
Abstract
Abstract
Background:
Children with life-threatening illnesses have unique physical and psychosocial needs that pediatric palliative care programs can address. Integrated programs strive to address these needs from the point of diagnosis through death, if needed, at the same time that curative care is provided. To better understand the variation in these needs, we assessed the health status and health-related quality of life (HRQOL) of children enrolled in an integrated pediatric palliative care program.
Methods:
A telephone survey was conducted with 98 parents whose children were enrolled in an integrated pediatric palliative care program in Florida. The Health Utilities Index (HUI) system was used to assess health status and HRQOL.
Results:
HUI2 attribute levels show that children have the greatest impairment with moderate-to-severe burdens related to self-care, mobility, and sensation, and the least impairment with emotion. HUI3 attribute levels show that children have the greatest impairment with moderate-to-severe burdens related to ambulation and cognition and the least impairment with hearing and emotional functioning. Mean overall HUI2 and HUI3 utility scores are 0.37 and 0.15, respectively.
Conclusion:
Children with life-threatening illnesses in our sample had a high level of morbidity compared with those found in other HUI studies of children with acute or chronic health conditions. Not only do our results highlight severely impaired HRQOL, they also demonstrate the wide variety of health states and needs for children in integrated palliative care programs. This information can help develop strategies to encourage more providers to participate in integrated pediatric palliative care programs.
Introduction
A major obstacle to developing these programs is that there is no clear understanding of whom to enroll and what services to provide. Children with life-threatening illnesses generally are at risk of dying before adulthood. Beyond that generalization, identifying children for enrollment is complicated. Life-threatening illnesses are heterogeneous, often have uncertain prognosis, and may be extremely rare. The IOM and the Association for Children's Palliative Care have described categories and trajectories of illness for these children.10,13 The categories and trajectories are insightful, but they are limited in their ability to conceptualize the scope and frequency of services needed. Without an understanding of health needs, staffing, service provision, management, and fiscal planning can be enigmatic. Lack of this information might lead to resistance by providers to serve children or to start their own programs.
Understanding the services needed requires an understanding of health needs. Solely focusing on the children's diagnoses does not necessarily help, given that functional capacity may vary across stages of disease progression. A first step is to understand the child's health status and health-related quality of life (HRQOL). In pediatrics there are numerous instruments used to measure HRQOL. Among these instruments, preference-based measures provide the ability to estimate quality-adjusted survival, which is relevant for early integrated pediatric palliative care. 14 Children in these programs have a variety of diseases; therefore, disease-specific instruments, although relevant, would not allow for comparisons. Generic instruments measure children's functioning levels across multiple domains of health;15–18 however, a 2009 study demonstrated that the PedsQL™ was not sensitive enough to be used in a population of children with life-threatening illnesses. 19 Preference-based questionnaires link a respondent's health profile to the utility of living in that state. These have been used in children with cancer,20–27 spina bifida, 28 cystic fibrosis, 29 and hydrocephalus. 30
Our study has two aims: 1) to employ a preference-based approach, the Health Utilities Index (HUI) system, to describe the health status of children enrolled in an early integrated pediatric palliative care program and 2) to summarize overall HUI2 and HUI3 scores to describe the distribution of overall HRQOL.
Methods
Sample
Study participants included parents of children, adolescents, and young adults 5–21 years of age who were enrolled in Florida's Partners in Care: Together for Kids (PIC:TFK) program, the first publicly funded, early integrated pediatric palliative care program in the nation. 12 The HUI developers do not recommend that children <5 years of age be administered the tool, as it is not valid for this age group (which represents 29% of those in the program). 31 All those enrolled in the program are eligible for Medicaid or State Children's Health Insurance Program (SCHIP). Children are identified for potential enrollment by their state-employed care coordinator. Care coordinators base their decision to approach a family on their knowledge of the child's circumstances and a list of potential diagnoses that result in a child being eligible for the program. After a referral is obtained from the primary care physician, parents are approached to enroll their children, and services are provided by a local hospice or at the children's homes. 32 Services available to children include support counseling, expressive therapies, pain and symptom management, personal care, and nursing care. Services available to family members include respite, support counseling, and expressive therapies. Children can receive curative and palliative care at the same time.
