing from the project. This reflected a “vicious cycle” that the project was unable to break: that of low referrals into palliative care, reinforcing the unimportance of the area from the palliative care professionals' perspective. Those who did attend the program evaluated it very highly:
“I wish I could have known this as a junior doctor…it would have helped improve care in the hospital.” (evaluation form)
“The communication sessions involving clients and role play was possibly the best training session I've been on for years–the information was easily transferrable to other client groups.” (evaluation interview)
Although one delegate said:
“The acknowledged limitation is that only a limited amount of skill can be gained from sporadic workshops like this.” (evaluation form)
Training for ID staff
Out of 228 residential care homes identified within the South West London area, 46 (20%) accessed the training programs, with care managers attending and general attendance high throughout the 2-year period. A number of homes sent more of their staff to subsequent training programs, indicating its perceived value. Following the end of the training program, the project administrator continued to receive calls from care managers requesting further training. Feedback included:
“Very helpful, informative, and interactive. Lots of information sharing and experience from people who have had to support people at the end of life. Information on palliative care available in the area was also helpful. We have now developed an end-of-life care plan for all the service users after discussion with them, next of kin, and advocate.” (Care Home Manager)
“The funeral director's talk was enlightening and broke some of the taboos.” (Care Home Staff)
“I feel more able to talk about dying.” (Care Home Staff)
“Bereavement counselling is for staff, not just for clients.” (Care Home Staff)
Link-worker scheme
The link-worker scheme delivered mixed, but generally disappointing results. Individuals struggled with lack of management support for their role and uncertainty about what was expected of them. The lack of collaborative working at senior levels in the organizations involved was a major factor in these results. There was no shared strategic commitment to developing the role, and no clear accountability for the link workers. The link-worker network was draped over existing structures rather than embedded in them, making the scheme very vulnerable.
A focus group was held after 2 years, attended by over half of the link workers. It became clear that whereas some had a working interest within the field, others felt obliged to perform the role as no one else in their team volunteered or they were asked by management. When asked how they saw their role, the majority described a passive role as a point of contact for other professionals, whereas a few felt the role should be proactive in maintaining links and collaboration between the different groups of professionals. Points of frustration included a lack of understanding as to why referrals for people with learning disabilities to the hospices were not happening and not knowing where to target or promote the role.
During evaluation interviews at the end of the project, comments included:
“The link-worker training was interesting but a sense of nothing to get your teeth into, little clear direction.” (Link Worker)
“The scheme itself has foundered on senior managers' lack of willingness to treat the role seriously.” (Steering Group Member)
Despite several attempts to redefine and promote the role, the link-worker scheme was cancelled one year before the project was completed.
Independent evaluation of the project
The key findings of the evaluation were as follows:
• There was virtually unanimous agreement that care home staff benefited from the training and were able to put it to good use. • ID community teams too were seen as having benefited from the program–not least by learning what palliative care is and how it can be accessed. • There was less agreement on whether palliative care professionals had derived lasting benefit. • The training was particularly valued for promoting reflection about complex issues and thinking about difference, as well as for acknowledging fears and constructively working with them. • The link-workers scheme was generally disappointing and unsuccessful. • Both palliative care and ID were widely viewed as being rather forbidding and perhaps even frightening areas, each with its own unfamiliar language. Searching questions were raised by interviewees about “who does what, why?” in relation to the care of people with ID at the end of life. • The project was working in very difficult and demanding territory, with a wide range of stakeholders. Critically, the project mostly involved direct health and social care professionals, trainers, and voluntary sector organizations, not system managers and not local users and family carers. This might explain some of the problems experienced in partnership working.
Discussion
In general, there was a lack of understanding of each other's role between palliative care professionals and ID staff, with each unsure of what the other service is providing and how it is run. There was a further challenge in the lack of available data about where people with ID in the local area are living and dying.
