
Abstract
Abstract
Background and methods:
Ensuring appropriate palliative and end-of-life (EOL) care in the acute environment is complex and challenging. The Liverpool Care Pathway (LCP) aims to support staff to provide holistic EOL care utilizing a structured framework to prompt and guide care. We report on the post-implementation findings of a mixed methodology (survey and focus group [FG] forums) study into staff perceptions of EOL care following the pilot implementation of the LCP into two acute wards.
Results and conclusions:
Study results suggest that within acute settings staff perceive that the LCP improves EOL care overall, assists interdisciplinary communication around death and dying, and that is a useful tool to positively influence decision making and care delivery. Further research into aspects of staff communication, diagnosing dying, changing direction of care, and the physical environment is warranted.
Introduction
The Liverpool Care Pathway (LCP) was developed in the United Kingdom 12 to transfer hospice best practice EOL care into other care settings. It aims to support staff to provide holistic EOL care utilizing a structured framework to prompt and guide care. 12 The LCP is structured around an initial assessment, ongoing care, and care after death. Positive outcomes regarding integrated care pathways (ICP) for EOL care in various settings have been identified8,13–19 although randomized control trials are absent.13,20
The LCP has been found to improve the plan of care, provide guidance, and improve documentation and communication.21–23 Few acute care pre- and post-studies have been published.16,18 Di Leo and colleagues 18 explored staff (n=14) expectations of the LCP via focus groups (FG) pre-implementation and its impact on staff post-implementation (n=12). Outcomes included increased confidence among physicians regarding pain management and discontinuing inappropriate treatments. Nurses cited the beneficial impact of pro re nata (PRN) prescribing, but noted ongoing time and personnel constraints. 18 Veerbeek and colleagues identified improved documentation and a reduction in symptom burden following LCP implementation in hospital, home, and nursing home settings. 16
We report on the post-implementation findings of a mixed methodology study into staff perceptions of EOL care following the pilot implementation of the LCP into two acute wards. Staff perceptions of EOL care pre-implementation 7 established a baseline description of EOL care and indicated the potential to improve care utilizing the LCP.
Methods
Mixed methodology (survey and FG forums) were utilized to address the question: Do staff perceive that an integrated care pathway for the imminently dying patient, their family, and whānau positively influences care. (Note: whānau (noun) is a New Zealand Māori word that refers to extended family or family group. It is a familiar term of address to a number of people.) Of particular interest was the LCP's perceived impact on care, staff knowledge, confidence, communication, and teamwork, and its value as a clinical tool to guide practice and decision making and address barriers to care.
Staff working or having worked on the two pilot wards (n=227) following the implementation of the LCP were surveyed and invited to FG forums. The study population post-implementation is not a replica of the pre-implementation survey population 7 as the purpose was to evaluate the impact of the LCP following the pilot. Additionally, staff mobility and survey anonymity make it impossible to link individual survey respondents pre- and post-implementation.
Surveys (10 pages) with a self-addressed return envelope were distributed via the hospital mail system. Reminder notices were posted in the wards and via e-mail. An 18% (n=41) response rate from the two wards was achieved. The survey replicated the pre-implementation survey 7 including demographic data (Q1-8), statements to be ranked on a Likert scale, and open-ended questions (Q9-35), with the addition of LCP-specific questions. The LCP questions included Likert-scale statements related to the LCP (Q39-50) and an invitation to comment regarding improvements to the overall care of the dying (Q50), barriers to the care of patients (Q51), their family, and whānau (Q52) as well as suggestions as to how the care of patients (Q53), their family, and whānau (Q54) could be improved. Additional comments (Q55) were also sought. The LCP-specific questions (Q39-55) are the focus of this paper.
FGs enabled the collection of additional qualitative data through group interaction24,25 and included one medical (n=6), two nursing (n=9), and one allied health (n=3) groups totaling 18 staff. Of these participants 10 returned the post-survey, one did not, and 6 did not respond to the question. FG forums utilized the same process as the survey and were facilitated by an experienced externally contracted person. A member of the research team (KS) attended the forums to answer questions, obtain consent, and take field notes. The scope of the topic was broadly defined and related to participants' experiences of EOL care, experiences of using the pathway, and their perceptions of its influence on care. Inclusion criteria (survey and FGs) required staff to have been involved in the care of least one person using the LCP.
