
Abstract
Abstract
The authors propose that the characteristics of personal (individual) compassion may be extrapolated to the concept of corporate (organizational) compassion. Modern health care facilities attract staff members who are able to exercise varying degrees of compassion in their busy daily routines. However, little discussion has taken place on how health care organizations might best harness and integrate aspects of individual compassion to create an organization with compassion as a core value. We define three characteristics of a “compassionate hospital” as 1) the presence of a healing environment, 2) a sense of connection among people, and 3) a sense of purpose and identity. We suggest how a “top down” focus on compassion as a core value by clinical leaders could maximize the compassion of health care workers, and reduce the suffering expressed and/or experienced by health care workers and patients in today's health care facilities. The compassionate hospital concept is intended to act as a proposition for health policy researchers and decision-makers in health care so as to reduce the suffering of sick patients, and to restore a sense of well-being, meaning, and purpose among health care workers.
“On ne demande pas à un matheureaux: de quel pays es-tu? Ou de quel réligion es-tu? On lui dit: tu souffres, cela suffit.”*
Introduction
Both authors have a deep understanding of the nature of personal compassion. This paper, however, is written in an attempt to extend the principles underpinning individual (personal) compassion to the corporate (organizational) health care system. Our aim is to outline what we believe to be characteristics of the “compassionate hospital,” and to propose how implementation of the core aspects of personal compassion may extend to significant cultural changes within health care organizations. Our premise is that the exercise of existing individual compassion by health care staff may be enhanced by a “top-down” approach, led by compassionate clinical leadership engaging with health care bureaucracy.
The Compassionate Hospital: A New Emphasis on Care
The definition of a compassionate hospital that we believe to be most meaningful and practical is “a health care facility whose staff has a deep awareness of, and respond to, the suffering that arises from illness.”
This definition relies on the following three concepts:
1. “Hospital” is a collective noun that refers to those who work within the physical structure of what we commonly refer to as the hospital building. Therefore, “we are all the hospital,” and the ideal of compassionate care should extend to staff and patients alike. 2. An understanding of compassion. There are two major components in the common dictionary definition of compassion: first, “a deep awareness of suffering,” and second, “a desire to alleviate that suffering.”
1
At the heart of compassion, therefore, is the readiness to appreciate the plight of another whole person and to develop strategies that help to confront suffering.
2
The common themes inherent in many definitions of suffering are aloneness, feeling lost, disintegration, abandonment, feeling vulnerable, and fearful—as expressed in the “Sola, perduta, abbandonata” aria of Puccini's opera Manon Lescaut.3–5
3. The distinction between “disease” and “illness.” Whereas the compassionate hospital seeks to cure (i.e., eradicate) disease, an equally and more expansive task of health care is to minimize disability and to assist patients to optimise their subjective experience of disease presence, that is, to manage “illness.”
6
Sources of Suffering in the Context of Illness
The distressing effect of the underlying disease process and treatment cannot be over-emphasised. Troublesome symptoms such as unrelieved pain, shortness of breath, lethargy, lack of appetite, thirst, and feeling sick all the time are common and powerful determinants of suffering. However, suffering may exist in the absence of significant physical symptoms and may even continue despite careful attention to physical distress. The suffering that may result from survivorship after cure of cancer has been recently highlighted. 7 Undiagnosed depressive and anxiety disorders, family dysfunction, fatigue, communication breakdown, and emotional distress have been found to be additional, important sources of suffering. 8
Despite the universal expectation that health care professionals have a core role in relieving suffering, it is acknowledged that health care professionals are poorly trained and unprepared to diagnose, assess, and manage patient suffering, even if pain management, psychological issues, and psychiatric diagnoses are covered in the medical curriculum.9,10 Furthermore, there are many disincentives and obstacles within modern health care that stifle the development of physician-healers. 10 Because suffering frequently has an existential component related to a shattering of meaning, purpose, and hope,3,11 physicians cannot rely solely on theory, knowledge, and skills that address physiological dysfunction. Rather, as Coulehan suggests, there is a need “to engage the patient at an existential level.” 12
Suffering may also be induced by simply being ill. For some patients, being ill represents a profound loss of independence, for some it represents punishment, and for others it represents shame and guilt, and feeling unclean as well as dependent and having lost status. Although two patients may have seemingly identical diseases, their subjective experiences may be very different. 13 Hospitals are large, impersonal places where patients may experience profound loss of control, where they are subject to foreign rules and regulations, and where staff often have too little time and often speak with the foreign tongue of medical jargon.
