
Abstract
Abstract
Aims:
To map children's palliative care (CPC) around the world and to and survey the learning needs of respondents.
Methods:
The study reports on the responses to an online questionnaire given by people downloading the online version of the ‘Children's Palliative Care in Africa’ textbook.
Results:
346 people responded (251 health professionals) from all continents but mostly from Africa, N America or Europe. Respondents worked in various types of health facilities, but in Africa over half were HIV/AIDS treatment centres. The average number of children per year seen ranged from 136 in Africa to 82 in Europe. The overall mean confidence scores across all CPC subject areas was 3.2/5. Confidence increased significantly with the degree respondents were exposed to caring for dying children in practice. Nurses were marginally the most confident group, but less confident than doctors in pain and symptom-control. N Americans were more confident than others in all subject areas except HIV/AIDS and spirituality, where Africans were more confident. Europeans were more confident than Africans in symptom control subject areas. Africans see the most children, but have the least confidence, and fewest resources.
Discussion:
This is a descriptive uncontrolled study so any apparent differences between respondent sub-groups require further validation. The study provides insight into who is providing CPC across the world, and highlights the multi-disciplinary nature of CPC. It raises questions about how we can best support colleagues in resource-limited settings. It suggests further study is required into the nature of regional demand for CPC, the best places to resource and provide CPC, the nature of professionals' training needs, the most effective ways to train and deliver CPC care, the best ways for professionals to support each other, and effective ways to share resources and knowledge across the world.
Introduction
This descriptive study offers an insight into what might be happening “out there” by reporting on the responses to an online questionnaire given by people downloading the Children's Palliative Care in Africa 1 textbook. A PDF version of the textbook is provided for free downloading at the International Children's Palliative Care Network website (as part of a Diana Princess of Wales Memorial Fund project to develop CPC services across sub-Saharan Africa). 2
The online questionnaire was derived from the International Children's Palliative Care Network (ICPCN) CPC curriculum (available by request to the author) and has been used by the author in previous studies that explore the educational needs of CPC health professionals in the UK, Uganda, Tanzania, and South Africa.3,4
What we do know about CPC is that nearly all child deaths occur in resource-poor countries, almost half of them in Africa, where 1 in 8 children do not reach 5 years old 5 and where HIV/AIDS and cancer are the two commonest incurable childhood diseases. 6 However, we do not know which types of organizations or professionals might be providing CPC, particularly in developing countries; nor do we know what the educational needs of those professionals might be. In the absence of evidence, those responsible for the development of CPC services, curricula, courses, and learning have little to guide them. Adult palliative care learning resources are being developed, but there are significant differences between adult and children's palliative care.7–12 This study is descriptive in nature, and so cannot offer firm comparative data or conclusions. However, it does serve to provide useful and fascinating insights into who is “out there” and what their learning needs might be, and so may serve to generate and direct further research into CPC development, education, and training in the future.
Study aims
The aims of the study are to map CPC services around the world, specifically looking at which types of organizations and professionals may be offering CPC services in different continents, and to survey what the self-rated educational needs of those professionals might be.
Ethical approval
The educational needs questionnaire was considered and approved by the Hospice and Palliative Care Association of South Africa Research Ethics Committee, The National Institute for Medical Research in Tanzania, and the Uganda Council for Science and Technology.
Methods
To map CPC services, all professionals logging onto the ICPCN website in a 3-month period in 2010 to download the textbook Children's Palliative Care in Africa had to complete an online survey before they could download the book. There were no exclusion criteria. Respondents were asked to give their professional role, country, organization type, number of years they had worked in CPC, and an estimate of the number of children with palliative care needs they had seen in the last year.
To survey educational needs, respondents were asked to self-rate their confidence in each of the 26 subject areas of the ICPCN CPC course curriculum (see Table 1) using a 5-point scale (from 1=completely lacking confidence to 5=completely confident). See Fig. 1 for an example question.
Sample educational needs question from the survey.
Results
Analysis of the respondent demographics
In the first 3 months 346 people responded to the online questionnaire. We were able to analyse the responses as follows:
Professional background
For the data on professional background, see Table 2.