Consecutive implementation into the two wards resulted in staff being surveyed 6 and 11 months after LCP implementation. FGs were held 10 and 15 months post-implementation.
Ethical considerations
Approval was obtained from the Central Regional Ethics Committee. Return of the anonymous survey implied consent and individual consent was sought from FG participants.
Data analysis
Quantitative data
Demographic data related to the study population are included in Table 1. Survey respondents were predominantly female, relatively experienced in their professions and EOL care with the majority (n=30 or 73%) caring for >10 people.
Qualitative data
Data for qualitative analysis were obtained from questions inviting comment in response to a Likert-,scale question (Q50), open questions (Q51-55), and FG data. Comments within the survey were purposefully sought 26 to allow for explanation of perceptions and provide an opportunity to express unsolicited views. FG discussion was transcribed verbatim.
A basic descriptive analysis27,28 in relation to the research question and objectives regarding care provision, staff knowledge, confidence, communication, teamwork, guiding practice, decision making, and addressing barriers to care was undertaken by two of the authors (JBC and KS). The results were subsequently discussed with team members.
Results
Responses to the LCP-specific Likert-scale statements (Q39-50), with the most pertinent quantifiable survey data are presented in Fig. 1. Respondents (>70%) either strongly agreed or agreed that the LCP had positively influenced care across all key areas (Fig. 1). Overall care had improved and >90% indicated an improved understanding of the goals of care. Staff knowledge and confidence were identified as improving. The most noted improvement was anticipatory prescribing for the five most common EOL symptoms. Introducing the LCP also stimulated conversations about the status of the patient and an appropriate plan of care. Importantly, the document itself was regarded as easy to use. Barriers to care provision were also identified.
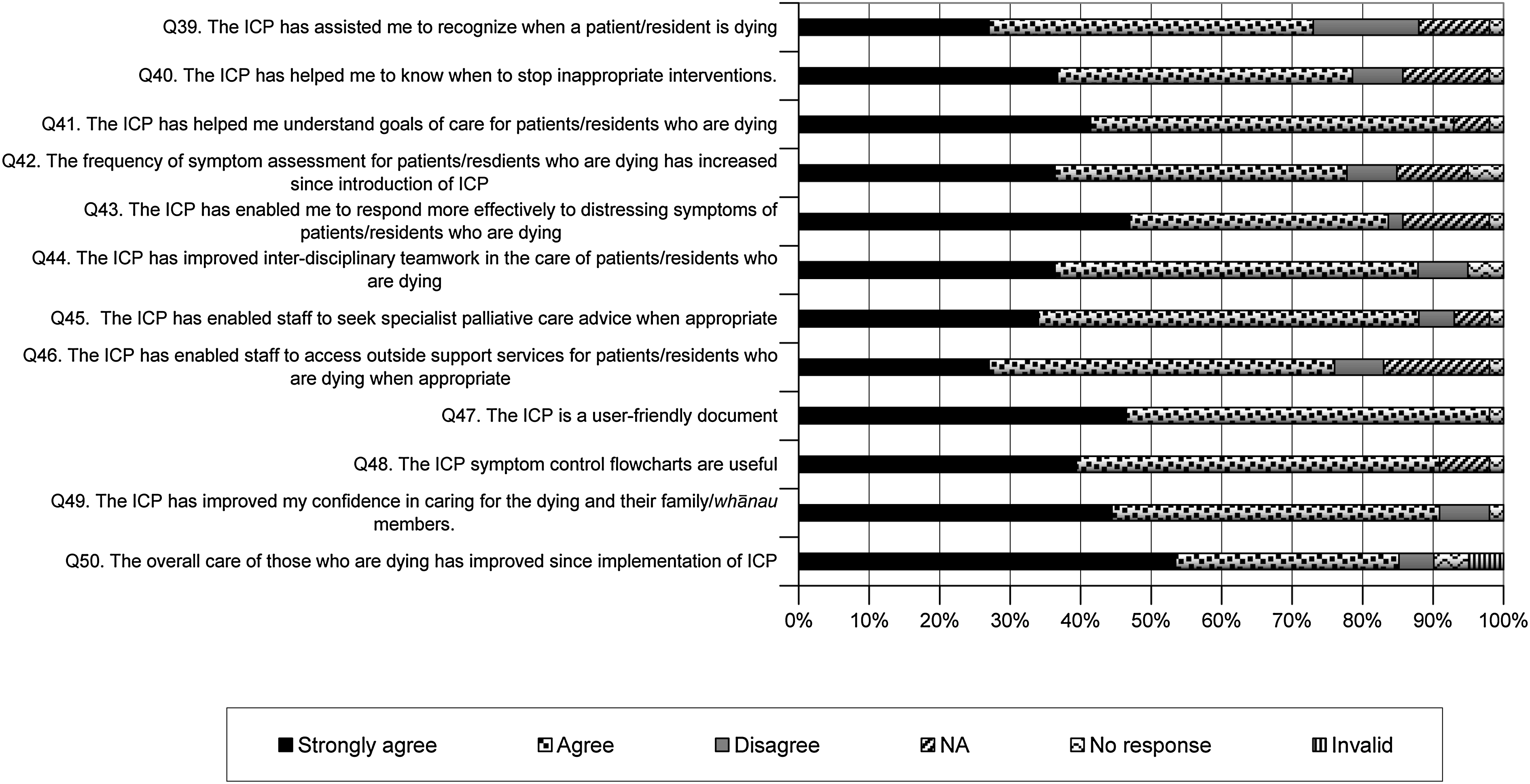
Likert-scale responses as a percentage of participants—acute care.
Care of the dying
In addition to the LCP Likert-scale responses (Fig. 1), comments (survey and FGs) illustrated how the LCP made a substantial difference. Anticipatory prescribing of PRN medications was identified as particularly beneficial across disciplines. Staff perceived that the introduction of the LCP also positively influenced the EOL care of patients not on the LCP.