The Suffering of Clinicians
In proposing how a hospital might be structured, and function, with compassion as its core value, the authors understand very clearly the multiple and complex reasons why today's hospitals and health care system suppress (inadvertently or otherwise), and fail to enhance, a compassionate workplace. Although a full understanding of these contemporary issues is important, the topic has been discussed by other authors. 14 For instance, it is recognized that one of the current crises facing those who work in health care facilities is disengagement, particularly between administrators and clinicians, and even among clinicians themselves.15-7
There has been a recent resurgence in the topic of the suffering experienced by health care professionals. Cole and Carlin 17 have drawn attention to the suffering of physicians, who may themselves suffer from the “dehumanization of modern medicine.” Edwards et al. 15 emphasise the need for clinicians to develop a “new compact” with large health care organizations and to develop ownership of a new agenda to encourage creativity, personal renewal, and learning, including engagement in activities such as mentoring and reflective feedback.
Bureaucracy aside, the suffering of clinicians is multifaceted. It is uncommon in the public hospital system for clinicians to express their suffering, to “tell it like it is.” Partly as a result of their training, many clinicians may feel alone and isolated as they go about their daily routines.17-20 There are few opportunities for clinicians to come together as a group to socialize, to reflect as individuals among their peers, and to devise strategies for individual clinicians not only to survive, but also to thrive, in the workplace. 21
Remen believes that, year by year, rotation by rotation, young clinicians may trade their wholeness, their identity, for the acquisition of skills and expertise.22,23 Clinicians increasingly become defined by the technical aspects of their job, rather than by the worth of their intrinsic selves. If one confuses one's “essential self” with the technical aspects of one's work, it becomes nigh impossible to reflect on oneself. A genuine sense of self may have been progressively subsumed by one's professional persona over many years of training. Therefore, the real risk is that many students and clinicians may continue to practice in a nonreflective fashion, carrying out the work for which they were trained, but never really reflecting on whether that work is feeding and sustaining them, or on how their activities and behavior impact upon their patients (or vice versa). 24
For some time now, health care professionals have come to integrate quality assurance (QA) into their professional lives to ensure that the technical aspects of their work are state-of-the-art. Clinicians continue to strive to improve their work and expertise through a range of programs in various departments, hospitals, and colleges. However, it is suggested that what is missing is an equal emphasis on QA in relevant self-care programs that assist clinicians to reflect on personal elements of their work. There should be no antagonism between the technical approach to disease and the personal aspects of patient care. Indeed, if clinicians are to practice and to care in an holistic fashion, the technical and the personal aspects of the profession must be seen to be inseparable.
It is also important that we resist the temptation to redefine the word “care” by linking it to our technical skills and expertise. 25 Clinicians may mistake technical ability and expertise as a substitute for caring. For instance, clinicians can occasionally delude themselves into believing that they “care” because they order lots of tests and x-rays, have used a certain type of therapeutic technique, work long hours, or spend time reading the latest journals.
Characteristics of a Compassionate Hospital
The overlapping characteristics of a compassionate hospital, originally proposed by Youngson, 26 are the presence of a healing environment (a sense of place), a sense of connection among people (togetherness), and a sense of purpose and identity (inner resources). (See Figs. 1 through 3.)
