
Abstract

The original Burden Interview was comprised of 22 items; it was later abridged to 12 concise questions by Bédard et al., 2001 (see appendix). The latter version, which was created using the highest item-total correlations, is considered a reliable and valid measure of burden. The two-factor structure (personal strain and role strain) retained an acceptable level of internal consistency (α=0.88 and α=0.78, respectively) and was found to be highly correlated with the original version, boasting correlations that ranged from 0.92 to 0.97. A later study surveying the carers of institutional and community-dwelling patients suffering dementia found support for the two-factor structure (O`Rourke and Tuokko, 2003), adding to the validity that the Burden Interview is a robust measure of burden.
Though widely accepted, the Burden Interview has never been used to measure burden among informal caregivers of palliative home care clients. Caring for a family member suffering from terminal illness is different from caring for a family member diagnosed with dementia or Alzheimer's disease (Grunfeld, Glossop, McDowell, and Danbrook, 1997). Providing care to a family member suffering from Alzheimer's disease is said to be one of the most difficult challenges faced by informal caregivers. Challenges include reduced social skills, disruptive behavior, and personality fluctuations (Chappell, Penning, 1996; Morris, Morris, and Britton, 1988; Schulz, Visintainer, and Williamson, 1990). This may result in chronic stress that will affect the health and well-being of the caregiver. Alternatively, informal carers of terminally ill patients may experience significant psychosocial (Chappell, Penning, 1996), physical, and economic burdens that may reduce the caregivers' quality of life (McMillan, 1996). Considering these important differences, it is difficult to determine whether the factor structure of the Burden Interview will be maintained in the population.
The current study examined the psychometric properties of the Burden Interview. This study postulated that the first nine indicators would load only on the latent construct of personal strain and that the remaining three indicators would load only on role strain. The degree of fit of the hypothesized model was tested using the maximum likelihood chi-square statistic provided in the LISREL output.
Methods
Participants
Participants were the informal but primary caregivers of terminally ill persons receiving palliative home care. Only clients who have an estimated prognosis of six months or less are referred to this home care program. Home care is a type of health care provided in the clients' homes by health care professionals. In Ontario, Canada, palliative home care is distributed by community care access centers. Persons receiving care from a community care access center are referred to as clients. These centers employ care coordinators who assess the clients' needs and develop care plans according to those needs. The care plans are then followed by local health care professionals, including nursing staff and personal support workers. Participants in this study were recruited from two community care access centers.
The study focused on the key informal caregivers of clients who are in the palliative home care program; primary caregivers may have been family members, friends, or neighbors whom the clients relied upon the most often. This definition did not include paid providers of care or agency volunteers. Care coordinators relied on the home care clients to identify key informal caregivers at the time of assessment.
Information about participating in the study was not discussed until after the care coordinators' assessment of the clients' need for care were appropriately assessed. This protocol was followed to ensure that neither the clients nor the caregivers felt pressured to participate in the study. The care coordinators' task was to request permission from the clients to contact their key informal caregivers upon completion of the client interviews. Therefore, the clients and the caregivers had to be present during the assessment to be considered eligible to participate in the study. Additional eligibility criteria included age (18 years of age or older) and the ability to speak, read, and write English. This study was approved by the University of Waterloo's research ethics committee.
To ensure client-caregiver confidentiality, all information that could have identified the caregivers or the clients was removed. A mail-in strategy was used to retrieve the Burden Interview from the informal caregivers. The research package provided to the caregivers included information about the study, a consent form, the Burden Interview, and a prepaid return envelope.
Analysis
Confirmatory factor analysis using LISREL was used to examine the factor structure of the abridged Burden Interview. The normed chi-square (χ 2 /df ratio) was used to determine the extent to which the hypothesized measurement model adequately fit the sample data. A small normed chi-square ratio ranging from 1 to 5 serves as an adequate indicator of good fit, a ratio of less than 1 indicates over-fit, and a ratio greater than 5 represents poor fit (Kline, 1998; Wheaton, Muthen, Alwin and Summers, 1977).
