
Abstract
Abstract
Background:
The effect of caring for a dying cancer patient on caregiving burden has been explored primarily in Western-based studies with small samples or in studies that did not follow up until the patient's death, but has not yet been investigated in Taiwan.
Objective:
The study's goals were (1) to identify the trajectory of caregiving burden for family caregivers (FCs) of terminally ill cancer patients in Taiwan, and (2) to investigate the determinants of caregiving burden in a large sample and with longitudinal follow-ups, until the patient's death.
Method:
A prospective, longitudinal study was conducted among 193 FCs. The trajectory and determinants of caregiving burden were identified by a generalized estimation equation approach.
Results:
Caregiving burden did not change as the patient's death approached. FCs experienced heavy caregiving burden when their relative suffered from greater symptom distress or if they were spousal caregivers; provided high intensity of assistance to the patient while spending fewer hours providing care; reported financial insufficiency; or had lower social support, fewer psychological resources, or less confidence in caregiving.
Conclusions:
Taiwanese family caregivers' carrry moderate caregiving burden which did not change significantly as the patients' death approached. The effects of caregiving burden while providing EOL care to terminally ill cancer patients may be tempered substantially by enhancing family caregivers caregiving confidence, social support, and psychological resources.
Introduction
Caregiving burden is influenced by contextual factors, i.e., FCs' characteristics and patients' disease-related characteristics, caregiving demands, psychological and social resources, and appraisals of the caregiving situation.9,10 FCs' characteristics such as gender,11,12 age, 11 educational level, 12 and relationship with the patient13,14 affect caregiving burden. Caregiving burden has also been significantly impacted by patients' disease-related characteristics, i.e., proximity in time to death,15,16 severity of symptoms, 17 and functional status.16,17 Another factor suggested to be influential in caregiving burden is the intensity of assistance provided to terminally ill cancer patients. 18
FCs facing the stress and challenge of caregiving have been suggested to be helped by having strong psychological (i.e., coping capability) and social support resources. 19 A person's coping ability in a stressful environment reflects his or her sense of coherence (SOC). 20 We consider the SOC of FCs as their psychological resource for facing the stress and challenge of caring for dying family members. When FCs can find positive meaning in taking care of patients, comprehend caregiving demands appropriately, and have access to relevant resources to manage difficulties in caregiving, their caregiving burden will be lessened.
The caregiving burden of terminally ill patients' FCs has been well studied,12,14,17,21–22 but few studies have used a longitudinal design to examine changes in caregiving burden. Terminally ill patients' physical condition deteriorates quickly. Therefore, caregiving burden may change rapidly in response to patients' changing needs. A cross-sectional design cannot capture the dynamic changes in end-of-life (EOL) caregiving burden. Among the studies7,13,16 that did investigate longitudinal changes in caregiving burden of terminally ill cancer patients' FCs, the samples were small (N<60)7,13 and the attrition rate was high (40%–65%).7,13 Most importantly, these studies13,16 did not follow up with FCs until the patient's death to explore changes in caregiving burden throughout the patients' dying process, and did not comprehensively account for factors influencing EOL caregiving, e.g., contextual factors, caregiving demands, available psychological and social resources, and appraisals of the caregiving situation.
Therefore, the first purpose of this research was to investigate changes in caregiving burden until the patient's death for FCs of terminally cancer patients in Taiwan. Second, this study examined the determinants of caregiving burden from five potential factors: contextual factors, caregiving demands, psychological resources, available social resources, and appraisal of the caregiving situation. A clear understanding of determinants of caregiving burden as cancer patients approach death will help clinicians develop appropriate and effective interventions to reduce caregiving burden.
Method
Study design and sample
This longitudinal and prospective survey study was conducted from November 2007 to October 2009. Participants were recruited by convenience from FCs of terminally ill cancer patients at two medical centers in northwestern Taiwan. FCs were interviewed in person every other week from the time of enrollment until the patient's death. Eligible FCs had to meet the following criteria: (1) had a relative with terminal-stage cancer whose disease continued to deteriorate and was unresponsive to current curative cancer treatments as judged by the patient's physician, (2) were identified by the patient as the person most involved in their actual care, (3) were 21 years of age or older, and (4) were willing to participate and could communicate with the data collectors. The research ethics committees of the study sites approved the research protocol. A written informed consent was obtained from all subjects.