Continent of origin
Given that the textbook was aimed at Africa, it is perhaps not surprising that the largest group (114) was from Africa. However, substantial numbers were also from Europe (110) and North America (92). There were small numbers from the other continents. (See Fig. 2.)
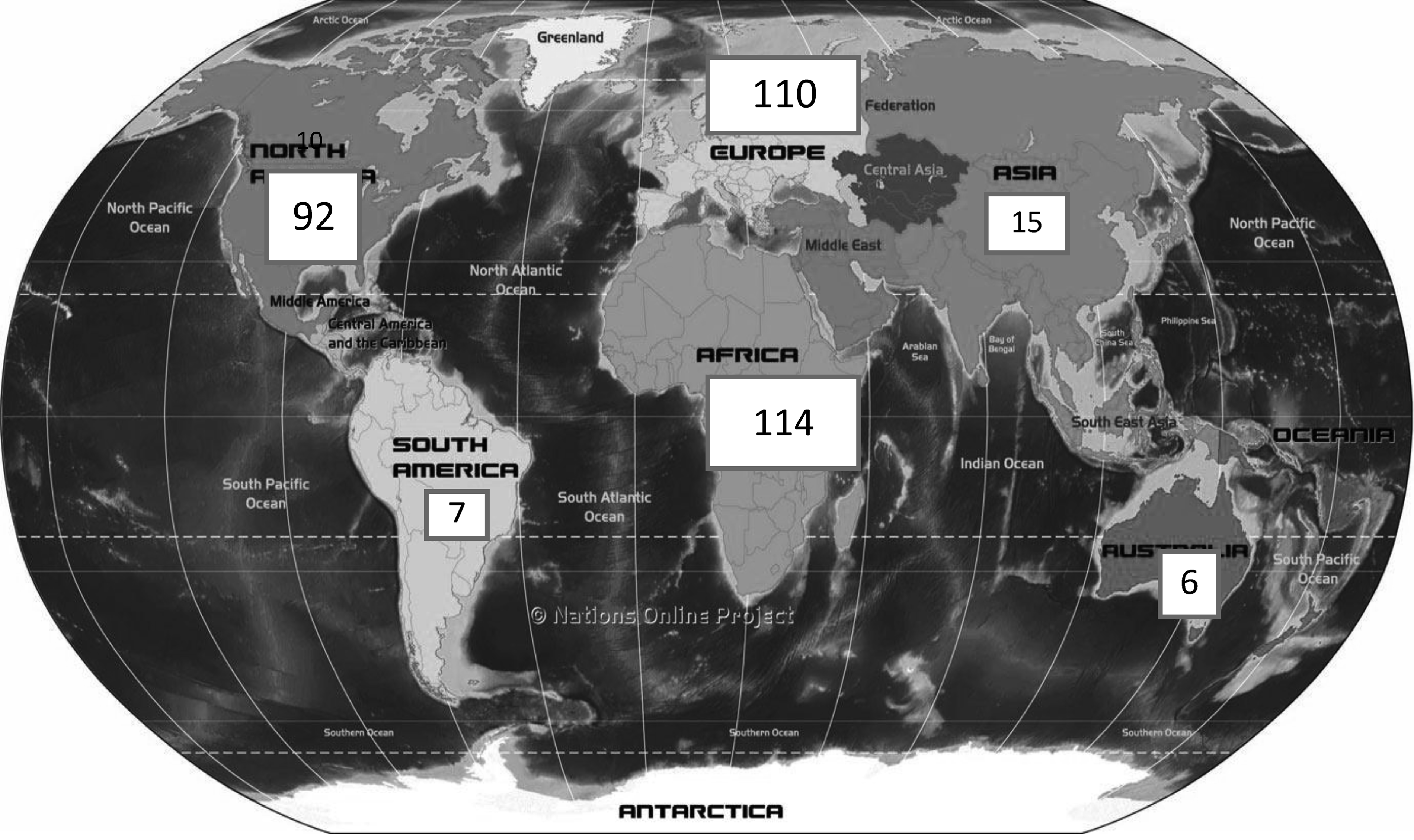
Geographical location of respondents.
Exposure of respondents to children with palliative care needs
To obtain information on respondents' exposure, we asked them to estimate how many such children had seen in the last year (Table 3).
