
Abstract
Abstract
Background:
No method is available for evidence-based glycemic-control management in the context of advanced cancer.
Objective:
This study aimed to analyze, by investigating A1C levels, the necessity of glycemic control in terminal cancer patients with preexisting type 2 diabetes.
Design:
This was a retrospective study.
Subjects:
We analyzed 53 terminal cancer patients who had preexisting type 2 diabetes. All patients first visited Kondo Hospital between April 2002 and December 2006.
Measurements:
We assessed the necessity of glycemic control based on the length of hospitalization and the length of the end-of-life period by using the Kaplan-Meier method and Cox hazard model. Length of the end-of-life period was calculated from the completion of palliative chemotherapy until death. Length of hospitalization was calculated from last admission until death.
Results:
The median length of hospitalization was significantly longer in relatively well controlled patients—with A1C levels <7.5% (49 days; 95% confidence interval [CI] 34.9–63.1)—than in poorly controlled patients, with A1C levels ≥7.5% (23 days; 95% CI 14.6–31.4, P=0.05). The median length of end of life was significantly longer in the relatively well controlled patients (144 days; 95% CI 115.9–172.1) than in poorly controlled patients (45 days; 95% CI 13.8–76.2, P=0.02). Cox multivariate analysis indicated that performance status (PS) at the initial visit to the hospice (hazard ratio [HR] 2.79; 95% CI 1.46–5.32, P=0.002) and glycemic control (HR 2.10; 95% CI 1.18–3.75, P=0.01) were independent, positive prognostic factors.
Conclusion:
Good glycemic control, that is, maintenance of A1C levels at <7.5% during the terminal phase of cancer, conferred a significant survival benefit in cancer patients who had preexisting type 2 diabetes.
Introduction
The A1C test has recently been recommended for diagnosing diabetes. 3 Notably, the American Diabetes Association recommends an A1C level of <7% for most patients. 4 However, many patients receiving cancer treatment fail to reach an A1C level of <7.5%. 5 Studies furthermore recommend A1C levels of 7.0% to 8.0% for frail older adults who have medical and functional comorbidities and for those with a life expectancy of <10 years. 6
During the end-of-life period the primary reason for managing hyperglycemia is not the avoidance of long-term complications, but rather the avoidance of unpleasant osmotic symptoms as well as treatment-associated hypoglycemia. However, there are no guidelines for glycemia-control management in terminal cancer patients. Therefore, to help better determine such guidelines, we retrospectively analyzed the necessity of glycemia control by investigating the A1C levels in terminal cancer patients who had preexisting T2DM.
Materials and Methods
Study population
Overall, 429 patients with malignancies seen in the Tokushima hospice between April 2002 and December 2006 were identified; in these patients, final anticancer therapy had failed and terminal palliative care was therefore indicated. Of these patients, 53 with preexisting T2DM (diabetes group) were included as subjects in this study. We excluded patients who had active hemorrhage, required dialysis or hemolysis, or were undergoing iron or vitamin B12 replacement therapy.
Assessments
The patients' general status and Eastern Clinical Oncology Group performance status (ECOG PS) were assessed. Initiation of terminal palliative care was defined as the date on which established anticancer treatments failed or, for patients who had indeterminate histories, the date of first visit to the hospice.
We assessed the level of glycemic control according to fasting blood glucose levels and A1C findings at the time of (1) the first visit and (2) admission to the hospice. The A1C level was defined as the value at the time of admission. Poorly controlled glycemia during the end-of-life period was defined as an A1C value≥7.5%, and well-controlled glycemia was defined as an A1C value<7.5%.
Length of the end-of-life period was calculated from the completion of palliative chemotherapy until death. Length of hospitalization was calculated from last admission until death.
Statistical methods
Time-to-event data (length of the end-of-life period and length of hospitalization) were summarized using the Kaplan-Meier method and compared using the log-rank test. Prognostic factors were evaluated using the Cox hazard model, with length of hospitalization and length of end-of-life as endpoints; P<0.05 was considered significant. The χ2 test was used for categorical variables. Data were analyzed using IBM SPSS 18 (IBM Corp., Somers, NY).
