
Abstract
Abstract
Background:
Despite broad support for palliative and end-of-life care training in medical schools, required clinical palliative care and end-of-life experiences are rare. In this study, we assess the impact of a required palliative care educational intervention on medical students' palliative care pain knowledge and end-of-life attitudes.
Methods:
In this wait-list control crossover design, third-year medical students from two sequential classes (n=157) completed a palliative care workshop at the beginning of a required year-long course. Students then completed a patient experience, online pain management module, and reflective essay in either the first or second half of the course. Fifteen validated multiple choice palliative care pain management items and the Thanatophobia Scale (7 items) were administered to measure knowledge and attitudes for all students at baseline, 5.5 months, and 11 months. Multivariate repeated measures ANOVA was used to determine differences between groups and across time.
Results:
Analysis found statistically significant increases in knowledge and improvements in attitudes (p<0.001) across the time points as well as a statistically significant interaction effect between time and groups (p=0.006). These changes correspond to specific curricular intervention components in which attitudinal improvements are seen after the workshop, and knowledge increases are seen after the patient experience, online pain module, and reflective essay.
Conclusion:
A modest, required palliative care curriculum can yield improvements in medical student knowledge and attitudes. However, expansion of the experiential component and palliative care skills training and assessment are needed for students to have more meaningful outcomes and to ultimately contribute to better patient outcomes.
Introduction
To improve the palliative and end-of-life care training at Baylor College of Medicine (BCM), we introduced a targeted palliative care curriculum for third-year medical students (MS3s) during a longitudinal required course. Literature suggests that structured didactics and experiential components in a palliative care curriculum lead to higher student self-efficacy for care of dying patients; 8 further, many authors have specifically advocated for more experiential training.9–11 With funding from the End of Life/Palliative Education Resource Center (EPERC), 12 we implemented a palliative care clinical experience augmented by other learning activities and measured students' knowledge and attitudes before, mid-course and after the course in a crossover design. We hypothesized that MS3s would have an increase in knowledge and improved attitudes toward palliative and end-of-life care. The purpose of this article is to report the impact of these educational interventions on MS3s' palliative care pain management knowledge and end-of-life attitudes.
Methods
We implemented our MS3 palliative care curriculum in a required 46 week clinical and community course, Longitudinal Ambulatory Care Experience (LACE). This course occurs one afternoon per week after students have completed 18 months of preclinical and 6 months of clinical training. Here we report methods and data collected during 2007–2008 and 2008–2009; the first 2 years of the curriculum.
At the beginning of LACE (July), we conducted a 3 hour required palliative care workshop. The workshop had two large group components with all students together: a 1 hour didactic lecture on basic palliative care concepts (definitions, domains, scope) immediately followed by a 45 minute faculty interview with one or two bereaved family members of patients who had received palliative care. Students were then randomly assigned to small groups of 8–10 for a 1 hour discussion facilitated by two interdisciplinary faculty with palliative or end-of-life care experience, including one physician. Small groups further processed palliative care concepts, including personal experiences and relevant cases, serious illness trajectories, and health care provider responses to strong emotions evoked within this area.
Over the following 11 months, students completed a 3 hour palliative care patient experience. Students visited one of eight clinical sites (six community hospice sites and two inpatient palliative care settings in tertiary hospitals) and were supervised by a committed cohort of eight board-certified hospice and palliative medicine physicians who had received curricular training for the project and ongoing support. These physicians led all student activities at their site and were also trained to identify clinical teaching points and explore student thoughts and feelings about the patient interaction and lessons learned. One to three student pairs visited a site together depending upon patient volume at each site. After the site orientation, students participated in a brief review of palliative care domains, scope, and goals. Student pairs were introduced to preselected, consenting palliative care patients or if a patient was nonverbal, family members. Students spent ∼1–1.5 hours interviewing the patient or family using a standardized palliative care history and physical form, with intermittent direct physician supervision. Finally, student pairs presented their patients to the lead physician and fellow students for discussion, teaching points, and debriefing with lessons learned.
