
Abstract
Abstract
Introduction:
Pulmonary arterial hypertension (PAH) is a progressive and ultimately fatal disease of the pulmonary circulation. There has never been an investigation of the end-of-life symptoms in patients with PAH. In this investigation, we surveyed surrogates of recent decedents with PAH. We evaluate their responses to better understand the end-of-life experience of patients with PAH.
Methods:
The survey instrument includes demographic information and the Edmonton Symptoms Assessment Scale. Accredo Therapeutics mailed the survey to surrogates of recent decedents with PAH, and responses were anonymously returned to investigators at Virginia Commonwealth University and used in our descriptive analysis.
Results:
Of 100 surveys distributed over 24 months (February 2009 to February 2011), we obtained 36 responses (response rate 36%). We found that most patient deaths (90%) were related to PAH, that the majority of patients died in the hospital (67%), with the majority of in-hospital deaths (83%) occurring in intensive care. Palliative care was infrequently involved in patients' care, and many surrogates were unaware of palliative care and hospice services available to the decedents. Patients died with a high symptom burden, especially dyspnea.
Conclusion:
In this cohort, patients with PAH usually died from their disease, often in the hospital setting with a high symptom burden. Further study will be needed to confirm the findings from this study and to better understand the forces leading to the trends uncovered in this investigation.
Introduction
Methods
Survey instrument
The survey (Fig. 1) was created with assistance from the Virginia Commonwealth University (VCU) Clinical Research Center and was compatible with TELEform software, which recognized patient responses and translated the responses to a secure electronic database. Demographic information for patients and families was collected, but the research team was blinded to identity. The survey instrument included the Edmonton Symptom Assessment Scale (ESAS), a well-validated and reliable tool for assessment of symptoms in the palliative care setting.11,12 Respondents were instructed to complete the ESAS based on their perception of symptoms during their loved one's last days. The ESAS asked the respondent to rate each of eight symptoms (pain, depression, anxiety, dyspnea, well-being, nausea, tiredness, appetite) from 0–10, with a higher score indicating greater intensity. Respondents were also asked to provide specific information regarding the PAH diagnosis and care received by their loved one (including pharmacologic management).