Results
The median and mean ages in the diabetes group were 72.0 and 70.5 years, respectively. The diabetes group could be subclassified into two groups according to A1C values: poorly controlled patients with A1C values≥7.5% (n=24) and relatively well controlled patients with A1C values<7.5% (n=29). Other characteristics (gender, ECOG PS at admission, diabetes medications, and type of cancer) were not significantly different between the well controlled and poorly controlled diabetes groups (see Table 1).
χ2 test, **Student's t-test
ECOG PS, Eastern Clinical Oncology Group performance status; SD, standard deviation.
In the diabetes group, the median length of hospitalization was significantly longer for the relatively well controlled group (49 days; 95% CI 34.9–63.1) compared to the poorly controlled group (23 days; 95% CI 14.6–31.4, P=0.05). (See Figure 1.) The median length of the end-of-life period was significantly longer in the relatively well controlled group (144 days; 95% CI 115.9–172.1) compared to the poorly controlled group (45 days; 95% CI 13.8–76.2, P=0.02). (See Figure 2.)
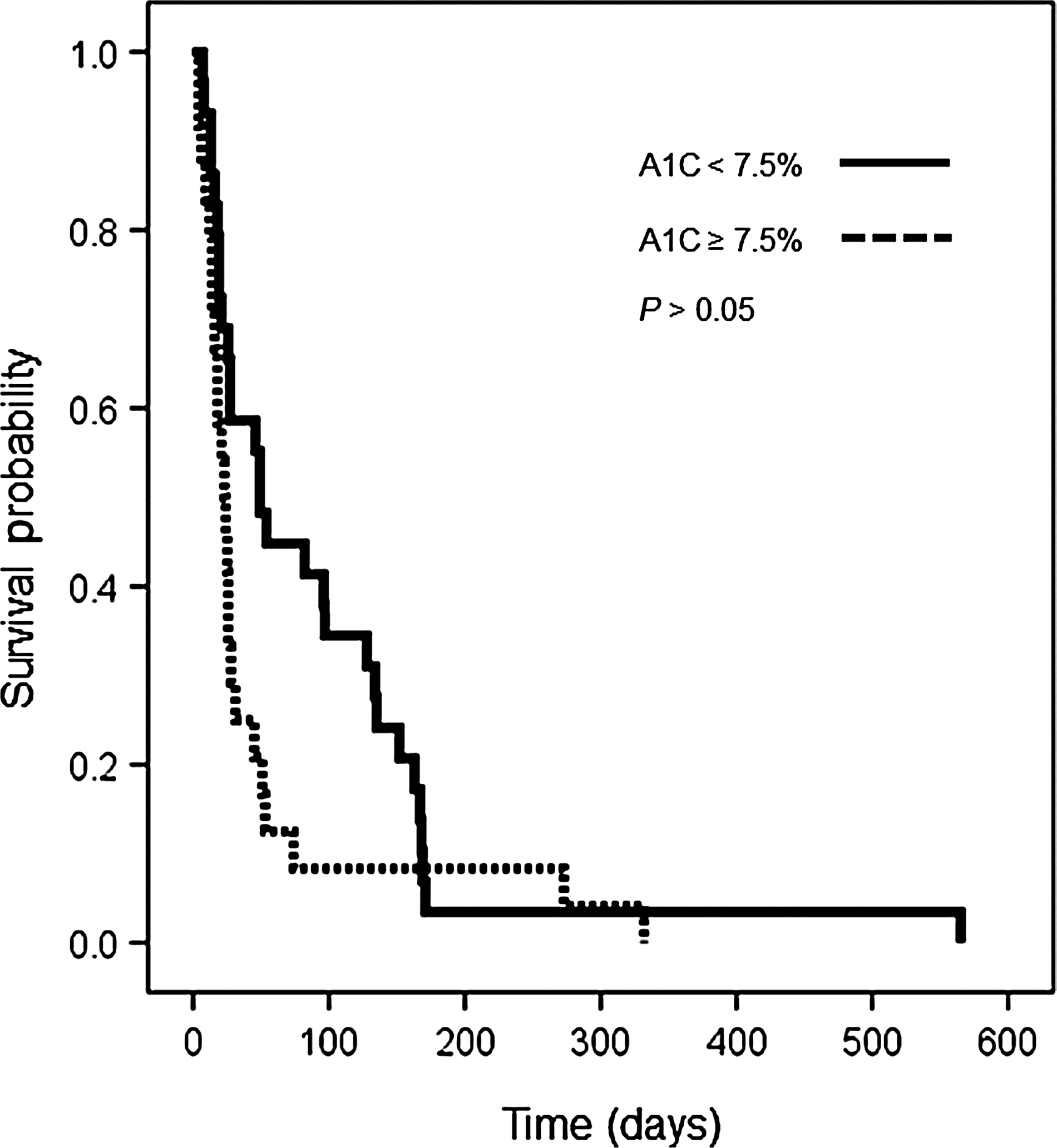
Kaplan-Meier estimates of the length of hospitalization in terminal cancer patients with preexisting diabetes.
