
Abstract
Abstract
Background:
Communication about religious and spiritual issues is fundamental to palliative care, yet little empirical data exist to guide curricula in this area. The goal of this study was to develop an improved understanding of physicians' perspectives on their communication competence about religious and spiritual issues.
Methods:
We examined surveys of physician trainees (n=297) enrolled in an ongoing communication skills study at two medical centers in the northwestern and southeastern United States. Our primary outcome was self-assessed competence in discussing religion and spirituality. We used exploratory structural equation modeling (SEM) to develop measurement and full models for acquisition of self-assessed communication competencies.
Results:
Our measurement SEM identified two latent constructs that we label Basic and Intermediate Competence, composed of five self-assessed communication skills. The Basic Competence construct included overall satisfaction with palliative care skills and with discussing do not resuscitate (DNR) status. The Intermediate Competence construct included responding to inappropriate treatment requests, maintaining hope, and addressing fears about the end-of-life. Our full SEM model found that Basic Competence predicted Intermediate Competence and that Intermediate Competence predicted competence in religious and spiritual discussions. Years of clinical training directly influenced Basic Competence. Increased end-of-life discussions positively influenced Basic Competence and had a complex association with Intermediate Competence. Southeastern trainees perceived more competence in religious and spiritual discussions than northwestern trainees.
Conclusion:
This study suggests that discussion of religious and spiritual issues is a communication skill that trainees consider more advanced than other commonly taught communication skills, such as discussing DNR orders.
Introduction
Conversely, physicians don't assign the same importance to religious and spiritual issues, and these topics are often neglected when communicating with patients and families. In a study of 177 adult outpatients, 90% believed prayer could influence recovery from illness, 45% indicated religious beliefs would impact medical decision making in the context of grave illness, and 94% indicated their physician should ask about their religious beliefs. 9 However, only 15% of these patients recalled ever being asked about their religious beliefs by their physician. Paradoxically, in a survey of 476 physicians, 85% reported they should be aware of patients' spirituality but the majority would not directly ask about it. 27 Finally, in analyses of satisfaction surveys from 1,732,652 patients in the National Inpatient Database, spiritual needs were ranked as second in the National Inpatient Priority Index. However, only 6% reported that any staff member had inquired about their spiritual needs and 0.9% of the inquiries had come from physicians. 28
Thus, patient, family, and physicians' perspectives on the role of religious and spiritual issues are noticeably discrepant perhaps related to a paucity of physician training in religious and spiritual issues. Our goal was to develop an improved understanding of physician trainees' perspectives on their competence in communication about palliative issues in general and about religion and spirituality in particular.
As part of an ongoing, multicenter, randomized trial to improve clinicians' communication skills, we conducted baseline surveys of physician trainees' knowledge and attitudes about palliative care that included their self-assessed competency in addressing patients' and families' religion and spirituality. The objective of this article is to develop an empirically derived conceptual model that would inform communication skills training programs by examining factors associated with trainees' self-assessed competency in religious and spiritual discussions. We hypothesized that trainees would report low self-assessed competency in religious and spiritual inquiries and used structural equation modeling in an exploratory fashion to develop measurement and full structural equation modeling (SEM) models describing acquisition of self-assessed competencies in end-of-life communication.
Methods
Study design and setting
The Improving Clinician Communication Skills (ICCS) study is a 5-year, two-center, randomized trial of a communication skills workshop designed to improve clinicians' communication skills. ICCS is ongoing at the University of Washington in Seattle, Washington, and the Medical University of South Carolina in Charleston, South Carolina. Data for this ICCS substudy were obtained from the first 4 years of pre-intervention surveys completed by participating physician trainees. All study procedures were approved by the institutional review boards of each institution.
Physician participants
Internal medicine residents and select subspecialty fellows are eligible for participation. Recruitment procedures include a mailing at the start of each academic year followed by two reminders over a 2- to 5-week period for nonrespondents. Overall, 52% (n=297) of eligible physician trainees have participated to date.
Data collection
All participants completed surveys to characterize their self-assessed knowledge and skill with respect to different aspects of palliative care and end-of-life communication. Participants were assigned a unique, electronic identifier, and baseline surveys were completed online via a secure website. Eighty-two percent of ICCS participants (244/297) completed baseline surveys.