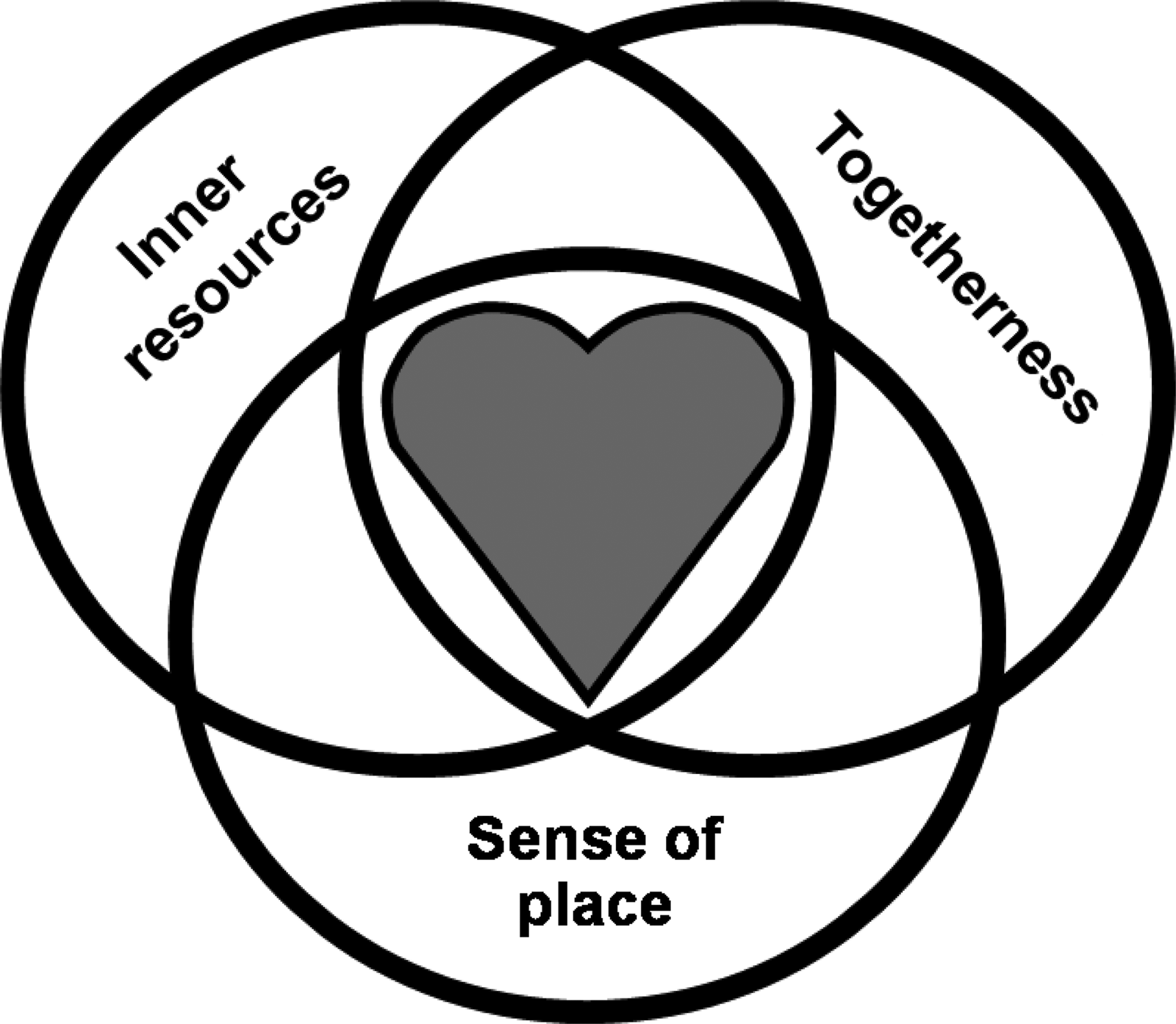
Elements of a compassionate hospital.
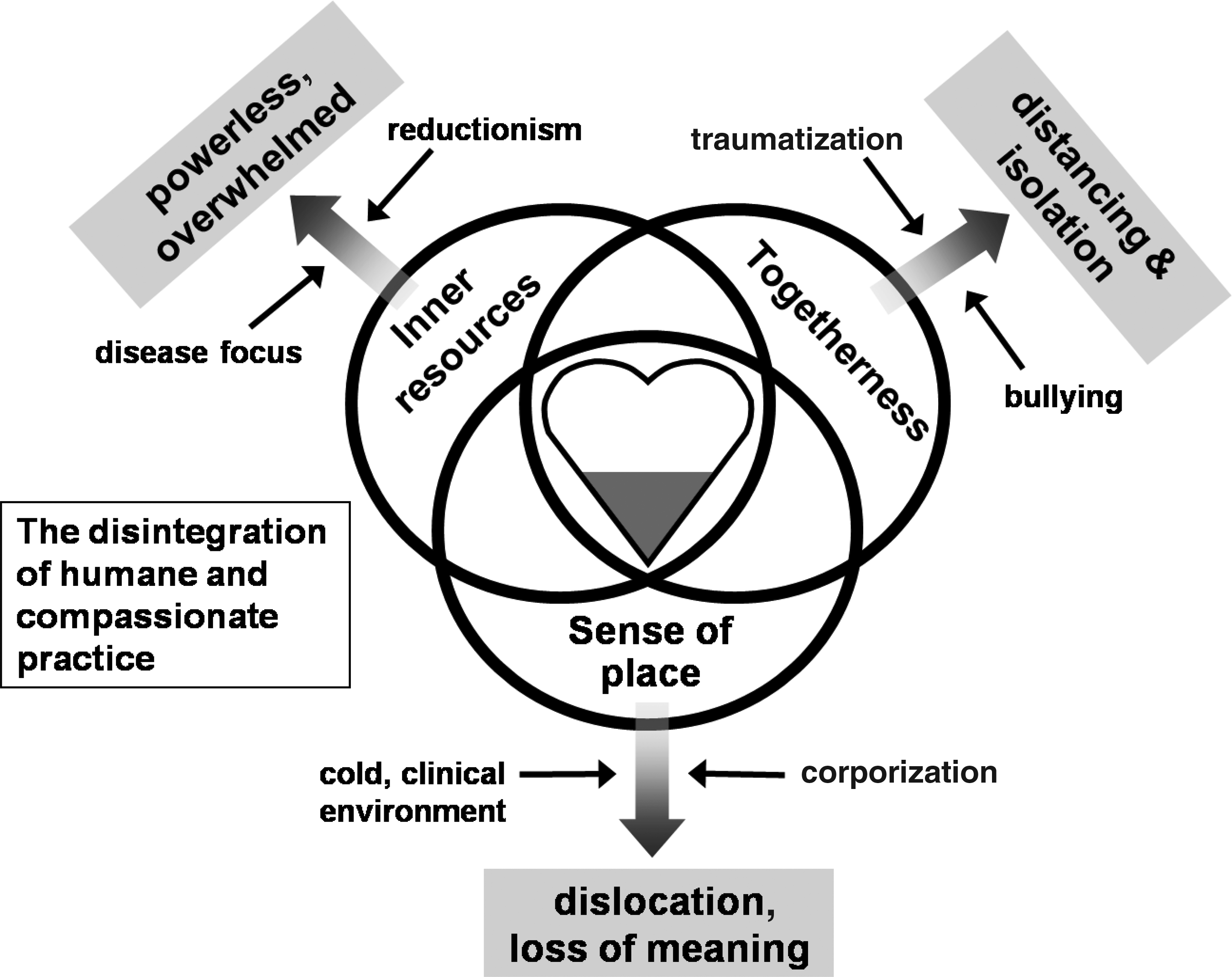
The disintegration of humane and compassionate practice.

The re-integration of humane and compassionate practice.
The presence of a healing environment
The environment within a compassionate hospital must support the healing process for both patients and staff. In this context, we refer to the “hospital” as a physical structure rather than as the collective noun to which we have previously referred. Important issues include easy access to wards, simple signage, comfortable chairs, friendly architecture, and the ability for patients to bring home-comforts into hospital. Evocative wall hangings, mounted throughout the health care institution, should remind staff of the value of their work, the purpose of their roles, and their connectivity to themselves, to patients, and to the wider community. Friendly architecture might involve the use of “healing” colours, and an atmosphere that maximizes natural light, sunshine, fresh air, a sense of space, seclusion and privacy, and large windows with a pleasant aspect. The availability of reflective spaces, or an ecumenical chapel, may allow staff and patients to ponder and re-engage with those issues that give meaning and purpose to daily routines. Seemingly simple acts of caring such as ward cleanliness, the ability to feed patients, and temperature control are obvious. In many of our older health care facilities, it is difficult to imagine how the cramped spaces, poor lighting, paint peeling from walls and ceilings, gray colors, and bare walls would promote psychological and emotional recovery from disease.
A sense of connection among people
It is widely understood that the degree to which people are connected is a good marker of health status. Furthermore, connectivity leads to a sense of meaning and purpose. 27 A compassionate hospital will therefore take steps to foster a sense of connection among its staff and patients.