All parents in the program were sent a letter informing them that a telephone survey, which asked generally about quality of care and program satisfaction, would be conducted. Surveys were conducted in English and Spanish between July and September 2009. HUI items were a subset of that survey. The University of Florida's Institutional Review Board (IRB) approved this study. The IRB approval did not include permission to speak directly to the children/adolescents themselves or matching the survey data with diagnoses in administrative data.
Outcome measure
The HUI was used in this study. The HUI is a survey that the parent completes to assess health status on several different domains of health and calculates an overall health utility score for children ≥5 years of age.31,33–35 The HUI is comprehensive in that it provides information about the type and extent of disabilities (generic scales), and it also provides information about the relative importance of those disabilities (preference-based scales). Hundreds of pediatric studies have used the HUI.20–30, 36–41
The HUI consists of two systems, HUI2 and HUI3, which are independent but complementary systems often reported together.34,35 For each of the HUI2 and HUI3 systems, there are four standard outcome measures. First, once the parent completes the survey, an algorithm is used to convert the responses to a six-attribute vector for the HUI2 and an eight-attribute vector for the HUI3. The HUI2 has six attributes each with four or five levels of functioning: sensation (vision, hearing, speech), mobility, emotion, cognition, self-care, and pain. Fertility is included in HUI2 but was not assessed in this study. HUI3 has eight attributes each with five or six levels of functioning: vision, hearing, speech, ambulation, dexterity, emotion, cognition, and pain. The HUI2 and HUI3 attribute levels can also be collapsed into four standardized disability categories: none, mild, moderate, or severe. Second, standardized scoring algorithms produce a single-attribute utility score for each attribute ranging from zero to one, where zero represents the lowest level of function and one represents the absence of disability in that attribute. Third, the comprehensive health state for each child is calculated based on the combination of that child's attribute levels. The comprehensive health state of each child is described as a health state vector consisting of one level for each of the attributes. Fourth, a standardized scoring algorithm produces an overall multiattribute HRQOL score. The overall HUI2 utility score ranges from −0.03 to 1.00 and overall HUI3 utility score ranges from −0.36 to 1.00. Negative scores connote states considered to be worse than death. Higher overall utility scores indicate better HRQOL. All coding algorithms are included in the HUI Procedures Manual. The HUI scoring functions are based on community preferences. The HUI2 scoring function was estimated using preference scores obtained from a random sample of parents. The HUI3 scoring function was estimated using preference scores obtained from a random sample of the general population ≥16 years of age. The reader is referred to Torrance et al. and Feeny et al. for a further explanation of the HUI system and scoring instructions.34,35 Generic preference-based measures such as HUI combine self-assessed health status (parent as proxy respondent in this study) with the application of community preferences for the valuation of self-assessed health status.
STATA version 10.0 was used to calculate the HUI2 and HUI3 single attribute and overall HRQOL scores. 42 Missing data accounted for between 1% and 13% of question responses and were imputed by making logical imputations wherever possible using the instrument developer's instructions. When calculating the overall utility score, any remaining missing values were imputed using attribute levels randomly selected from the whole population.
Results
Sample characteristics
The response rate for the 98 parents of children ≥5 years of age who completed the HUI was 67.1%. Table 1 describes the characteristics of the children and adolescents in the study and shows that 51% of parents lived in a two-parent household, 42% were married, 84% primarily spoke English, 58% were white non-Hispanic, and 35% had an Associates Degree or higher. Mean age of the children and adolescents was 12.4 years, and 56% were female.
HUI2 results
Table 2 shows the percentage and number of children and adolescents in the sample by attribute level. Higher levels imply greater loss of functionality. Those in the sample were most severely impaired in their ability to perform self-care functions (63% of parents reported moderately or severely impaired health status) and least impaired by emotion (35.8% of parents reported moderately or severely impaired health status) and pain (40% report no problems with pain). Fifty-eight percent of children and adolescents had moderate-to-severe disabilities relating to sensation (vision, hearing, or speech) and mobility. These trends are also illustrated by the single-attribute HUI2 utility scores, where a lower utility score indicates a greater degree of impairment (Table 3).
The Classification Scheme for HUI2 Levels is described in Torrance et al. 34 HUI2 does not include a level 5 for three attributes: sensation, cognition, and self-care.
HUI2 Level 1 corresponds to no disability; Level 2 corresponds to mild disability; Level 3 corresponds to moderate disability; Levels 4 and 5 correspond to severe disability.
