
Abstract
Abstract
Background:
Palliative care physicians are increasingly being asked to provide end-of-life (EOL) care for children. Yet very little is known about physicians' level of comfort and willingness to do so.
Objectives:
This study assessed the attitudes of palliative care physicians toward providing care for pediatric patients and to describe the supports they desire in order to do so.
Methods:
An online questionnaire was e-mailed to all physicians in the Division of Palliative Care at the University of Toronto. The questionnaire explored perceptions, attitudes, and level of comfort caring for pediatric patients. Results are reported using frequencies, ratios, and other descriptive analyses.
Results:
Forty-four physicians of the 74 (59%) surveyed responded. On average, physicians cared for fewer than one child per each year of practice. Although the majority of respondents perceived their pediatric training to be inadequate, 70% were willing to provide care to children. Respondents felt at ease applying their knowledge and skills in some aspects of pediatric care (e.g., principles of pain and symptom management, communication about EOL issues) but less so in others (e.g., medication dosing, ethical issues unique to pediatrics). All respondents welcomed opportunities for additional training, but a third felt it was not essential. In particular, the most frequently expressed need was for mentorship by pediatric palliative care specialists.
Conclusions:
Palliative physicians tend to be willing to care for children, but perceive their level of training to be insufficient. Although additional training is endorsed, physicians favored real-time support and mentorship from a pediatric expert.
Introduction
It is believed that most PCPs receive little if any formal training in pediatrics. It is not unusual for practitioners competent and comfortable caring for dying adults to feel unprepared and anxious about doing so for children. 6 Parents of dying children may perceive the discomfort of PCPs, which may lead to reluctance accepting their support.7,8
Despite the increasing need for PCPs to be involved in the care of dying children, only one study, involving three physicians based out of a single hospice in Ireland, has examined this phenomenon. 6 The current study examined the attitudes of a larger sample of PCPs, working in various practice models and settings, towards pediatric patients.
Methods
Study design
A cross-sectional study was undertaken using electronic surveys (FluidSurveys©). A questionnaire link was e-mailed to physician members of the Division of Palliative Care (DPC) in the Department of Family and Community Medicine at the University of Toronto, in September 2010.
Participants
Physicians in the DPC represent a heterogeneous group, diverse in its organizational affiliation and geography. Members may practice individually or within groups; across a variety of settings (home-based, inpatient units, outpatient clinics); and in urban or rural areas. Most have no formal shared-care arrangement with pediatric specialists.
Survey procedure
The study explored attitudes and level of comfort caring for children in the following domains: experience, training and knowledge, managing pain and other symptoms, communication, ethical issues, and overall willingness to provide care. Prior to its use, the survey was piloted by seven palliative experts outside of the province of Ontario. Two follow-up e-mails were sent to participants within a span of four months from the first distribution. This study received approval from the University of Toronto research ethics board.
Statistical analysis
Descriptive statistics (i.e., frequencies) were performed using SPSS Version 19 (SPSS Inc., Chicago, IL). Exploratory bivariate analyses were not possible due to insufficient sample size across multiple categories. Content analysis of responses to open-ended questions was used for context.
Results
Respondent characteristics and pediatric palliative care training
Physicians in the DPC whose work was not limited to adults (n=74) were sent the questionnaire (see Table 1). Respondents cared for <1 child/year on average over their total number of years in practice. Despite the infrequency of pediatric cases encountered, most respondents believed their pediatric exposure during training was inadequate to meet their current needs; 86.0% (37/43) deemed the number of lectures on pediatric palliative care to be insufficient, and 83.3% (35/42) felt they did not have enough pediatric clinical exposure.
DPC, Division of Palliative Care, University of Toronto.
The survey was only sent to physicians and further limited to those who work in a setting in which there was a possibility of caring for a child; physicians working exclusively in adult centers were not invited to participate.
Denominators vary according to the number of respondents for each survey question.
Almost 80% (34/43) believed that their current level of training was inadequate to care for dying children regularly, defined as at least one case per year. Specifically, 95.4% (41/43) of respondents indicated that they would appreciate additional lectures and clinical training in pediatric palliative care if they were required to start looking after pediatric patients on a regular basis. Yet a third of these respondents felt that even though more pediatric training would be beneficial, it should not be required.
Management of pain and other symptoms
More than 50% of respondents reported being ‘somewhat unfamiliar’ or ‘very unfamiliar’ in answering a series of questions related to the management of pain and other symptoms in dying children (range between 56%–73% over five unique items on this theme) (see Table 2). The exception, however, was that slightly fewer (45.2%, 19/42) reported being unfamiliar with the classes of medications used to treat pediatric pain. Respondents demonstrated the least amount of familiarity with respect to dosing of pediatric medications and valued further education in this area most.
n corresponds to number of respondents who answered each question.