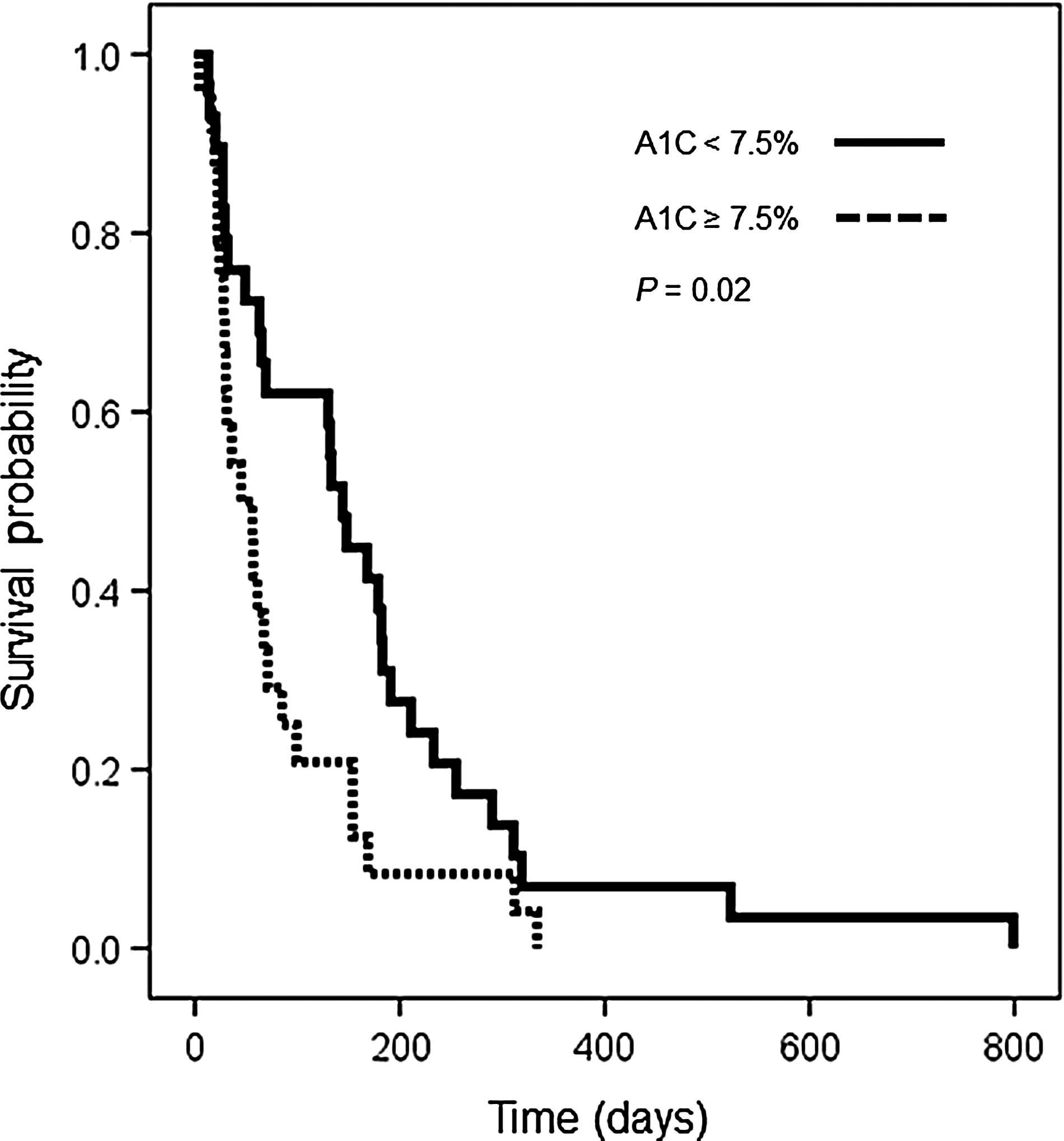
Kaplan-Meier estimates of the length of the end-of-life period in terminal cancer patients with preexisting diabetes.