Materials
The 12-item Burden Interview examines role strain and personal strain among caregivers. Each item is measured on a 5-point Likert scale of 1 (never), 2 (rarely), 3 (sometimes), 4 (quite frequently), and 5 (nearly always). This version of the Burden Interview was designed as a self-report survey. Cumulative scores range from 0 to 60, with higher scores reflecting greater levels of burden. This abridged Burden Interview is considered a reliable and valid brief measure of burden that supports the two-factor structure with an acceptable level of internal consistency for each of the two factors of α=0.88 and α=0.78, for role strain and personal strain, respectively.
Results
The palliative home care program care coordinators approached a total of 107 client-caregiver dyads about participating in the study between June and November of 2007. A total of 71 eligible caregivers completed and returned the survey to the researchers, yielding a response rate of 65%. Clients suffered from a number of different types of cancer, chronic obstructive pulmonary disease (COPD), coronary heart failure, and amytrophic lateral sclerosis (ALS). The majority of caregivers were female (70%), a spouse (52%), and comparatively younger (60.7) than the family members being cared for. Many of the caregivers had been providing care to the clients for nearly two years (see Table 1). Few (10%) provided care to others. Number of male and female clients was nearly equal, and the average age of the clients was approximately 74 years. Many of the clients were married (61%) and lived with their spouses.
M, mean; SD, standard deviation.
Totals vary due to missing information.
Abridged scores were high (M=19.89, SD=9.23) compared to scores reported by Bédard et al., 2001 (mean=11.20); O'Rourke and Tuokko, 2003 (males mean 8.29 versus females mean 5.77); and Higginson et al., 2010 (mean=12.0). The average score for personal strain was 23.94 (SD=7.92, min=9, max=40), with a high level of reliability (α=0.90). Scores for role strain averaged 7.95 (SD=2.88, min=3, max=15), with a moderate to high level of reliability (α=0.76).
Factor structure of the Burden Interview
Confirmatory factor analysis examined the factor structure of the 12 abridged Burden Interview items. The model (see Figure 1) showed a χ 2 (53)=131.72, GFI =0.771, AGFI=0.663, and root mean square residual=0.157. This resulted in a normed chi-square (χ 2 /df ratio) of 2.49, well below the ratio of about 5 or less suggested by Wheaton, Muthen, Alwin and Summers (1977).
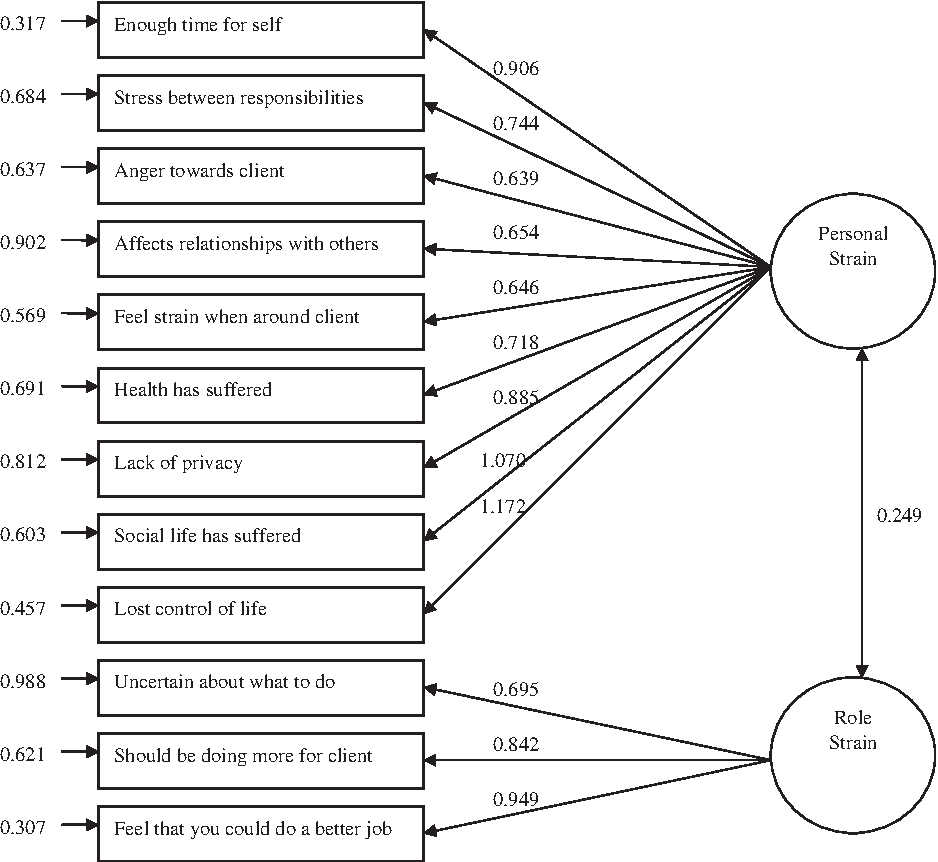
Two-factor confirmatory measurement model: Role strain, personal strain (Lambda scores).