Outcome measure
The outcome measure for this study was a single item taken from the 17-item Perceived Competence Questionnaire29,30 in which trainees self-assessed their competence in key dimensions of end-of-life communication. The survey stem states: “Overall, how competent do you feel to do the following” with specific aspects of communication listed beneath it. This questionnaire has been validated for use among internal medicine trainees 31 and uses a 1 through 5 response scale with 1=“not very competent” to 5=“very competent.” For this study we used self-assessed competency in: “discuss[ing] religious or spiritual issues with patients and families” as our primary outcome.
Covariates/predictors
To control for characteristics that might influence self-assessed competency ratings, we included trainees' self-reports of: years of clinical training, age, sex, race, and number of end-of-life discussions with patients or families. We hypothesized that trainee self-assessed competency in religious/spiritual discussions would be related to self-assessed competency in other aspects of communication, especially those having thematic overlap with religion/spirituality. Thus, we included items that provided trainees' self-assessment of the following skills: overall satisfaction with palliative care skills, 32 competency in responding to requests for inappropriate treatments, supporting hope, addressing fears about the end of life, and discussing do not resuscitate (DNR) status.
Data analysis
Data analysis included three phases, each based on regression modeling, first using bivariate and multipredictor regression models to locate likely predictors of the outcome (phase one), then simplifying these models by identifying latent constructs that potentially affected trainees' scores on multiple competency items (phase two), and finally hypothesizing and testing a model that linked the latent constructs with other predictors and with the outcome (phase three). Because our outcome measure was ordinal, we used probit regression for all models, with coefficients produced by a weighted mean- and variance-adjusted least squares estimator.
In phase one, we ran separate regressions with each pre-specified covariate as a predictor of trainee's self-assessed competence in discussing religious/spiritual issues. We followed this with a multiple predictor model, simultaneously entering all predictors. Because we noted substantial collinearity among the self-assessed competencies being tested as covariates, we proceeded to phase two.
In phase two we tested several measurement models in which these competencies were hypothesized to reflect one or more latent constructs. We used a SEM technique known as exploratory factor analysis in the confirmatory factor analysis framework (E/CFA) 33 to initially test whether the self-assessed competencies reflected a single, underlying competency construct. Then, using information from modification indices, we expanded the number of constructs and altered the competencies associated with each construct until an E/CFA measurement model with acceptable fit was obtained. We also kept in mind the face validity of the grouping of measured competencies into the latent competency constructs. For phase two, minimally acceptable model fit required a χ2 test of fit with p value>0.05, with preferred values much higher, 34 reflecting a finding that the variance-covariance matrix estimated for the postulated model did not depart significantly from the actual variance-covariance matrix observed in the data.
In phase three, we expanded the measurement model developed in phase two, adding other predictors and the outcome, forming a full SEM, with hypothesized causal pathways linking the latent constructs and external predictors with one another and with the outcome. We used modification indices and the statistical significance of causal pathways to guide model adjustments. The initial model included all predictors tested in phase one, but substituted the latent constructs from phase two for the individual competency covariates. We hypothesized that the latent constructs were mediating variables between trainee characteristics and self-assessed religious/spiritual competency, that the latent constructs had a specific causal order, and that there was an additional direct path between the earlier construct and religious/spiritual competency. In addition to the paths through the mediating constructs, we postulated direct paths of influence from trainee characteristics to the outcome. From this initial SEM we sequentially removed, in order of decreasing coefficient p values, paths associated with nonsignificant coefficients. As with the measurement model, the criterion for minimally acceptable fit of the full SEM was a χ2 test of fit with p value >0.05.
We used SPSS 17.0 for Windows (SPSS, Inc., Chicago, IL; www.spss.com) for descriptive statistics, and Mplus 6.1 (Muthén & Muthén, Los Angeles, CA; www.statmodel.com) for regression, E/CFA, and the full SEM analyses.
Results
The characteristics and self-assessed communication competencies of our 242 physician trainees participating in this substudy of ICCS are reported in Table 1. When ICCS participants (52%) were compared with ICCS nonparticipants (48%), we found that participants were more likely to be female, white, and in earlier years of training compared with nonparticipants (data not shown). There was not a significant difference by site. In general, our trainees reported low self-assessed competency ratings for most of the communication skills we had a priori selected for these analyses. Specifically, 50% of trainees indicated they felt less than somewhat competent in discussing religious or spiritual issues and 31% felt only “somewhat competent.” The mean self-assessed competency rating for skills such as responding to inappropriate treatment requests, maintaining hope, and responding to fear about the end of life were similarly low, whereas trainees on average felt more than somewhat competent to discuss DNR status (Table 1).