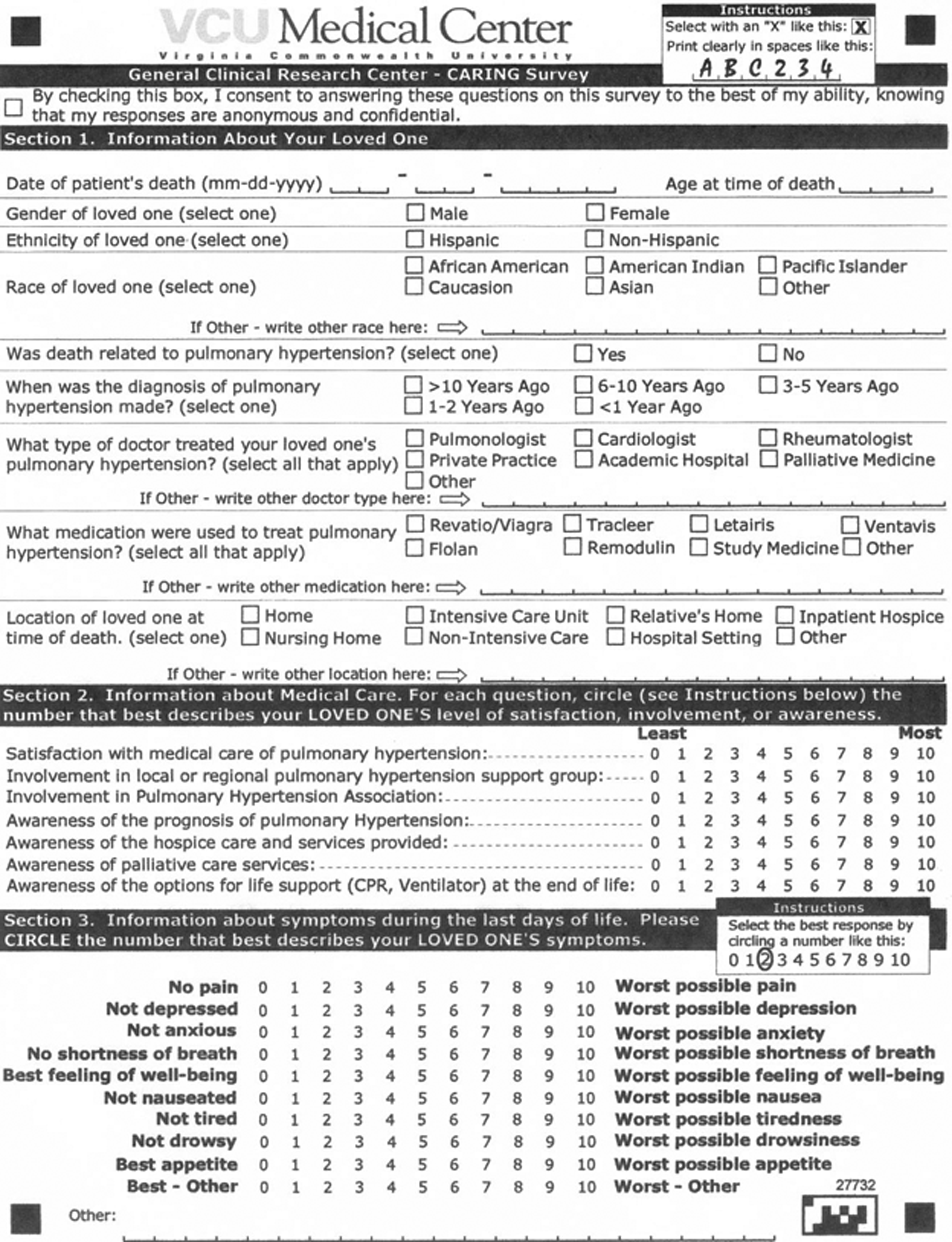
The survey instrument.
Survey distribution
We partnered with regional branches of Accredo Therapeutics to distribute our surveys. Accredo Therapeutics delivers medication, supplies, and training to patients with PAH. Accredo is typically notified by a patient's surrogate when that patient dies. We received permission from PAH centers in the Mid-Atlantic region of the United States. When Accredo learned of a patient's death, a survey was mailed to the next of kin, and a postage-paid envelope without identifiable data was included. On completion of the survey, the respondent would mail it in the provided envelope addressed to VCU.
Statistical analysis
Based on our principal hypothesis and power calculation, we planned to distribute 400 questionnaires and to analyze data using a Wilcoxon signed rank-sum test. However, when it became apparent that our goal for distribution was unobtainable, we focused on a descriptive analysis as our primary means of evaluation.
Results
Of 100 surveys distributed over 24 months (February 2009 to February 2011), we obtained 36 responses (response rate, 36%). Patient characteristics are listed in Table 1. In this cohort, combination treatment was common (53%), and 58% of patients were on prostacyclin therapy. Most patient deaths were related to PAH (90%). Only 11% of patients had a palliative care physician involved in their care. Last, the majority of patients (67%) died in the hospital (Fig. 2). Of those who died in the hospital, 83% died in the intensive care unit.

Location of patients at the time of their death.
PAH, pulmonary arterial hypertension.
As depicted in Figure 3, most surrogates were informed of end-of-life options for their loved ones. Twenty-seven percent of respondents had little to no knowledge (defined as a rating of less than or equal to 3 of 10) of palliative care resources available, 19% had little to no knowledge of hospice resources available, and 58% had little to no knowledge of support group resources available to them.