We used the Cox hazard model to analyze the effect of gender, age, ECOG PS at initial visit to the hospice, diabetes medications, and glycemic control (A1C≥7.5% versus<7.5%) on length of hospitalization and length of end-of-life period. In univariate analysis, three factors were statistically significant predictors of the length of the end-of-life period: ECOG PS at initial visit (HR 3.06; 95% CI 1.66–5.67, P<0.001); diabetes medication (HR 0.52; 95% CI 0.29–0.93, P=0.03); and glycemic control (HR 1.90; 95% CI 1.09–3.35, P=0.03). Multivariate analysis indicated that ECOG PS at initial visit (HR 2.79; 95% CI 1.46–5.32, P=0.002) and glycemic control (HR 2.10; 95% CI 1.18–3.75, P=0.01) were independent, positive prognostic factors in terminal cancer patients with preexisting T2DM (see Table 2). In univariate analysis only ECOG PS at initial visit (HR 2.50; 95% CI 1.38–4.53, P=0.03) was a significant predictor of length of hospitalization.
CI, confidence interval; ECOG PS, Eastern Clinical Oncology Group performance status; HR, hazard ratio.
Discussion
Mortality is moderately higher in patients with concomitant cancer and diabetes than in patients with cancer alone. The management of diabetes in terminal cancer patients is complex, with no guidelines available or consensus among physicians concerning appropriate treatment. In the current study we determined the targeted glycemic control level that affected prolongation of survival. To our knowledge, this is the first study showing that the management of glycemic control using A1C is useful for terminal cancer patients with preexisting T2DM.
There is a clear, optimal level of glycemic control for the prevention of microvascular complications in patients with T2DM. Thus, fasting blood glucose concentration correlates fairly well with A1C values and can be used with A1C to estimate glycemic control. 7 The results of previous trials suggest that a target A1C level of 7.0%–7.9% may be safer than a target level of 6.0% for patients with long-standing T2DM who are at high risk for cardiovascular disease. 8 An A1C level of 7.5% was associated with the lowest levels of all-cause mortality. 9
For terminal cancer patients, quality of life may be affected by osmotic symptoms when levels of glycemia are markedly high and when hypoglycemia associated with diabetes medication and hepatic dysfunction occurs. On the other hand, no clear guidance is available on the preferred glycemia threshold for terminal patients. A previous report suggested maintaining blood glucose concentration between 10 and 20 mmol/l in terminal cancer patients. 10 Repeated blood sugar determinations are uncomfortable for the patient, and so the goal is to maintain blood glucose levels within an acceptable range, with minimal requirement for monitoring. During this period of care, dietary restrictions should not be enforced. Insulin or oral agents should be administered accordingly. 11
Although it is well recognized that some T2DM patients and their families view the continuation of treatment as very important, discontinuation of glycemia monitoring is generally the preferred course of action. 12 A1C levels are monitored using a blood test that correlates the mean blood glucose levels over the previous one to two months; it is used to check that diabetes treatment remains effective. The monitoring of A1C as means of glycemic control negates the need for frequent invasive measurements. Therefore, this testing could offer a simple and acceptable method of detection—if the level of A1C is proven useful as a tool for the management of glycemic control in terminal cancer patients with preexisting T2DM.
Advanced cancer is associated with anorexia-cachexia and weight loss. Anorexia-cachexia, gastrointestinal disturbance, and hepatic derangement directly lead to hypoglycemia, regardless of whether hypoglycemic agents are used. Hyperglycemia in turn leads to unpleasant osmotic symptoms. The causes of hyperglycemia in patients with advanced disease are multifaceted. 13
Certain limitations of this study should be considered, including its retrospective nature and small sample size. However, our results show that the management of glycemic control using A1C is useful for terminal cancer patients with preexisting T2DM. We have planned to conduct a prospective observational cohort study in cancer patients with T2DM by using the A1C level.
Footnotes
Acknowledgments
We appreciate the contributions of the staff of hospice Tokushima in analyzing clinical data. This work was supported in part by the National Cancer Center Research and Development Fund of Japan (23-A-14).
Author Disclosure Statement
There are no conflicts of interest to declare.