Ethics and communication
A majority of respondents reported feeling ‘somewhat uncomfortable’ or ‘very uncomfortable’ with ethical issues related to pediatric palliative care (see Table 3), specifically regarding honesty and truth telling (53.7%, 22/41) and the developing autonomy of the dying child (57.5%, 23/40). In contrast, most felt comfortable (either ‘somewhat’ or ‘very’) facilitating difficult conversations (see Table 4) including talking to families about forgoing life-sustaining treatments (65.9%, 27/41); talking to siblings and friends of the dying child (57.5%, 23/40); and discussing resuscitation preferences with the dying child (57.1%, 24/42).
n corresponds to number of respondents who answered each question.
n corresponds to number of respondents who answered each question.
Willingness to be involved in pediatric palliative care
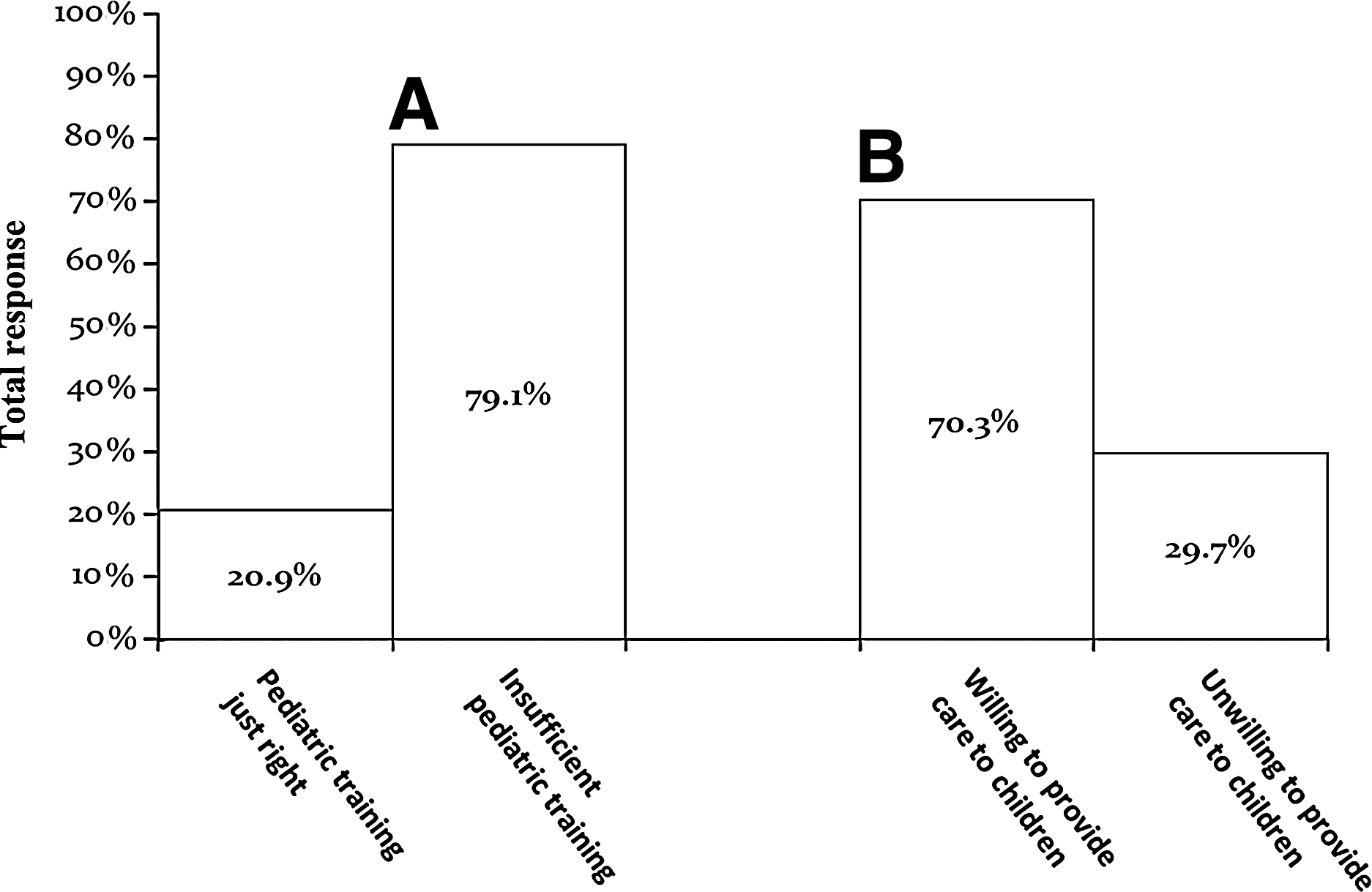
Although 79.1% of respondents reported that they did not have adequate training to regularly provide palliative care to children, 70.3% (26/37) still indicated a willingness to participate in pediatric cases if called upon (see Figure 1). When asked in an open-ended question what would increase their comfort providing care to children, 80% (16/20) of respondents endorsed access to expert pediatric support; only 15% (3/20) favored additional pediatric training. When support was provided by a general pediatrician, 84.2% (32/38) of respondents indicated a willingness to participate in a dying child's care. This increased to 94.7% (36/38) if support was provided by pediatric palliative care consultants. Even with support from a pediatric palliative care specialist, 5.3% (2/38) were unwilling to care for pediatric patients.