Students were also required to complete an online palliative care pain management module developed by the Medical College of Wisconsin (MCW) 12 and encouraged to do so prior to their palliative care patient experience. This interactive module highlighted the role of nonopioid analgesic agents, key pharmacological principles of opioid analgesics, and indications for specific adjuvant medications for neuropathic pain, and included a set multiple choice test questions. Although students had access through the EPERC grant to 16 online palliative care training modules developed at MCW, they were only required to complete the pain management module. Completion of the pain management module was monitored online to ensure that all students completed this part of the intervention.
To enhance the educational intervention and reinforce learning, students were required to complete a reflective essay within 1 week after their palliative care patient experience. Students were asked to reflect on their thoughts and feelings about caring for a dying patient before versus after the visit, the challenges they encountered, and the application of the experience to future patient encounters. The lead physician reviewed the essay and provided the student written feedback. In summary, the entire intervention (palliative care workshop, palliative care patient experience, online pain management module, reflective essay) comprised ∼8 hours.
To assess the efficacy of this multiple component intervention, we assessed changes in knowledge and attitudes using one tool for each from previously validated instruments. Validated tools in this area were few and ease of repeat administration to a large group was important. Palliative care pain knowledge, specifically in the area of opioid analgesia, was measured via 15 multiple choice items. Seven items were selected from the MCW online pain management module test questions, 12 and eight were selected from a validated instrument used in the National Residency End-of-Life Education Project. 13 The items were selected to test basic opioid knowledge, as this is a challenging but important area in palliative care. Both sets of source questions were developed by experts in the field. A summed total score for each student at each administration was calculated by determining the total number answered correctly out of 15. Palliative care attitudes were measured using the Thanatophobia Scale, 14 , a seven item Likert scale (1=strongly agree, 7=strongly disagree; scale direction reversed so higher scores reflected more positive attitudes) that quantifies affective responses to care of dying patients and their families. The scale was selected because it had been validated with medical students and used to measure the impact of palliative care education. 14 A mean score for the seven items was calculated for each student at each administration. Students were also asked to indicate the number of core clerkships completed and the number of past encounters with imminently dying patients since entering medical school. Student demographic data were captured for race and gender. Students were asked to complete these instruments as a paper and pencil questionnaire prior to the start of the palliative care workshop in July (baseline), at mid-course in January (T2), and at course conclusion in June (T3) (see Fig. 1).