Although not shown in the table, there were 88 unique vectors indicating that the sample was heterogeneous. Figure 1 presents the distribution of overall multiattribute utility scores for the HUI2 and HUI3 (median HUI2 multiattribute score=0.32; mean HUI2 multiattribute score=0.37; standard deviation=0.28; median HUI3 multiattribute score=0.05; mean HUI3 multiattribute score=0.15; standard deviation=0.42).
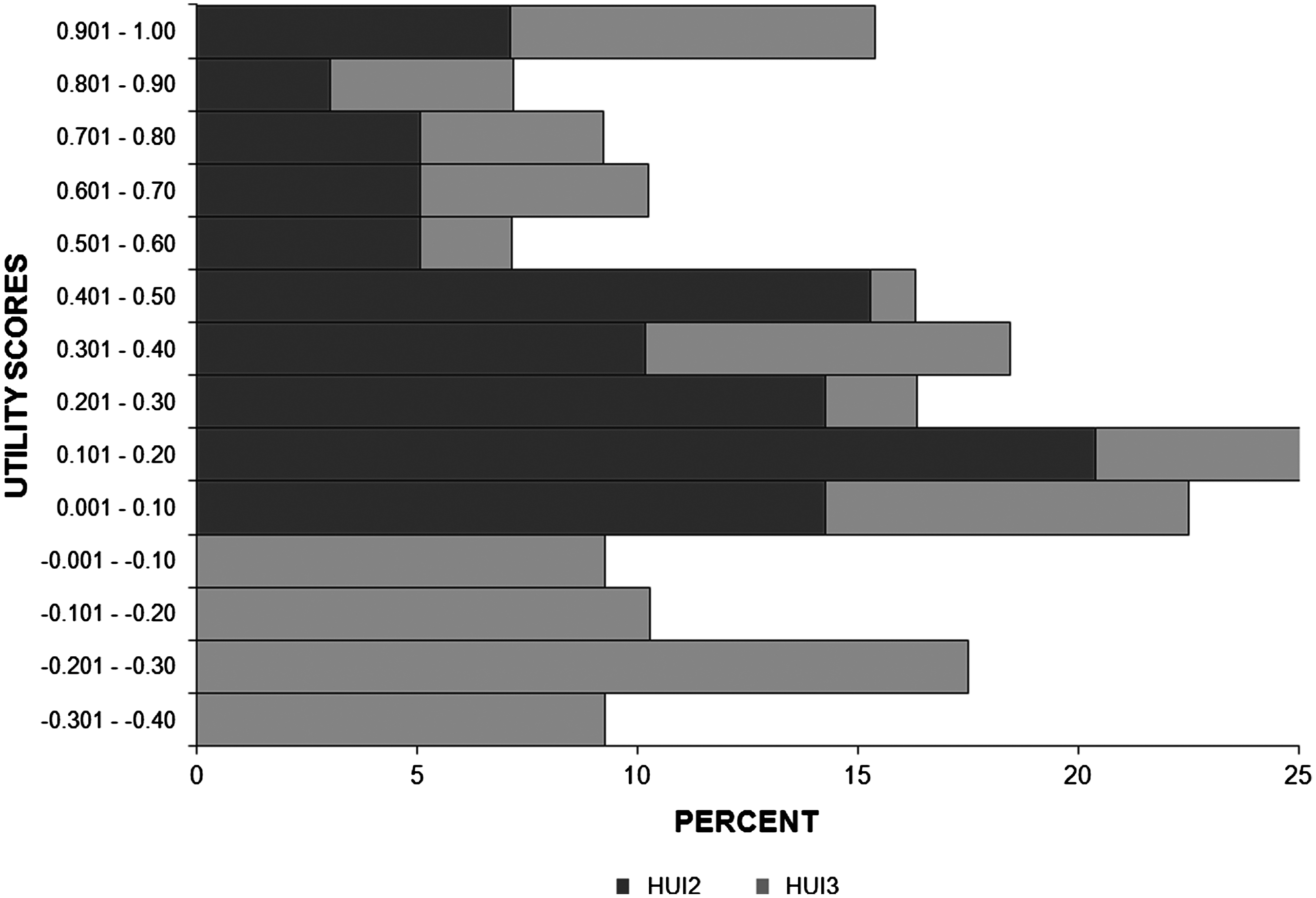
HUI utility scores.