Response scale=0 (not at all satisfied); 10 (completely satisfied).
Response options=1 (not very competent); 3 (somewhat competent); 5 (very competent).
DNR, do not resuscitate; SD, Standard deviation.
Results of our phase one analysis are shown in Table 2. Our single predictor models found associations between our outcome of self-assessed competency in religious and spiritual discussions and covariate/predictor measures of the southeastern training program, increased years of clinical training, and increased number of end-of-life discussions, whereas covariates of age, sex, and race were not associated. Additionally, as hypothesized, each of the other self-assessed communication competencies was significantly associated with self-assessed competency in religious and spiritual discussions. In our multiple-predictor model southeastern training program, discussing hope and eliciting fears about end of life were independently associated with self-assessed competency in discussing religious and spiritual issues (Table 2).
Regression coefficients are based on probit regression models using a weighted mean- and variance-adjusted least squares estimator. The outcome is the trainee's response to the question, “Rate your competence in discussing religious or spiritual issues with patients and families”; response categories were 1 (not very competent); 3 (somewhat competent); 5 (very competent). The multipredictor model is based on 233 cases with complete data and produced R2=0.445.
The reference category is white non-Hispanic.
Three-category ordinal predictor: 0, 1–3, 4+ discussions.
Response scale=0 (not at all satisfied); 10 (completely satisfied).
Response options=1 (not very competent); 3 (somewhat competent); 5 (very competent).
p values that meet statistical significance of <0.05 are bold, non-significant p values are not.
CI, confidence interval, DNR, do not resuscitate.
The multiple-predictor model in Table 2 suggested that trainees' sense of satisfaction with their palliative care skills, along with their self-assessed competence in specific communication skills may be a generalized characteristic, with the specific aspects highly collinear. These specific areas of self-assessed competence, each acting alone, explained 15% to 29% of the variability in self-assessed competence in discussing religious and spiritual issues, with particularly strong associations for discussing how patients can maintain hope and eliciting patients' fears for the end of life.
These observations led to phase two analyses and a search for latent variables that reflected the trainee's overall sense of competence and that served as the best predictor of self-assessed competence in discussing religious and spiritual issues. Although a single communication skills construct with five indicators met the criterion for minimally acceptable fit, the data suggested there were two latent variables that may underlie the five self-assessed competencies. The fit of a two-construct model was substantially better than that obtained with the single-construct model. The constituent components of the two latent variables are shown in Fig. 1 and labeled as “Basic Communication Competence” and “Intermediate Communication Competence.” Basic Competence consists of general satisfaction with palliative care skills and self-assessed competence in discussing DNR with families. Intermediate Competence consists of self-assessed competence in responding to inappropriate treatment requests, discussions of maintaining patients' hope, and eliciting patients' fears about the end-of-life (Fig. 1).