I do think those who are dying here have a much more comprehensive planned approach to their care, there isn't the waiting for meds [medications] to be charted and indecisions over these especially after hours, nurses are better empowered with the LCP tool. Registered Nurse (R.N.), 33. Survey.
Those on the LCP are far better looked after however I feel the general care of the dying patients who are not on the LCP has improved. R.N., 40. Survey.
… I noticed that there is a more respectful attitude towards dying since the Care Pathway has been integrated through the Hospital. It's been an attitude—a gentler tone in people's voices when they say someone may be dying—but not in a sloshy sentimental way but sort of, something is happening that we need to respect. Allied Health FG (AHFG).
Overall care improved, goals were clearer, as was staff's ability to achieve these, with respondents more confident about recognizing dying and assessing symptoms.
Documentation
The document was seen as user friendly (Q47), a valuable guide, and prompted the delivery of care. This promoted confidence (Q49) regarding care delivery and that key areas of care were not overlooked.
Goals are clearly set in the pathway. Reduce delay in symptomatic mix. Appropriate drugs for symptoms are pre-prescribed, hence reduced delay in drug administration when required. Gives Drs (especially junior staff when they first start on the jobs) more confidence in their prescriptions for symptom mix. MF (Medical Fellow), 10. Survey.
A more structured approach to EOL care was seen as positive.
Communication and teamwork
Staff identified the LCP as a catalyst for EOL-care-related discussions. When the LCP was commenced, ambiguity and uncertainty regarding the plan of care were resolved.
We have had several patients go through this process and I have found it very positive—it kind of formalizes things. It gives the nursing staff the ability to look after their patients better without fighting, without having to rely on on-call staff to come and do things. It sets up very clearly how these people are to be managed, so at least the nurses don't have to argue to get something prescribed or not, its all done by the team, before after hours—I have found it very positive. MFG (Medical FG), p2.
Involvement of the multi/interdisciplinary team in EOL decision making appeared to improve, as did communication with families and among staff.