Previous studies have shown that item 5, “Your family member or friend currently affects your relationship with family or friends in a negative way,” cross-loaded on both factors. LISREL's modification index was used to free this linkage, resulting in an improved χ 2 (52)=114.95, GFI=0.801, AGFI=0.701, and root mean square residual=0.146. The difference between the two chi-square values was 16.77.
Discussion
The Burden Interview has been shown to be robust and is considered the gold standard measure of caregiver burden. Subsequent work by Bédard et al. (2001) resulted in the development of an abridged version of the Burden Interview that could easily be used as a screener for the caregivers of cognitively impaired adults. The present study examined the usefulness of the abridged version in assessing caregiver burden among informal caregivers of terminally ill home care clients, a population that is systematically different from cognitively impaired adults. Results of this study showed that overall, burden scores were high compared to Bédard et al. (2001) and O'Rourke and Tuokko (2003), suggesting a higher level of burden compared to populations previously studied.
Confirmatory factor analysis using LISREL supports the two-factor structure of the burden inventory. This study served the purpose of testing the factor structure of the Burden Interview with a sample of informal caregivers of terminally ill home care clients and will contribute to a better understanding of caregiver burden in the home. Use of the abridged Burden Interview during assessment also might help care coordinators to identify client-caregiver dyads at risk of excess caregiver burden. This may be used to support an approach that encourages caregivers to improve their coping methods and/or use respite services. Care coordinators might also modify the care plan to reduce levels of burden and improve outcomes.
The main limitation of this study is that it relied on caregiver volunteers to complete the survey; this may have resulted in a biased sample. Although there is no way to determine if this is the case, anecdotal evidence suggests that care coordinators only approached client-caregiver dyads whose health and prognosis was relatively good. This was the protocol set out by the ethics committee and a reality with research involving vulnerable populations.
This study adds to the evidence that caregiver burden is a significant problem among caregivers of terminally ill home care clients. Results of the confirmatory factor analysis support these findings. What remains unclear is the threshold at which caregiver burden becomes a concern or contributes to excessive problems in the home. The analysis shows that burden can be evaluated using a relatively short inventory of items, like those found in the abridged version of the Burden Inventory. It also sets the stage for a standardized way to assess the well-being of the client and the caregiver, and for the development of programs designed to help informal caregivers who experience burden to cope with the client's illness. This represents an important next step in research.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Appendix
Abridged Zarit Burden Interview (Bédard et al., 2001). All questions are answered as never (1), rarely (2), sometimes (3), quite frequently (4), or nearly always (5).
DO YOU FEEL …
1. because of the time you spend with your relative/friend you don′t have enough time for yourself? 2. stressed between caring for your relative/friend and trying to meet other responsibilities (work/family)? 3. angry when you are around your relative/friend? 4. your relative/friend currently affects your relationship with family members or friends in a negative way? 5. strained when you are around your relative/friend? 6. your health has suffered because of your involvement with your relative/friend? 7. you don′t have as much privacy as you would like because of your relative/friend? 8. your social life has suffered because you are caring for your relative/friend? 9. you have lost control of your life since your relative/friend′s illness? 10. uncertain about what to do about your relative/friend? 11. you should be doing more for your relative/friend? 12. you could do a better job caring for your relative/friend?