Organizational background
To get an idea of the kind of health facilities professionals work in, we asked respondents to select which medical services their facility offered, from a picking list of HIV/AIDS care, general pediatrics, general medicine, and general palliative care (respondents could tick more than one). (See Table 4.) This information is useful to managers and funders as they try to work out where best to target CPC resources as it tends to be easier to offer CPC where adult palliative care or general pediatric care is already being offered.
Analysis of educational need
Respondents were asked to self-rate their confidence in each of the core domains of the ICPCN CPC curriculum (see Table 1).
The mean confidence score for all curriculum areas combined was 3.2 out of 5 (95% confidence interval [CI] 3.08-3.32). The full list of mean confidence scores per subject area (with 95% CIs) is shown in in Table 5.
Analysis suggests respondents' confidence varies according to the number of children with CPC needs they had seen in the previous year (see Table 6).
Analysis also suggests respondents' confidence varies according to their professional background (with doctors and nurses being more confident than other groups (see Table 7).
AHP, allied health professionals.
The study is descriptive by design, so we have to take care when making comparative analyses as we have not controlled for confounding variables, but we have sufficient data to make some statistically significant comparisons, which may prompt further research:
• Nurses were more confident than doctors in the following subject areas: family (assessment, dynamics, and support), caring at the end of life, holistic assessment and management planning, play and development, managing psychological problems, death and bereavement, community (assessment and intervention), and spirituality. • Doctors were more confident than nurses and other professionals in the management of pain symptom control areas and end-of-life care.