HUI3 results
Table 4 shows the percentage and number of children and adolescents in the sample by level for each of the eight attributes. Those in the sample were most severely impaired in ambulation and cognition (57–58% of parents reported moderately to severely impaired health status) and least impaired by hearing (11% of parents reported moderately to severely impaired health status) and pain (40% reported no problems with pain). These trends are also illustrated by the single attribute HUI3 utility scores, where a lower utility score indicates a greater degree of impairment (Table 5).
The Classification Scheme for HUI3 Levels is described in Feeny et al. 35 HUI3 does not include a Level 6 for three attributes: speech, emotion, and pain.
HUI3 Level 1 corresponds to no disability; Level 2 corresponds to mild disability; Levels 5 and 6 correspond to severe disability.
Level 3 corresponds to moderate disability for all attributes except cognition, where Cognition Level 3 corresponds to a mild disability.
Level 4 corresponds to moderate disability for the sensory attributes (speech, hearing, and speech), but to severe disability for all remaining attributes.
Although not shown in the table, there were 90 unique HUI3 vectors indicating that the sample was heterogeneous.
Discussion
This study investigated the health status and HRQOL within a population of children and adolescents who were enrolled in Florida's integrated pediatric palliative care program. Our results extend the literature in the following ways.
First, we used the HUI system, which provides an alternative to other methods of measuring HRQOL. 19 For example, unlike other generic HRQOL scales that report on general constructs of physical and emotional functioning, the HUI specifically addresses sensation, mobility/ambulation, emotion, cognition, self-care, pain, and dexterity. Results from the HUI2 show that children and adolescents in our sample had the most impairment in self care, mobility, and sensation, and the least impairment in emotion. The most impairment in self-care has implications for family caregivers and corroborates findings from our prior work. 43 In a 2010 study, we found that more than one half of parents whose children were in the program reported fatigue (65%), having to give up things (71%), having to change plans at the last minute (76%), and having difficulties in finding a reliable caregiver (77%), and said that their lives were like a roller coaster ride (90%).
Second, because we used the HUI, we could compare the functioning levels for children and adolescents in our sample with results from other studies. Our sample had a mean HUI2 utility score of 0.37. Examples of HUI2 mean scores from other studies are 0.78–0.96 childhood cancer survivors,20–24 0.86 liver transplant survivors, 44 0.83 adolescents with cystic fibrosis, 29 0.82 extremely low birth weight, 37 and 0.55 spina bifida. 28 Our sample had a mean HUI3 utility score of 0.15. Examples of HUI3 mean scores from other studies are 0.6–0.93 childhood cancer survivors,25–27 0.73 cystic fibrosis, 36 0.59–0.86 extremely low birth weight or preterm,38–41 0.62–0.63 hearing loss or damage,45,46 0.45 spina bifida, 36 0.36 Down's syndrome, 36 0.28 cerebral palsy, 36 0.18 chromosomal abnormalities, 36 and 0.12 hydrocephalus. 36 The children and adolescents in our sample were markedly more impaired. There are several ways these results could be interpreted. Our results could imply that there is selection bias in that only the most impaired are approached for enrollment in our program. Alternatively, our results could imply that our program is appropriately enrolling those with the greatest health care needs. This illustrates the importance for key stakeholders who are considering implementing an early integrated program to set priorities for which children and adolescents they wish to serve in the program. Setting global criteria for enrollment based on diagnoses alone may not align with the needs of the patient and may lead to inefficient allocation of resources, whereas the mean, median, and range of HUI scores might help in this process. It is important to note that whereas there is some overlap between HUI2 and HUI3, there are domains that differ. For example, in regard to pain, HUI2 focuses on the amount or type of pain and analgesic requirements, whereas HUI3 focuses on the extent to which pain disrupts activities.
Third, our results can be used to understand the priorities for service provision in an integrated program, and how those services differ from traditional pediatric palliative care. For example, pain management is viewed as a core component in traditional, or end- of-life, pediatric palliative care, and almost all patients require pain management services from a physician. In our sample, the single attribute HUI2 utility score on pain may illustrate a key difference in health status for those in integrated versus end-of-life palliative care programs. Our results could be interpreted that those in the integrated program may not need as much pain management or that those in the integrated program receive pain management services resulting in lower levels of pain. Furthermore, the children and adolescents in our sample had significant ambulation and self-care impairments. These results suggest that personal or nursing care is critical in early integrated programs. Additionally, rehabilitative services, although typically not part of palliative programs, might be of greater need when children and adolescents receive care in the early stages of their illness continuum. It is important to acknowledge that not all of the patients' health care needs would be expected to be treated by the pediatric palliative care team. Sensation and mobility might only be addressed by the patient's primary care provider, whereas emotion and pain might be better addressed by the palliative care team. Integrating primary and pediatric palliative care requires coordination and communication between providers. In a fragmented health care system such as that in the United States, developing an integrated pediatric palliative care program requires a clear definition of what is being integrated, how it is being integrated, defined roles for all of the stakeholders, and timely information on the specific needs of the children and adolescents and their family members.