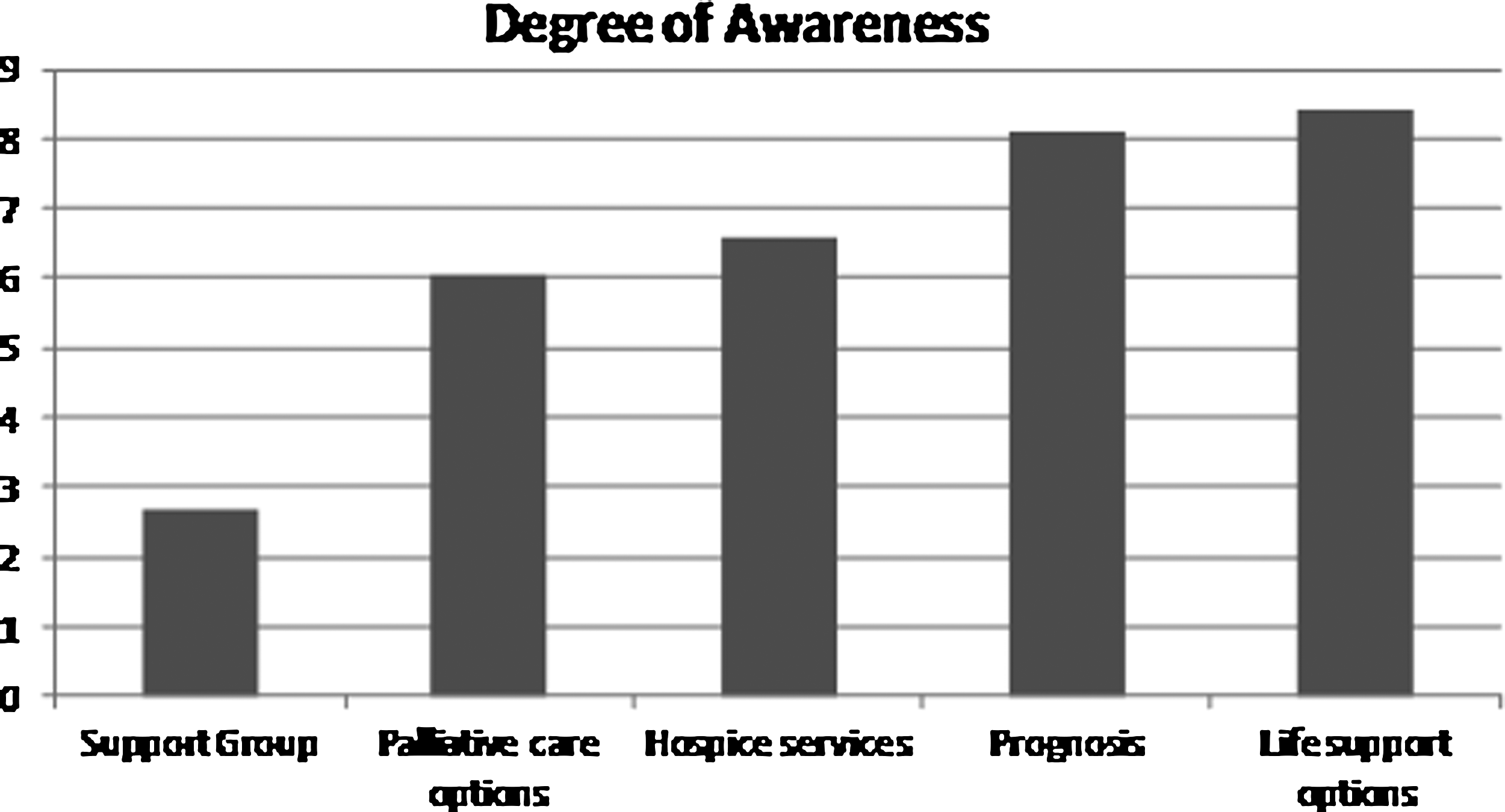
Mean responses regarding the awareness of prognosis and of different services provided. 10 indicates the most awareness, and 0 indicates the least possible awareness.
Mean scores from ESAS symptom domains are reported in Figure 4, and they are compared with previously published results from patients with hematologic or solid malignancies near the end of their life. 13 While direct comparison of responses from our surrogates to other studies that obtained responses directly from patients should be done with caution, we note that our respondents have a very high rating in dyspnea, anxiety, and depression compared with these other cohorts. Last, we added responses from individual ESAS components to make a total ESAS score for each patient. When total ESAS scores were compared between those who died at home (58) and those who died in the hospital (55), no significant difference was found.