These comparisons are visually represented in Fig. 3. This diagram represents the five subject areas of most and least confidence for doctors, nurses, allied health professionals, and students. The scores are relative to doctors. It highlights that doctors seem more confident than other groups in the clinical subject areas (pain and symptom control areas—to the right of the x-axis) but less confident in some of the nonclinical areas (such as spirituality, community, communication, and psychological problems—to the left of the x-axis).
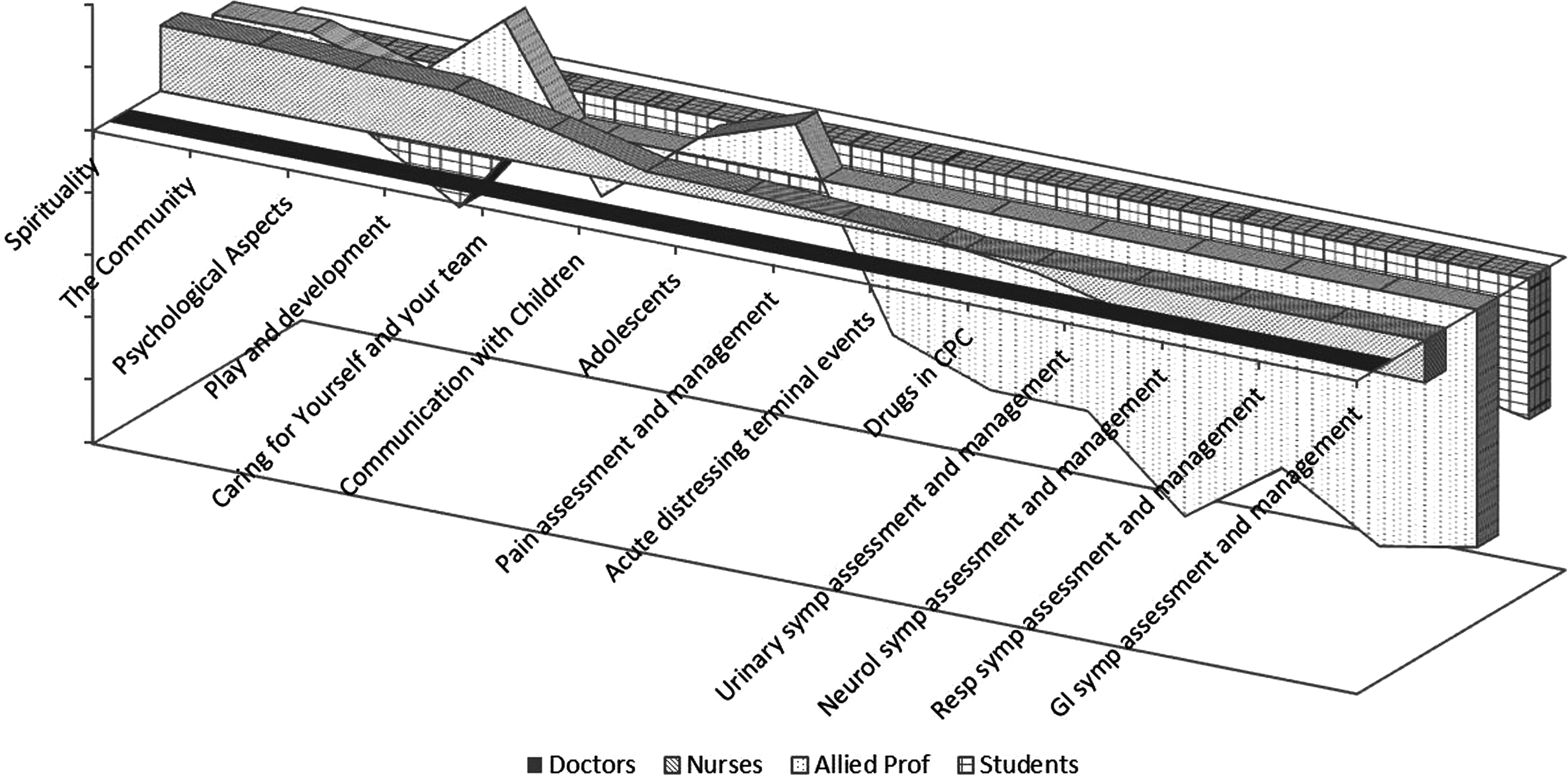
Overall confidence compared with doctors, by professional group.
The sample sizes for Africa, Europe, and North America were large enough to make some statistically significant comparisons, which might be helpful to guide future research:
• European professionals were more confident than African professionals in all of the symptom control areas, pain assessment and management, and end-of-life care. • African professionals were significantly more confident than European professionals in HIV/AIDS care and spirituality. • North American professionals were not less confident than Europeans in any areas, and were significantly more confident than Europeans in HIV/AIDS; adolescents; holistic assessment and management planning; psychological problems; family assessment and management; learning, teaching, and training; communication with children; drugs in CPC; play and development; and background and basic principles in CPC. • North American professionals were more confident than African professionals in all areas except HIV/AIDS, and the difference reached statistical significance in most areas. • African professionals were significantly more confident than European and North American professionals in CPC in children with HIV/AIDS.
These comparisons are visually represented in Fig. 4, in which we have graphically represented the subject areas of greatest and least confidence from African, European, and North American respondents (relative to European respondents).
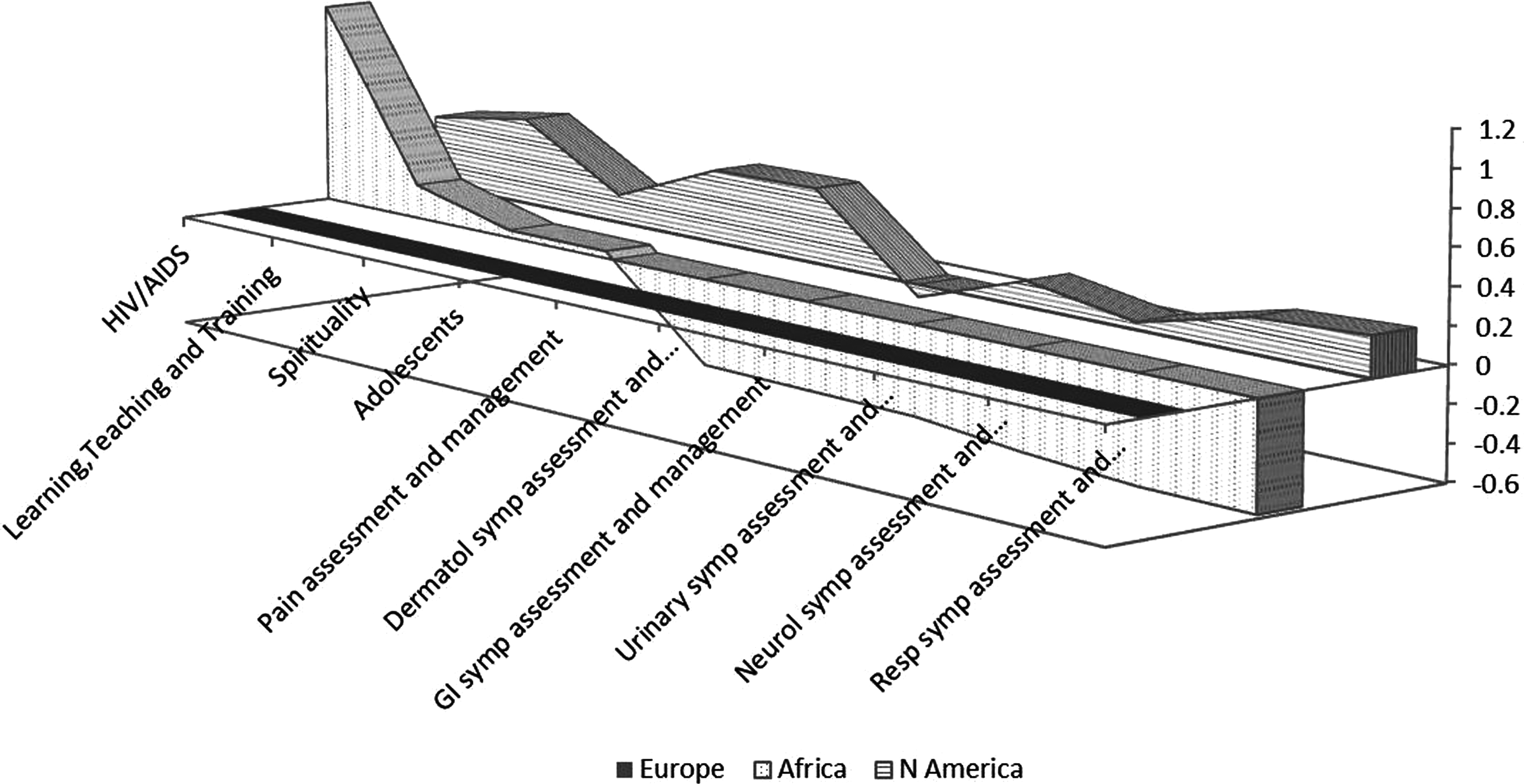
Confidence in subject areas by continent, compared with Europe.
Comments from respondents
Respondents were offered space to make general comments, and a selection of comments is included below:
From Africa many of the comments relate to the size and challenge of the task, given the huge numbers and low resources. For example:
• We are keen to start somewhere. The task is intimidating. • I come into regular contact with children and I am not confident in treating them. • We are just starting a new palliative care centre targeting 200 children per year.
Similar themes emerge from comments from Asia, which also highlight that CPC is still very new and relatively unsupported:
• HIV/AIDS is becoming a serious problem in Indonesia, and we are not really prepared or even seemingly aware. • We have just launched our service in 2008, and we are struggling…our level of confidence is still low, especially because there are no palliative care experts in Indonesia. • We rely on foreign PC expert training 3 times a year. In between, our team has to rely on their own instincts.
From North America we had few comments, but one from a parent:
• I'm a mom of 2 healthy boys. I am not in the healthcare field as a professional merely as a human.
And also one from Mexico:
• Mexico has similar problems that are in Africa. I think it will be very helpful to have the book,
so we can look and find the right answer, for our new PPC.
From Europe we had few comments, except this one from a student nurse, which perhaps captures what many professionals feel about CPC:
• I HOPE I'LL NEVER USE THIS BOOK !!!!
Discussion
This is a descriptive study, aimed simply at describing what is “out there” with the hope that it will generate further questions and research about CPC provision and training across the world. It is important to note that it is not designed as a comparative study. This study is of self-selected respondents who were looking for a free, English online textbook aimed professionals working in CPC in the African setting. We cannot say how representative this population is of the whole population of professionals working in CPC worldwide, but it is unlikely to be fully representative due to differences in native language, awareness of the book or website, and Internet and computer accessibility. Although we have sufficient data to make some statistically significant comparisons in some areas, further research is needed to validate any apparent associations.