Fourth, by enumerating the number of unique health status vectors, our results illustrated the high degree of variability in the cohort. Even though this makes it challenging to predict service and staffing needs, our data can still be used to develop strategies to overcome some of these challenges. For example, in traditional palliative care there may be only one provider, or very few providers, in the geographic area that offer care to children and adolescents. The hesitancy of providers to serve these populations may in part be because of cost concerns. One strategy might be to coordinate care among different palliative care organizations. Similar to health plans that offer specialized benefit packages based on the most cost-effective services they provide, pediatric palliative care providers could specialize in their most cost-effective services. Cooperative agreements between hospices and hospitals may be a way to provide the full complement of services and not decrease efficiency. Similarly, multiple hospices could establish pediatric cooperative agreements whereby one hospice provides one type of service (such as nursing care) and the other hospice provides the complementary services (such as psychosocial care). Admittedly, this system would only work under fee-for-service; however, a shared care model might alleviate some of the staffing and fiscal issues associated with providing care to a small group. Shared care models and pediatric palliative care cooperatives should be explored.
Limitations
There are several limitations to our study. First, the response rate was 67%. Although this response rate is consistent with that of prior surveys conducted with this population,47,48 a 2009 study by Knapp et al. noted that black, non-Hispanic parents and parents whose children were in the mid-stage of illness were less likely to participate in surveys (P=0.01 and P=0.04, respectively). 49 Second, the generalizability of our findings are restricted because our sample only included the PIC:TFK program. Parents whose children received care in other states or through private insurance might report different HRQOL, and we have no information about children <5 years of age. Third, we only considered the parent's report of the child's health status. Prior studies are not conclusive as to the congruence between parent and child reports.28, 50–52 It is important to point out that approximately one-third of the children in our program were nonverbal and the same percentage had highly impaired cognitive skills, suggesting that they might not have been able to complete a questionnaire. Fourth, 10–12% of the sample had HUI scores >0.80. Although we did not have ethical approval to review their charts or diagnoses, it may be that these children had risk factors that had not yet developed into important functional limitations and that they could still benefit from the program's services. Finally, we did not ask about specific diagnoses. Oftentimes patients are admitted to the program with more than one life-threatening diagnosis. Solely focusing on diagnoses does not necessarily equate to an understanding of patients' needs, given that functional capacity may vary across stages of disease progression.
Conclusion
Despite these limitations, we believe this is the first study to describe the health status and HRQOL of children and adolescents who are enrolled in an early integrated pediatric palliative care program. This information becomes increasingly important as more states receive approval for similar programs. Recently proposed legislation (United States House Resolution 6931) would allow all states the option to provide Medicaid- eligible children and adolescents palliative in conjunction with curative care earlier than the last 6 months of life. 53 Section 2302 of the 2010 Health Reform Bill (Public Law #111-152) also allows children and adolescents enrolled in public insurance programs to receive palliative and curative treatment concurrently. Consequently, our results could eventually help to guide states on how to determine the effectiveness of these programs. Finally, our study emphasizes the need for more research to understand HRQOL and health status for children and adolescents with life-threatening illnesses.
Footnotes
Acknowledgments
This study was funded by a contract between the Institute for Child Health Policy and the Children's Medical Services Network. Caprice Knapp, Vanessa Madden, and Hua Wang were responsible for study design, data collection, data analysis, and manuscript writing. David Feeny and Dennis Revicki contributed to the data analysis and manuscript writing. Phyllis Sloyer and Charlotte Curtis aided in data acquisition, data interpretation, and approval of the final manuscript.
Author Disclosure Statement
David Feeny has a proprietary interest in Health Utilities Incorporated, Dundas, Ontario, Canada. HUInc. distributes copyrighted Health Utilities Index (HUI) materials and provides methodological advice on the use of HUI. None of the other authors declare a conflict of interest.