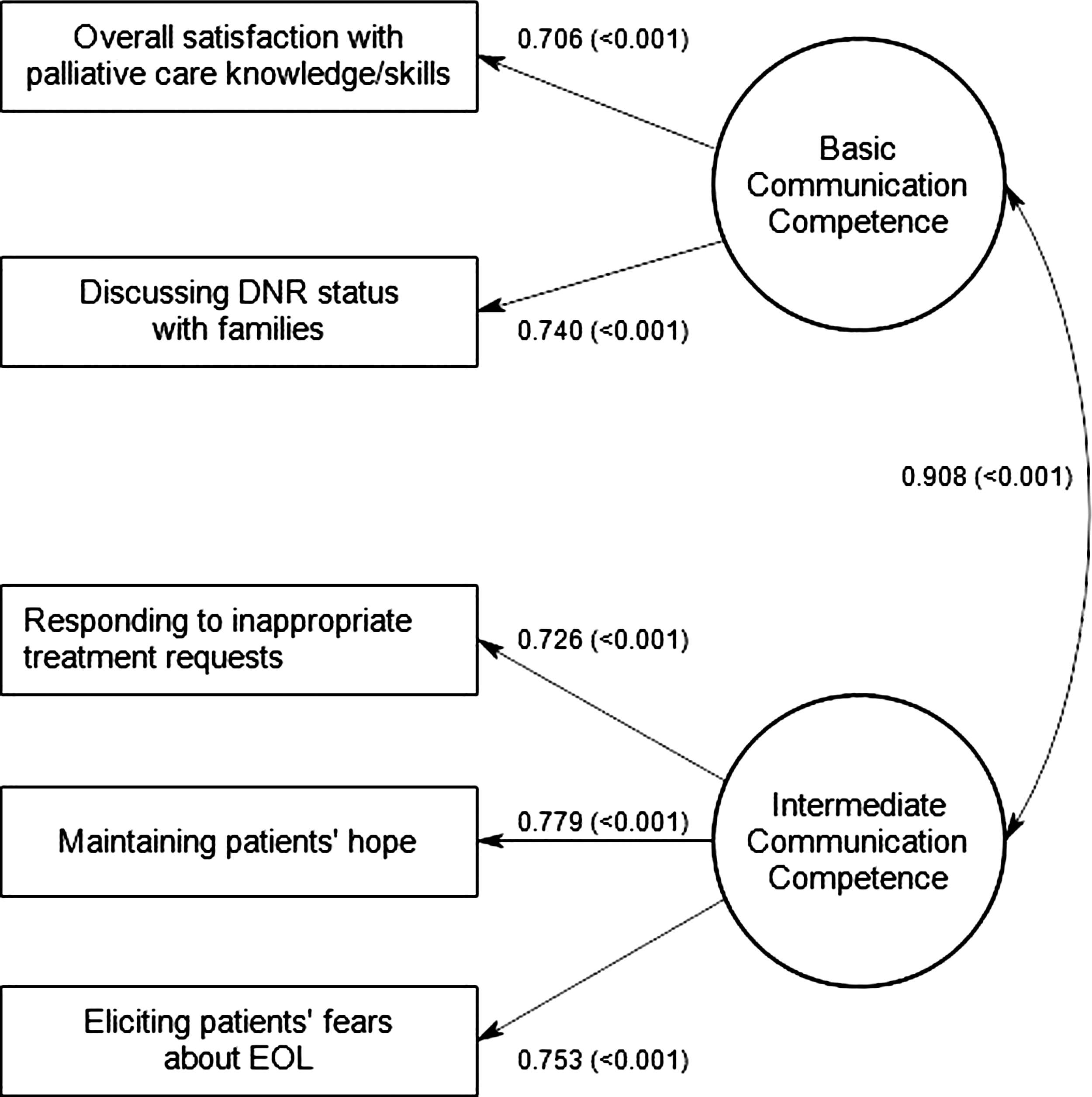
Measurement model of two latent constructs representing trainees' self-assessed competencies in palliative care and end-of-life communication.
In our phase three analysis, other trainee characteristics were integrated with our two competence variables and related to the outcome. We developed a structural equation model with good fit to our data, shown in Fig. 2. Trainee sex and race were not associated with either of the two competency variables or the outcome and thus were not included. Basic Competence had a strong positive association with Intermediate Competence, and Intermediate Competence had a strong association with self-assessed religious and spiritual competence. The effect of Basic Competence on religious and spiritual competence was entirely indirect, mediated by Intermediate Competence, with no additional significant direct impact of Basic Competence on self-assessed religious and spiritual competence.

Structural equation model associating trainee characteristics and two communication competence constructs with trainee self-assessed competence in religious and spiritual discussions.
Years of training and trainee age were associated with the Intermediate Competence variable, and ultimately with self-assessed religious and spiritual competence, but only through their association with Basic Competence (Fig. 2). The direct association of trainee age on Basic Competence was slightly negative. Older trainees reported slightly lower Basic Competence than did younger trainees after adjustment for years of training.
The number of end-of-life discussions was associated with both of the latent competence variables, but affected religious and spiritual competence only through these mediating variables (Fig. 2). There was a positive direct effect on Basic Competence and a complex relationship with Intermediate Competence such that end-of-life discussion experience ultimately resulted in a positive impact on self-assessed religious and spiritual competence.
Training program had a significant direct association with trainees' self-assessed competence in discussing religious and spiritual issues, but no association with the latent variables measuring Basic and Intermediate Competence. Trainees in the southeastern program felt more competent in the religious and spiritual domain than those in the northwestern program, but trainees were, on average, indistinguishable with regard to self-assessed competence in other communication skills.
Discussion
To our knowledge this is the first investigation describing the relationship between physician trainees' self-assessed competency in discussing religious and spiritual issues and other self-assessed communication skills. Furthermore, we identified trainee characteristics associated with self-assessed competencies with regards to religious and spiritual discussions.