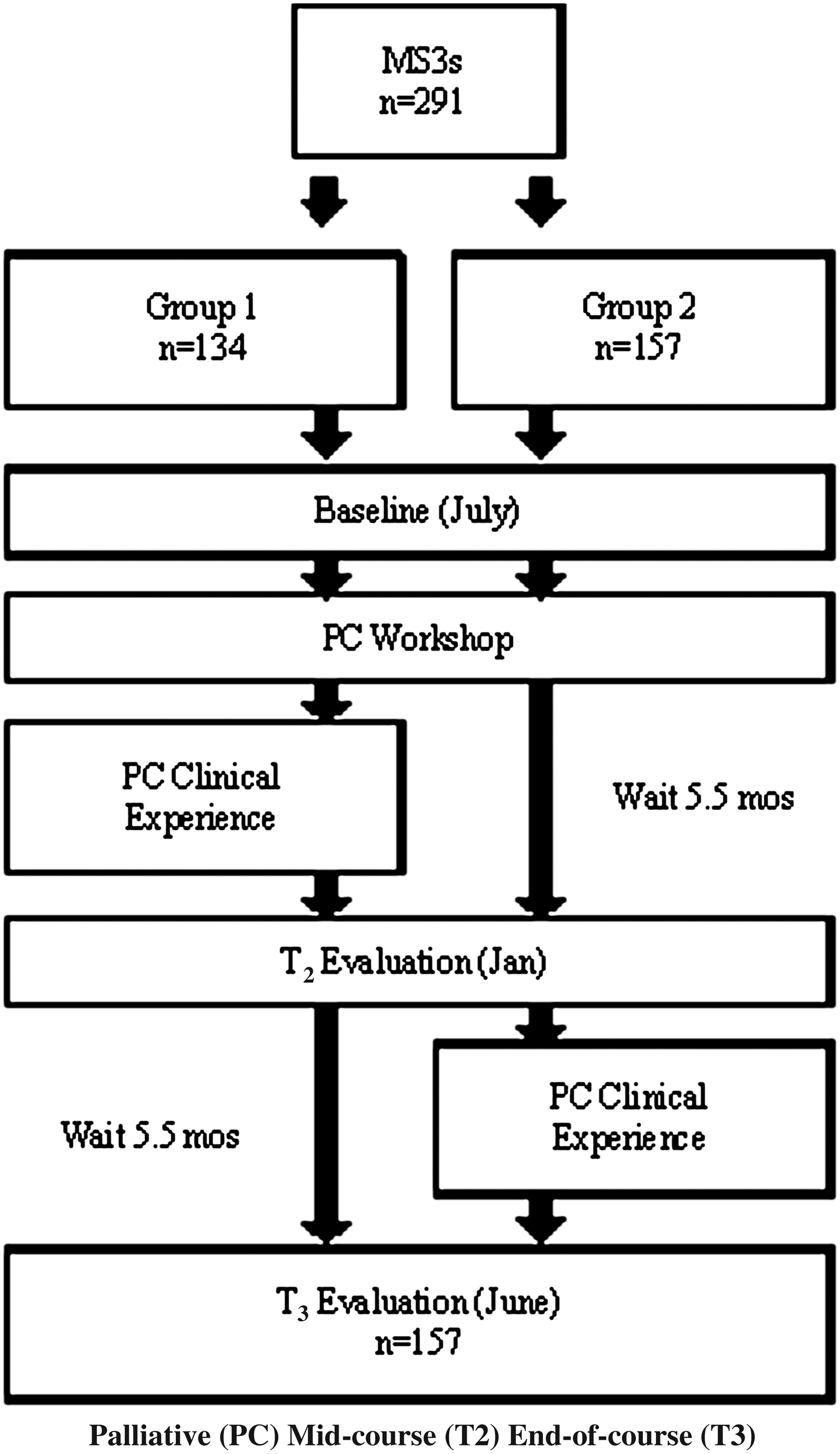
Graphic depiction of the wait-list control group with crossover design.
To determine the outcomes of this intervention, we utilized a wait-list control group with crossover design (see Fig. 1). 15 At T2, approximately half of the students had completed the palliative care workshop and palliative care patient experience, including the online pain management module and reflective essay (Group 1), whereas the other half had completed only the palliative care workshop (Group 2). At T2, Group 2 “crossed-over” and participated in the palliative care patient experience, with online module and essay completion, allowing us to compare the effects of the palliative care workshop and palliative care patient experience and the durability of those effects.
Descriptive and inferential statistics were calculated using SPSS 18.0. Data for two student cohorts (2007–2008 and 2008–2009) were combined. Descriptive statistics included percentage, median (Me), mean (M), and standard deviation (SD). To determine differences between Group 1 and Group 2 and across the three time points (baseline, T2, T3), multivariate repeated measures ANOVA was conducted with post-hoc analysis using Bonferroni correction. We set our α at 0.05. Educational significance, or effect size, was determined using η2 and Cohen's d. As there were few identified studies on which to base our decisions, we used recommendations of η2=0.01 and d=0.20 as a small effect, η2=0.06 and d=0.50 as a medium effect size, and η2=0.16 and d=0.80 as a large effect. 16 BCM Institutional Review Board approval was obtained for this study.
Results
In total, 157 students completed questionnaires at the three time points, for a response rate of 54.0%. Almost half the students were female and approximately one-third were from an underrepresented minority group, which is representative of the overall BCM student body. At baseline, most students had completed three clerkships (M=3.19, Me=3, SD=0.72) and interacted with two dying patients (M=2.53, Me=2, SD=2.42). However, 17.5% of students reported no encounters with an imminently dying patient. At baseline, students correctly answered 33.5% of the knowledge items and had a mean score of 4.81 (SD=1.18) out of 7 on the attitude items.
Comparing Groups 1 and 2, no differences were found at baseline for gender, race/ethnicity, or number of clerkships completed (Table 1). However, students in Group 2 had interacted with more dying patients (p=0.046, see Table 1 for results). No differences for palliative care pain knowledge or attitudes were noted between the groups at baseline.
M, mean; SD, standard deviation; NS, non-significant.