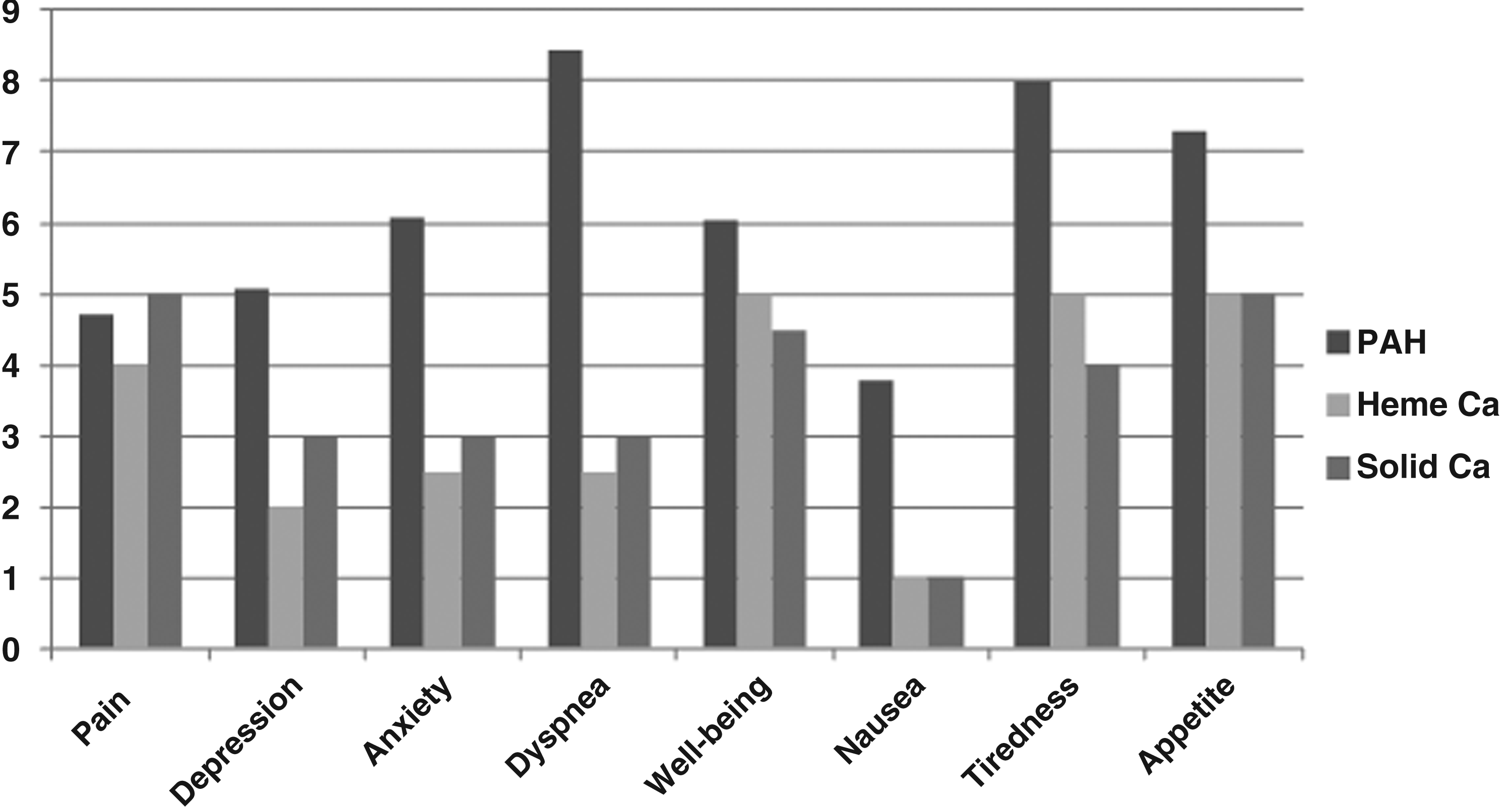
Mean scores from ESAS symptom domains.
Discussion
The prognosis of patients with PAH is equal to or worse than many forms of cancer. PAH places a significant and increasing burden on our health care system, as evidenced by the increasing number of annual hospitalizations and treatment-associated costs. In this study, the surrogates of consecutive patients who died of PAH were mailed a questionnaire with a response rate of 36%. The study was terminated before reaching the targeted response goal because of the lower than expected distribution rate and the lower than expected response rate. We believe the low distribution rate was due to a lower than anticipated death rate. Factors that might have contributed to this include a focused geographic area, as well as lack of knowledge of some deaths. Additionally, surrogates may not have been familiar with our investigator team or grief may have impacted their desire to return a survey, as distribution occurred soon after a patient's death. Last, the survey was sent by Accredo, not the physicians involved in the care. Nevertheless, we believe the information obtained is useful, particular for further hypothesis generation. We believe that our available results provide unique and important information about the end-of-life in patients with PAH and will inform further studies and pilot efforts.