Although most palliative care physicians believe they lack sufficient pediatric training (
All respondents valued opportunities for additional pediatric palliative care education. Lectures, workshops, and web-based sessions were endorsed teaching modalities; however, the majority of respondents favored small-group case-based learning (range between 79%–83%, over three unique items about preferred learning methods).
Discussion
Pediatric EOL care for children is primarily provided by a small group of specialists working at children's hospitals, in large urban centers. 3 This centralized model may create challenges facilitating death at home for those living beyond the immediate vicinity. PCPs represent potential partners in overcoming this situation. This is the first study to examine the attitudes of PCPs, working in a variety of settings and practices, towards pediatric patients.
Despite perceptions of inadequate pediatric education and training by most respondents, 70% were willing to provide care to children, even without any additional support. This readiness to care for pediatric patients may reflect a sense of duty among PCPs—if not them, then who? Some respondents identified themselves as the most appropriately trained individual to care for children, which fostered a sense of responsibility: “[I would care for a dying child] if no one else were available who had as much training as me.” In contrast, pediatricians perceive their lack of training9–12 and experience13,14 as barriers to providing palliative care and note that a busy office-based practice is not conducive to the time commitment required. 15
More than a third of respondents reported feeling ‘somewhat’ or ‘very familiar’ with issues related to pain and symptom management, yet most felt unfamiliar with medication dosing. These findings, in conjunction with open-ended responses, may imply that PCPs appreciate that the principles of pediatric symptom management are largely the same as for adults, but practically applying them may differ. “I am very comfortable with adult dosing and adjusting to (weight-based dosing) is not complex. However, my limited clinical experience makes me cautious.”
Communication skills are emphasized in palliative training and are among the primary ‘bedside tools’ of PCPs. 16 This may explain why a majority of respondents felt comfortable having difficult EOL conversations with children. In contrast, respondents felt mostly uncomfortable addressing conflicts involving children, despite frequently having to resolve disagreements with adult patients. 17 The disparity in comfort managing difficult conversations may suggest that PCPs regard the age of the patient to be irrelevant in some situations (i.e., EOL issues), while being germane in others (i.e., when the patient's decision making capacity is in question).
Even though respondents cared for fewer than one child per year on average, and more than 25% had never provided pediatric care, most felt they had received insufficient training in pediatric palliative care. While additional pediatric education was welcomed by all, more than a third did not consider it essential. This may reflect recognition that education, without the opportunity to practice it, will be ineffective. Most respondents advocated learning about pediatric palliative care through ongoing mentorship around individual cases, and willingness to care for children increased if care was shared with a general pediatrician (84%) or pediatric palliative care specialist (95%).
All participants were voluntary members of a division at an academic institution, which may limit generalizability. However, the DPC is an academic affiliation only, not a programmatic or organizational structure. Members belong to independent practices in diverse settings, dispersed over a large metropolitan area, its surrounding suburbs, and some rural areas. At present, PCP training programs in Canada are not required to address pediatric issues. 18 It is possible that PCPs training in places where pediatric competencies are expected, such as in the United States, 19 have different levels of comfort caring for dying children. A comparative study would be valuable.
Conclusion
Although PCPs felt unprepared to care for dying children, most believe that they should do so. Pediatric educational opportunities were endorsed, but the availability of pediatric experts to provide shared-care and mentorship around cases was valued more. Such models will require educational reorganization to appropriately incentivize mentoring. The findings have implications for curricular design, health system organization, and policy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
*
PCPs are individuals who primarily provide care to adult patients (>18 years). Most PCPs trained in Canada complete two years of family medicine followed by one year of palliative subspecialty training with no mandatory pediatric learning objectives.