Multivariate ANOVA analysis indicated overall statistically significant differences between the two groups (p=0.463, η2=0.01) and across the three time points (p<0.001, η2=0.13), and an interaction effect between time and group (p=0.006, η2=0.024) for both attitudes and knowledge. We noted significant improvements in attitudes across time (p<0.001, η2=0.28) but not between groups. Both Groups 1 and 2 showed statistically significant increases in attitudes between baseline and T2 (p<0.001, d=0.42) with no change between T2 and T3 (p=0.922, d=0.01). Analysis of knowledge indicated an overall significant increase in knowledge scores (p<0.01, η2=0.24) and an interaction effect of time and group (p=0.001, η2=0.09). Knowledge scores for Group 1 significantly increased between baseline and T2 (p<0.001, d=0.87), with no change between T2 and T3 (p=0.827, d=0.03). The knowledge scores for Group 2 showed no change between baseline and T2 (p=0.268, d=0.16) but a statistically significant increase between T2 and T3 (p<0.001, d=0.79). Table 2 provides specific results for each group at each time point.
M, mean; SD, standard deviation.
Attitudinal instrument scale 0-7.
Knowledge instrument scale 0-15.
Group 1 participated in both the palliative care workshop (immediately after baseline) and palliative care patient experience (between T1 and T2); Group 2 participated in palliative care workshop (immediately after baseline) and palliative care patient experience (between T2 and T3).
Discussion
Our findings suggest that an intensive, targeted but relatively brief MS3 palliative care curriculum with didactics, small group content, online palliative care pain management module, clinical patient experience, and reflective essay can increase palliative care pain knowledge and improve palliative care attitudes. Other medical student palliative care curricular initiatives have suggested positive knowledge 17 and attitudinal18,19 outcomes. Whereas some have included pre- and post-test data showing favorable changes in knowledge and attitudes, 20 none have reported a similar crossover design.
Despite completing 6 months of clinical rotations, MS3s displayed only mid-range attitudinal scores and very limited palliative care pain management knowledge at baseline, indicating a low level of proficiency. These concerning levels are not surprising with the inadequate training opportunities reported by many medical students.3,4 Dy et al. 21 also found deficient opioid-specific knowledge at pretesting in residents completing a different online palliative care pain module; for two opioid questions identified, 31% and 41% of residents answered correctly. Given that our MS3 scores were similarly low, this suggests that palliative care pain management curricula, specifically for opioid analgesia, should be strengthened across medical school and residency training.
Our results indicate that students' palliative care knowledge and attitudes improved from baseline levels and that these gains remained stable over time. Analysis suggests that the knowledge increase corresponded to the palliative care patient experience, before which students were encouraged to complete the online pain management module. Thus, the palliative care patient experience, perhaps specifically the online module, increased palliative care pain management knowledge, although students still answered less than half of the items correctly and the actual mean score increase was only approximately one point. The same study of residents also reported a statistically significant increase in palliative care pain knowledge after completion of that online module; however, the opioid-specific knowledge gains were generally lower than other gains. 21 Despite our statistically significant knowledge score increase, the persistently low scores on completion are troubling. Evidence suggests that acquisition of pain management knowledge is challenging even for fellows and practicing physicians. In one study, only 23% of second year hematology/oncology fellows responding to a palliative care survey correctly performed an opioid conversion. 22 Wolfert et al. found that a random sample of licensed physicians in Wisconsin had poor understanding of addiction, appropriate opioid prescribing, and practice guidelines for pain management. 23 Our findings suggest that a more intensive and experiential curriculum is needed to address these deficiencies and learning challenges at the student level.
Positive attitudinal changes occurred after the palliative care workshop for both groups and, importantly, persisted over time. This suggests that a workshop with palliative care didactics, interviews with bereaved family members, and a small group activity can have a lasting impact on students' palliative care attitudes. Perhaps this type of highly emotional activity 24 is sufficient to change attitudes and influence student perceptions. Although our results show statistically significant increases and effect sizes between small and medium, it seems that an expanded intervention could also more strongly impact attitudes.