A major finding of our study is that the two-thirds of patients died in the hospital setting, and the vast majority (92%) of deaths were related to PAH. Of patients who died in the hospital, 83% died in an intensive care unit. Our finding contrasts with patient preference in other chronic disease states, where a preference to die at home has been consistently found.13–15 It is possible that the high in-hospital mortality in our study may be related to symptom burden (such as excessive dyspnea) which was difficulty to manage at home, or that dying in the hospital was more comfortable for families and patients. This is supported by our data that symptom burden was perceived as very high compared to solid and hematopoietic malignancies (Fig. 4), 16 and that family members felt well informed regarding options for hospice care. There was no apparent difference in ESAS scores between those dying at home and those dying in the hospital, but this may have been limited by our small sample size and inability to detect a statistically significant difference.
As many hospitals have policies that restrict use of continuous prostacyclin therapy to the ICU or to a monitored bed, this may also have accounted for the increase of deaths in the ICU. Patients receiving long-term prostacyclin therapy are often very hesitant to leave the ICU or hospital ward where staff is proficient with prostacyclin infusion and associated care. 17 At VCU, patients have been treated in a palliative care unit without telemetry where aggressive symptom management could be done, after the goals of care have been firmly established.
Another obstacle to hospice care specific to PAH is cost associated with pharmacotherapy, which is normally continued until a patient's death. For example, patients on a continuous prostacyclin infusion (epoprostanol or treprostinil) often cannot continue this infusion once they enroll in hospice, due to the expense of medication and the concept that aggressive medical treatment is counter to the comfort directed goals of hospice care. Patients may realize that their death could be hastened by the discontinuation of prostacyclin and may have concerns about the symptom burden caused by this discontinuation. Some patients have been reluctant to enter hospice due to a personal moral objection to the discontinuation or downward titration of prostacyclin therapy, viewing it as suicide. 18 Therefore, difficulty in coordinating medical treatment and hospice care may increase the number of in-hospital deaths related to PAH.
It is possible that patients and physicians have different perceptions about the prognosis of PAH compared to diseases with similar prognosis (advanced heart failure and cancer), as discrepancies in perception have previously been cited between diseases with similar prognoses (congestive heart failure and malignancy). 19 This might explain why despite very high observed symptom burden, and a majority of surrogates who reported high levels of knowledge about palliative and hospice services, palliative care providers were involved in only 14% of patients' care. Alternatively, the low involvement of palliative care providers may reflect a paucity of palliative care resources to these patients (due to the anonymity of responses, we cannot determine if palliative care services were available to patients).
Last, the near-term prognosis of patients with PAH is difficult to determine compared with other end-stage disease, which may additionally lead to decreased utilization of hospice services. Nevertheless, patients with PAH have a serious, life-limiting, life-threatening illness with high symptom burden and appear to be ideal candidates for palliative care. In patients with advanced heart failure, enrollment in hospice care is more likely to be associated with discharge from hospice alive compared to patients with cancer, 20 and the disease course with heart failure is more variable. 21 Because patients with PAH typically die of right ventricular failure, challenges in prognosticating advanced heart failure are likely present in PAH. Therefore, difficulty in prognosticating this disease may also influence the high rate of in-hospital mortality.
This study has several limitations. While a retrospective, third-party account weakens the validity of survey results, we felt that this format was the only way to quickly and inexpensively obtain data on a reasonable number of patients. Use of a specialty pharmacy may be less likely in patients with PAH receiving sildenafil or tadalafil monotherapy, and the experiences of those patients may be disproportionately underrepresented. Also, responses came regionally from the eastern United States, and these results may not be readily generalizable to other regions or larger populations. As with any survey, a response bias may exist toward those who complete the survey. Last, the low number of completed responses compared with our anticipated result decreased the power of the study to detect the desired outcomes.
Conclusion
Despite the weaknesses with this study, our results suggest that palliative care and hospice resources are infrequently used in patients with PAH, and that patients often die in an ICU setting with high symptom burden. Over 30% of surrogates were unaware of palliative care resources available, and over 20% of surrogates were unaware of hospice resources available. We believe these findings are hypothesis generating, and given increasing resource utilization, symptom burden and costs associated with care of patients with PAH, that further study is warranted. A prospective intervention involving the early utilization of palliative care,and identifying barriers to hospice resources, may lead to improved patient satisfaction with medical care and lower symptom burden.
Footnotes
Acknowledgments
Funded by Gilead Therapeutics. The views expressed in this article are those of the authors and do not necessarily represent the views of Gilead Therapeutics. We would like to thank Accredo Therapeutics for their role in data acquisition and VCU's Clinical Research Center for assistance with the survey instrument.
Author Disclosure Statement
No competing financial interests exist.