Although >70% of respondents (Q39) believed the LCP helped identify dying patients, knowing when to stop interventions often remained challenging. The need to improve communication skills within the team regarding appropriate spiritual and cultural care among a multi-ethnic workforce was commented on, particularly by several allied health respondents.
Knowledge and confidence
Introducing the LCP was perceived as supporting staff in developing their knowledge and confidence in managing EOL care (Q40, 41, 43, and 49). This was supported in the FG discussion.
And I think it's good because it has given people a lot more knowledg—that people can die with dignity. NFG (Nursing FG), p7.
It guides the experienced staff—or staff that don't know how they will cope with this—and I think it's improved the care for the new grads [graduate nurses] and new staff because it's basically setting out what you should be doing—and you have to tick a box so hopefully you have done the care and I think it's improved the overall care of the patient and family. NFG, 2 p8.
The need for ongoing education regarding the LCP and EOL care was identified including its appropriate use, knowledge of palliative care practices, and assessment skills. Support from specialist palliative care services as required was highly valued.
Barriers to care provision
Perceived barriers related to three main areas: “diagnosing dying,” which impacts on changing the plan and direction of care; time/workload; and the physical environment. Nurses in particular commented on delays regarding changing the direction of care, particularly after hours when the patient's primary medical team was not available. A respondent perceived some physicians were more comfortable with euphemisms such as “for comfort cares” when patients entered the terminal phase, as opposed to making an explicit decision to commence the LCP.
Weekend teams do not like to make the decision of stopping treatments on patients who are not under them. Better weekend plans written in patients notes, if patient's condition may deteriorate to need to go on ICP. Enrolled Nurse (E.N.), 28. Survey.
Difficult “line” at times between treatment and quality of life and acceptance of needs for palliative care. SW (Social Worker), 17. Survey.
I have found that when we've tried, sometimes to get the patients started on it, that's when the problems start with getting doctors to actually commit, to a name on the forms…Whereas, before the LCP if you asked for a patient to be made “comfortable” they seemed to have less hang-ups about it. NFG, Pg1.
The complex and necessary tension around continuing to treat and/or recognizing dying was commented on by all professional groups. Nurses' role in questioning the direction of care was described positively by a consultant.
It's quite a traditional tension in some ways, I think the nurses have to try and keep the doctors realistic and point out things. We tend to press on, and the nursing staff say “do you really think this is appropriate,” and certainly a little more pressure for the patient to go on the pathway—and I might say ‘”no, not yet”…MFG, p10.
Medical staff (via FG) expressed some concern regarding appropriate use of the LCP. Clarity was seen as crucial regarding the difference between having no further treatment options and imminently dying. Conversely, a chaplain expressed concern regarding discontinuing the LCP and the potential distress this could cause when a person was no longer believed to be dying.
The paucity of single rooms and places for private meetings remained a concern.
Environment—lack of privacy. Lack of tea/coffee making facilities. Lack of patient lounges in some areas. Not a child friendly/tolerant environment. R.N., 14. Survey.
Perceptions of inadequate time and high workload were identified.
But in our Ward it's so hard because you are running and actually you don't want to be running when someone is dying. You need to be able to go in every hour or half an hour and say “is everything all right” and do it regularly and sometimes that is so hard. NFG 1, p11 and 12.
Challenges to care delivery regarding personnel, time, and the physical environment remained. However, the organization's implementation of the LCP changed the overall perception of care, reduced some significant barriers, and improved organizational processes.
Discussion
This study sought to discern if the LCP positively influenced care in two acute wards in a New Zealand hospital. It was the first of its kind in New Zealand, and only the second pre-post LCP acute care study internationally to be published.
All professional groups affirmed that the LCP positively influenced EOL care, by clarifying the plan of care, providing guidelines, and improving continuity of care, assessment and symptom control. Our findings indicate the LCP has been a critical factor in changing the processes around EOL care, including identifying dying, changing the direction of care, and improving documentation, knowledge, confidence, communication, and teamwork.