A connection among staff
Practical examples whereby staff may connect better with each other include communal meals, barbeques, grand rounds events, film evenings, whole person care programs, staff awards, and staff retreats. It has been suggested that Balint groups can be helpful, 28 as can practices such as mindfulness training, poetry, and reflective writing.29,30
A connection between staff and patients
The importance of developing worthwhile and meaningful connections between clinicians and their patients cannot be over-emphasised. It is proposed that many clinicians in modern health care facilities experience feelings of frustration, anger, disillusionment, and guilt because they cannot spend more quality time with their patients, and because their clinical efforts are often thwarted by administrative and resource limitations. Indeed, for many clinicians, meaningful interactions with patients may be a highly effective antidote against the stress associated with working in a regulated bureaucracy. Furthermore, the connection that is developed with patients is a two-way street; Remen suggests that our patients “often have the power to heal the rest of us in powerful ways. Years afterwards, many people can remember what a dying patient has said to them and carry it with them, woven into the fabric of their being, enabling them to be better.” 20
The compassionate hospital will allow clinicians not only to do what they do best as clinicians, but will also recognize the therapeutic value for both doctor and patient of enhancing the quality of the clinician-patient relationship. This can be accomplished by adopting a clinical agenda that includes interactive lecture series and experiential meetings on whole person care, mentoring, reflective writing, clinical supervision, activities such as mindfulness training, the integration of patient support groups into clinical practice, and communication skills programs. In dealing with the suffering of patients, the important role of storytelling and narrative medicine has been highlighted as a way in which clinicians may tap into their patients' experience of illness. Cole and Carlin 17 have also suggested that enabling physicians to tell their own stories and to reflect upon their clinical and personal experiences in an atmosphere of mutual support could be a powerful activity that allows renewal, self-care, and well-being.
A connection between hospital staff and members of the community
Community engagement is another important aspect of connectivity within the compassionate hospital. Community members need to be reassured that their health concerns are not only heard by their local healthcare facilities, but are proactively acknowledged. Staff within a compassionate hospital will therefore be outward-looking, and will treat with respect and technical skill the members of the community whom they serve. Examples by which this connection may be strengthened include a heightened role for hospital volunteers, optimal integration of clergy into the clinical team, fundraising activities, visits and talks by clinical staff to service clubs and at charity events, and hospital-based educational events for the public. For specific projects or programs, it may be advantageous to address health problems using committees composed of both hospital staff and community representatives.
A sense of purpose and vision
To restore the well-documented erosion of worth, meaning, and purpose for staff in today's health care facilities, 14 it is suggested that clinicians need to come together, and to form their own agenda of workplace interests and activities that will feed and sustain them. The development of a sense of purpose and vision calls for clinical leadership to champion this agenda. Fulfilled clinicians who take pride in their work and know what they stand for can more effectively assist administrators in dealing with the bureaucratic aspects of daily employment. Edwards et al. 14 emphasise that “doctors should have the opportunity to shape the goals of the organization, participate in resource allocation, and have the resources to do the job expected.”
It is therefore suggested that a fundamental aspect of the compassionate hospital is to embody a clinical leadership that works with hospital administrators to develop a parallel clinical agenda to meet the needs of the clinical workforce.
A compassionate hospital will clearly define its values and standards. It will also infuse its staff with a sense of identity, vision, and purpose, so that staff members have a better-formed view of personhood, and of their therapeutic utility. A compassionate hospital will have a leadership that is able to sustain staff. Clinical leadership among staff members is vital to the creation of the cultural change required for a compassionate hospital. Hospital managers will be closely involved in developing structures and programs that encourage open engagement with clinical staff, the eradication of bullying, and the provision for staff of the means of supporting a sense of worth, meaning, and purpose. Failure to engender a cultural change that provides a sense of purpose and vision for staff will inevitably result in an erosion of idealism and empathy, and a concomitant increase in corporate cynicism. According to Garling, “a new culture needs to take root which sees the patient's needs as the paramount central concern.” 14 The importance of sincere apology and open disclosure in clinical crises cannot be over-emphasised. Given a well-recognized link between the psychological welfare of staff and patient satisfaction, a failure to provide a sense of purpose and vision to health care workers almost certainly has resulted in poorer experiences and outcomes for patients.
A final objective in this context is the identification and conduct of empirical research to develop and validate measures for the three characteristics that we have proposed; further study could explore the most appropriate models of care that best support patients and staff in a health care facility where compassion is being integrated as a core value.
A Need for Pasteurization?
In the
In defining three characteristics of a compassionate hospital, we have outlined how committed health care workers might take the lead to harness and integrate aspects of existing individual compassion to create an organization with compassion as a core value: “Tu souffres, cela suffit” (“You are suffering, that is enough.”).
Footnotes
Acknowledgments
The authors are indebted to Ms. Judy Cush for her secretarial services and to Professor Geraldine Barnes for her sub-editing skills.
Author Disclosure Statement
No competing financial interests exist.