The association of self-assessed competency supported by our SEM models suggest a progression in how trainees perceive the development of these communication skills starting with basic competency consisting of palliative care skills plus the communication task common among physician trainees of establishing DNR status and building toward a more sophisticated intermediate competency in which they perceive greater proficiency in communication tasks such as responding to inappropriate treatment requests, hope, and fear. Finally, trainees who provide higher ratings for these intermediate communication skills are more likely to assess themselves as competent in discussing religion and spirituality, suggesting a hierarchy of perceived difficulty.
Neither years of training nor age had a direct influence on self-assessed competency in discussing religious and spiritual issues, but each was indirectly influential through its direct effects on Basic Competence. This implies that this specific communication skill does not simply develop over time without the development of more basic communication skills that increase with experience. This is congruent with findings obtained from attitudinal surveys of practicing internal medicine physicians in which only a minority agreed or strongly agreed that physicians should ask about patients' religious and spiritual beliefs. 27 Paradoxically, 85% of these physicians reported that they should “be aware” of patients' religious and spiritual needs. The finding that after adjusting for years of training, increasing trainee age was negatively associated with basic competency may suggest these trainees have lower self-assessments as a result of humility attributed to more work and life experiences or a result of the erosion of self-assessed competency over time, although our data cannot address these hypotheses directly.
The relationship between number of end-of-life discussions and the two latent competency constructs seems paradoxical as this characteristic had a positive direct effect on Basic Competence but a negative direct effect on Intermediate Competence. Given our exploratory methodology this may be due to chance, although Maslow's Four Stages of Learning 35 may provide an interesting theoretical explanation. This theory purports that acquiring skills proficiency occurs in four stages. The first stage is unconscious incompetence during which learners don't realize what they are unable to do. During the second stage, learners undertaking a task are aware of their deficits but unable to remedy them. The third stage is conscious competence in which some understanding is present but mastering the skill requires substantial effort. Thus, trainees who reported fewer end-of-life discussions may have been more likely to be in the first stage and may have unduly optimistic perceptions of their competency. Trainees with more experience in end-of-life discussions may have experienced “failures” and have greater self-awareness of their limitations.
Finally, Southeastern training location was directly and positively associated with increased self-assessed competence in religious and spiritual discussions. This may simply reflect the two individual training programs but is congruent with the greater prevalence of religion and religiosity in the southeastern United States as compared with the northwestern United States 36 and thus southeastern trainees may have personal beliefs that give them more self-assessed competence in this specific communication skill. Alternatively, the southeastern trainees may encounter religious and spiritual values among their patients and families more frequently and thus may acquire greater self-assessed competence. Interestingly, there was no difference in self-assessed Basic or Intermediate communication skills by training site.
There are several limitations to our findings. First, the proportion of eligible trainees participating in the parent ICCS trial is 52%, and there were differences between participants and nonparticipants limiting generalizability. Second, we did not inquire about trainees' personal religious and spiritual beliefs, so we cannot describe how this may have influenced their self-assessments. Third, although these trainees represent the future physician workforce, it is possible that different findings would be obtained from practicing physicians. However, the discrepant perspectives held by patients, families, and physicians regarding the relevance of religion and spirituality have been repeatedly observed and do not vary by physician experience. Fourth, although we elected to use the labels “Basic Competence” and “Intermediate Competence” for the two latent constructs and although we believe these labels have some face validity, the designations may be due to an error referred to as the “naming fallacy.” 37 Fifth, we have recently shown that physician self-assessments of general end-of-life communication skills do not correlate with patient assessments, 38 thus self-assessed competency is an incomplete reflection of physicians' communication skills. Finally, because both the measurement and structural SEM models were based on exploratory procedures, they are subject to questions about chance.
In conclusion, our analysis of physician trainee self-assessed competency ratings indicates that discussion of religious and spiritual issues is a communication skill distinct from other commonly taught communication skills, such as discussing DNR. These findings offer important empirical insights into how physicians might acquire such communication skills. Specifically, these findings could be used to augment existing spiritual assessment tools 26 and religious and spiritual support training programs. 25 Our data are congruent with other literature indicating physicians perceive religious and spiritual communication as challenging and suggest there is a need for specific training on addressing religious and spiritual issues because other communication skills may not automatically transfer to this important issue.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.