Participating staff believed the LCP assisted them to recognize dying, upon which appropriate care of the dying is dependent. 12 Decision making had improved, although nursing staff identified preferences by some physician colleagues for euphemisms such as “for comfort cares” rather than explicitly naming, addressing, and managing the dying phase by initiating the LCP. Recognizing dying can be particularly challenging in acute care settings.2,5,7–10
Difficulty in diagnosing dying was not a strong feature in a pre-post LCP Italian study, although increased confidence in discontinuing inappropriate treatments was noted. 18 Continuing inappropriate treatment was identified as a barrier to quality EOL care. 5 29 30 In some instances taking a parallel approach may be appropriate10,31 by initiating “pre LCP” conversations around the possibility of dying while continuing acute management. Findings of this study appear to support the use of LCP as a tool for decision making around death and dying.
The LCP document was perceived as changing and supporting practice by prompting and guiding staff across disciplines, a result that is similar to other studies.21,22,32 Most notably, anticipatory PRN prescribing was regarded positively across disciplines for enabling a timely nursing response to symptoms, an outcome previously reported.18,22
Nurses conveyed a strong commitment to delivering EOL care, a finding noted pre-implementation 7 and by other investigators.5,22,30,33 The importance of nursing in EOL care was evident in responses from physician and allied health participants, although it is not possible to determine if this had increased. A perceived increase, by physicians, in the value of nurses following the introduction of the LCP has been identified. 18 Reflecting earlier findings,18,21,22,32,34 the LCP was seen as improving communication within the team. Improved teamwork and collaboration was evident in the data with recognition of the differing orientation of disciplines and the positive contribution this makes to care. An increased awareness of communication difficulties was not evident, a finding noted as an outcome of LCP implementation in Italy. 18 Nursing staff in particular commented on the reduction of inappropriate practice variation between staff and across changes in shifts/teams. These findings reflect the aims of ICPs. 35 Further research into interdisciplinary team dynamics and their influence on care outcomes is indicated.
A desire for ongoing education related to EOL care was evident and is both necessary and appropriate. The necessity for thoughtful utilization of the LCP in relation to clinical skill has been clearly articulated. 36 To achieve this collaboration with specialist palliative care services is recommended.
Perceived barriers to EOL care related to the lack of appropriate physical spaces, and the perception of nurses in particular regarding inadequate staffing and time. These barriers, identified pre-implementation, 7 are outside the influence of the LCP. Italian colleagues also identified staffing and time as barriers to EOL care. 18 Further evaluation of space modification/alteration and design requirements of modern hospitals is required.
Study limitations include it being undertaken in one 194-bed hospital and the low survey and FG response rate. Participant bias may exist, and the introduction of the LCP may have mitigated staff concern. The difference between the implementation and evaluation time frames in the two wards was a risk regarding a less positive perception in the second ward, but this is not evident in the data. Survey and FG participants were obtained from both wards and medical and allied health staff who also work across the hospital. Staff turnover in wards during the intervention could have influenced the findings. Data obtained via FGs reflect the survey responses (both positive and negative). Triangulation of the data sources and informal discussion with clinical staff (e.g., physician interns, charges nurses, and after-hours nursing supervisors) and endeavors of nonpilot ward staff to obtain the LCP support the findings.
Conclusions
In this small study, evidence suggests that within acute settings staff perceive that the LCP improves EOL care overall and assists interdisciplinary communication around death and dying, and that it is a useful tool to positively influence decision making and care delivery. Improved confidence in diagnosing dying and an improved interdisciplinary team approach to death and dying are evident. Ongoing education, including the development of clinical skills, a holistic approach (including the physical environment), and communication is required, along with exploration of sustainability issues. Further research into aspects of staff communication, diagnosing dying, changing direction of care, and the physical environment is warranted.
Footnotes
Acknowledgments
The authors sincerely thank staff for their participation and our employers for supporting this project. Our thanks also go to Barry Keane for early project support, Pat Hickson for survey development, Lesley Batten for focus group facilitation, and Jo Giesen and Pip Lewer for administrative support.
Author Disclosure Statement
No competing financial interests exist.