Child mortality is a major health problem across the world, and particularly so in developing countries, where resources and health professionals are scarce. It is heartening to see that governmental and nongovernmental development specialists and academics as well as health professionals have accessed and downloaded the textbook and completed the survey.
It was interesting to note that, although the textbook was aimed at African health professionals, there were respondents from all continents, with a substantial number from both Europe and North America. It was also interesting to note that 23% of respondents were not health professionals (or student health professionals) but either academics or professionals working in governmental or nongovernmental development organizations. This may suggest a global interest in African CPC, but also may be because the textbook is a free online resource with contents relevant to any setting.
African professionals see the most children with CPC needs, which again is not surprising given that over half of all child deaths occur in Africa. 13 However, African professionals also appear generally less confident than professionals in Europe and North America, despite the high numbers of children they see. Given that the ratio of health professionals to the population ranges from 10 to 100 times fewer than in industrialized countries, 14 this suggests a particular problem. It appears that the least confident professionals may be working with the most children in the most deprived areas. Further research into the need for, and importance of, CPC training for African health professionals is needed.
In Africa, over half the respondents are based in HIV/AIDS treatment centers, whereas in other continents the proportion is much smaller. Again, this is perhaps unsurprising given the prevalence of HIV/AIDS in Africa, but there may be other associations. For example, perhaps providers in HIV/AIDS centers are more aware of CPC as a need than are professionals working in general clinics or hospitals, or perhaps they are more aware of the learning resources available. Further research exploring the awareness of CPC among different professional groups in Africa and elsewhere may be worthwhile if we are to target CPC advocacy and sensitization work most effectively. The finding may also suggest that funders, policy makers, and trainers might target and draw on the facilities at HIV/AIDS treatment centers to improve CPC capacity and training in Africa.
It was interesting to note that African professionals are significantly more confident than others in HIV/AIDS, which may be related to their greater exposure to children with it. Perhaps further work is needed to explore how the rest of the world can learn from and make best use of this expertise in Africa.
Health professionals' confidence varies from subject area to subject area, and no one professional group is more confident than others in all areas. The study shows that different professional groups appear to offer complementary skills in CPC provision, thus emphasising the potential benefits of a multi-disciplinary approach to CPC provision and training. It also suggests that multi-disciplinary training may be important to enable cross fertilization of ideas and practice among professionals, and also should be flexible enough to allow different professional groups to focus on different areas within the training.
On the other hand, some general trends emerge, which may justify further study. Nurses seem less confident in clinical subject areas (such as pain and symptom control), whereas doctors seem less confident in interpersonal competencies (such as communication, the family, the community, and psychosocial problems) and intrapersonal competencies (such as caring for oneself). This correlates with the author's studies in the UK 3 and Uganda. 4
We have to take care about drawing conclusions from this descriptive study. Furthermore, althoughour self-rated confidence often correlates with our actual learning need, it only does so in subject areas where we are aware of what we don't know. We are by definition blind to unknown areas of incompetence and so can have a high confidence in an area where we have low competence. To investigate this area further, qualitative analysis of professionals' learning needs, as discovered in practice, would be required.
Overall, the findings of this study appear to have implications for course and curriculum design and delivery that justify further study. The findings suggest a multi-disciplinary approach to service delivery and training may be effective, but they also suggest training may need to be flexible enough to cater for the differing learning needs of different professional groups. In resource-poor areas where doctors are scarce, and where nurses often are the lead clinicians, the apparent lack of confidence of nurses in symptom control suggests this is an area on which trainers could focus.
The author hopes that this research will facilitate and encourage others to start addressing the questions that this study has begun to ask, for example:
• What is the demand for CPC and where? • How can we target global resources to meet CPC needs most effectively? • Where are the best places to provide and facilitate CPC services and CPC training? • What CPC training resources are available in different areas? • Are the training resources that are available meeting the actual learning needs of professionals “on the ground”? • How can multi-disciplinary training courses and curricula meet the different needs of different professional groups? • What is the best way of providing CPC in areas where doctors are scarce or inaccessible? • How can training help multi-disciplinary teams work most effectively together to provide CPC, particularly in places where doctors are not easily accessible? • How can professionals in different areas of the world share and pool resources, experience, and understanding to facilitate the advance of CPC worldwide?