Compared with many medical school palliative care initiatives, our intervention of ∼8 hours per student was modest. Other reported curricula unfold over days19,20 or weeks. 18 One study designated a 12 hour minimum for “formal” palliative care training and found that more hours corresponded to higher palliative care self-efficacy scores. 11 Nonetheless, although we advocate for more dedicated time, our results suggest that a targeted, but less time-consuming intervention can still yield statistically significant outcomes, especially attitudinal ones. Additional data are also supportive of the positive impact; BCM student ratings of “inadequate” instruction for palliative care/pain management and end-of life care on the AAMC Graduation Questionnaire decreased from an average of 30% and 31%, respectively, for the two classes prior to implementation to an average of only 16% and 13% for both cohorts of students who participated. Moreover, qualitative data from student essays suggest that students valued the palliative care patient experience.
We posit that not only content, but also methods are critically important with regard to time intensity. Our inclusion of a supervised clinical experience, knowledge transfer, and a reflection exercise (three of five elements of an idealized palliative care curriculum) 10 employed significant resources but created a robust enough intervention to improve attitudes and increase knowledge. At the same time, we acknowledge that much potential learning is left unmeasured. Our instruments were selected for established validity, ease of measurement, and track record of use. Future efforts should broaden knowledge assessment beyond opioid-specific domains and further examine attitudinal outcomes.
Limitations
Our study has a number of limitations. First, even though all students were required to complete each experience, only 54% completed the assessments at all three time points. This response rate reflects the fluidity of a class cohort (away rotations, dual degree programs, study abroad) during the clinical years. Because the assessment was proctored, only students in attendance on all three dates had matched responses. Interestingly, our analysis of students who completed the questionnaires at all three points was similar to those who did not. We noted no differences in race, sex, number of clerkships completed, or number of patients observed during their last days of life. Students who completed the questionnaires at all three points did, however, have slightly higher pain management knowledge scores, by approximately half a point, and slightly lower palliative care attitudes at baseline. In total, this suggests that our results are reflective of the class as a whole, despite our low matched triplicate response rate. Second, although our palliative care pain management knowledge items were taken from existing instruments, they were not independently validated. This tool was also specific to opioid knowledge domains and, therefore, a very specific, narrow measure of palliative care pain knowledge. Third, it is difficult to isolate the impact of a longitudinal palliative care curriculum in the context of routine MS3 clinical rotations. Our results may reflect other palliative care training students received during these rotations. The crossover analysis, however, demonstrates specific improvements at defined time points for both palliative care pain knowledge and attitudes that correspond to our intervention. Finally, this curricular intervention was limited to knowledge and attitudes and did not incorporate palliative care skills training or assessment. Knowledge and attitudes are key focal points for improvement but are not sufficient to prepare future physicians to provide high quality end-of-life and palliative care and to improve patient outcomes.
Because a longitudinal, required MS3 course that parallels clinical rotations is uncommon in medical schools, the generalizability and reproducibility of our results may be limited. For BCM, the ability to integrate palliative care curricular elements longitudinally within the same highly-regarded course offered a unique opportunity. Nonetheless, implementation of the separate components (i.e., palliative care workshop and clinical palliative care experience) is possible within a clerkship or across multiple clerkships. The literature reports implementation of similar curricular elements within 16 and across clerkships. 17
Conclusion
Statistically significant and sustained improvements in palliative care pain management knowledge and end-of-life attitudes occurred with a modest, required MS3 palliative care curriculum. Despite this, it is difficult to predict whether these changes will translate into improved patient outcomes. For this reason, expansion of our curriculum to include greater breadth and depth of palliative care knowledge domains and assessment, more experiential training, and a specific focus on skill building and skill assessment is needed.
Footnotes
Acknowledgments
The authors acknowledge Dr. George Taffet for his mentoring in developing the intervention, Dr. Susan Block for her mentoring in the EPERC grant implementation, and Dr. David Weismann for the use of his materials. Dr. Morrison's work was supported by funds from Geriatric Academic Career Awards K01 HP 00077 and K01 HP00117. The authors received funding from the Medical College of Wisconsin/EPERC, which was funded by the Robert Wood Johnson Foundation Increasing Palliative Care in Medical Education Grant.
Author Disclosure Statement
No competing financial interests exist.