The findings of the evaluation and the experience of the project reflected two particular tensions:
• Specialist versus generic working: In the fields of both palliative care and ID, there was a tension between specialism and generic working across boundaries. Until professionals acknowledge these tensions fully, effective change in practice will be patchy, depending entirely on the commitment and dedication of the individuals within a particular organization. • Minority access versus mainstream services: Within the project there was a view of people with ID as a minority wanting access to services, producing the tension of special support versus being in the mainstream. Patients with ID were largely invisible to the hospice services involved. It was clearly important to connect ID carers and specialists into palliative care and overcome their desire to stay outside the mainstream; but no easy ways were found of doing so. One interviewee described the key challenge for the program as being “to adapt mainstream services so that they can meet a variety of needs rather than hive off people with ID.” This issue is all the more important in the context of equalities legislation for the public sector to demonstrate that it is not discriminating, The National End of Life Care Strategy in England has the specific purpose of enabling hard to reach groups (including people with ID) to access mainstream care, ensuring that all adults are able to receive high-quality end-of-life care.
18
Ultimately, the project aimed to effect a change in care, to be reflected through an increased number of referrals for people with ID to palliative care services and an increased satisfaction with end-of-life care for this group. However, embedding change is a huge challenge, and was only partly achieved by this project. Embedding change requires tackling both culture (how people think) and structure (how things are organized). The project tackled the change in care that it wanted to achieve through a cultural initiative (the training) and a structural initiative (the link-worker scheme). The findings showed the former was more successful than the latter, and within that the training for care-home staff was the most positive.
Recommendations
The results and discussion show it is critical to address a number of issues in order for similar work to be effective and sustainable in the longer term. Recommendations include:
1. Secure via joint commissioning a development worker for ID and end-of-life care, to support ID staff to improve their practice and to create a pull on palliative care staff to engage with people with ID. Ideally, this post should be an ID specialist based in a palliative care team. There is an excellent and highly successful example of such a post in Northumberland (North England), where the only Macmillan palliative care nurse who specializes in people with ID was named “Palliative Care Nurse of the Year 2010”.
19
2. Training for ID care staff, involving palliative care staff as trainers, is clearly needed and can be effective. Without the benefits of an external funder, such training might be sustainable through engaging commissioners or making it a social enterprise. 3. It is important to establish how ID services are organized within the local area. During our project, many (though by no means all) people with ID in South West London lived in small group homes. In the future, such residential care homes will cease to be funded and organized in the same way, with a greater emphasis on personalized budgets. In other areas (including other countries) there may well be other models, including more institutional models of care provision. This will affect local training needs. 4. Ensure that the goals of any initiative are clear and measurable to all professionals involved. 5. Ensure that senior management of organizations are proactively involved in an initiative and accountable. 6. Consider linking to national training programs, such as the Gold Standards Framework in the UK. After our study ended, the National End of Life Care Programme published a practical guide that supports anyone caring for people with learning disabilities to ensure that those who may be in the last months of their life receive high-quality end-of-life care.
20
Conclusion
This article has discussed a tension between specialism and generic working across boundaries. A significant contribution to this tension was the issue of specialist support for people with ID as a minority group versus being in the mainstream. The project aimed to effect a change in care. It clearly demonstrated that in order for a change to be embedded in mainstream services cultural and structural issues needed to be addressed. The project was successful in addressing the cultural issues via the training of care-home staff. However, the lack of data in the field and the lack of system support through involvement of senior service managers made the achievement of any structural change within the project very difficult.
One of the key challenges in this project was described as the need to adapt mainstream services to meet a variety of needs; this issue is all the more important in the context of equalities legislation for the public sector to demonstrate that it is not discriminating. In order for people with ID to access palliative care services, end-of-life care commissioners need to think about systematic profiling of, and planning for, vulnerable patient groups with specific needs, ensuring that they make “reasonable adjustments” in order to provide equal access to health care (a UK requirement), and in line with the national End of Life Care Strategy.
Footnotes
Acknowledgments
HC was project manager. MC and SM conducted the external evaluation of the project. IT provided supervision, research knowledge, and overall support. With thanks to the King's Fund for providing the grant that enabled this work. We would like to acknowledge the support and input of the Steering Group. Thanks to those who participated in this project, especially the link workers who put in the time and effort trying to achieve our goals, regardless of the frustrations they faced.
Author Disclosure Statement
No competing financial interests exist.