Measures
Outcome variable
Caregiving burden was measured by the Caregiver Reaction Assessment (CRA). 23 The CRA has five subscales: impact on schedule, caregiver esteem, lack of family support, impact on health, and impact on finances. Responses to the 24-item CRA are rated on a five-point Likert scale and are summed together. The total CRA score is computed by averaging scores for the 24 items and ranges from 1 to 5, with higher scores indicating heavier caregiving burden. The reliability and validity of the original five CRA subscales 23 and the derived total CRA score17,22 have been established. In this study Cronbach's alpha for the total CRA score was 0.89.
Independent variables
This study categorized potential predictors of caregiver burden as follows:
(1) Contextual factors: FCs' characteristics included age, gender, relationship with the patient, and the presence of chronic disease. Patients' demographics and disease-related characteristics included age, comorbidities, postdiagnosis survival, and symptom distress. Symptom distress was measured by the Symptom Distress Scale (SDS),
24
which assesses 13 common symptoms of cancer patients. Higher scores indicate greater distress. In this study Cronbach's alpha=0.85. (2) Caregiving demands were measured by the amount of assistance provided in personal care, homemaking, transportation, and health care.
25
Scores for these four items were summed to give a composite score for the intensity of total assistance provided, with a range from 4 to 16. Cronbach's alpha in this study was 0.88. The time spent caregiving each day was categorized as<8, 9–16, and 17–24 hours. (3) Psychological resources were measured by Antonovsky's SOC scale.
20
The 13-item SOC scale has three subscales: meaningfulness, comprehensibility, and manageability. The total score ranges from 13 to 91, with higher scores indicating a stronger SOC. In this study Cronbach's alpha was 0.83. (4) Available social resources were measured by the Medical Outcomes Study (MOS) Social Support Survey (MOS-SSS).
26
The 19-item MOS-SSS assesses emotional, informational, tangible, and affectionate support, as well as positive social interaction. Higher scores indicate better perceived social support. Cronbach's alpha in this study was 0.96. (5) Appraisal of the caregiving situation was measured by the degree of the FC's confidence in knowing what to expect while the patient is dying, what to do at the time of death, and how to take care of the patient at home.
27
Each item was measured on a three-point scale (1=not at all confident, 2=fairly confident, 3=very confident). In this study Cronbach's alpha of the composite score was 0.69.
Data collection
After FCs had agreed to participate they were first interviewed before the patient's discharge from the hospital. Since SOC has generally been recognized as a stable trait of an individual, 28 it was measured only at the initial interview along with FCs' characteristics and patients' demographic and disease-related characteristics. The other variables were measured in face-to-face interviews at roughly two-week intervals until the patient's death.
Statistical analysis
We determined the time proximity to the patient's death as the period between the time of the patient's death and the day the interview was conducted. To illustrate graphically changes in mean CRA scores, we further categorized the time proximity to the patient's death into 1–30 days, 31–90 days, 91–180 days, and >181 days as conventionally used in estimating survival for terminally ill cancer patients. 29 We analyzed the time proximity to the patient's death as a continuous variable to assess its association with CRA total and subscale scores using a generalized estimation equation (GEE). 30 In the multivariate GEE model to identify determinants of caregiving burden, time proximity to the patient's death was analyzed as a categorical variable (with >180 days from the patient's death as reference) to more precisely assess its association with CRA scores as the patient's death approaches.
Results
Of 295 FCs of terminally ill cancer patients enrolled in the study, 69 (23.4%) withdrew from follow-up for various reasons, e.g., occupied by providing care or perceived study participation as too demanding. Among the remaining 226 FCs, 193 lost their ill relative during the study period and comprised the study sample.
At the initial interview, the deceased patients' family caregivers and those who did not complete the follow-ups did not differ significantly in independent variables or CRA scores. However, FCs of the deceased patients provided a higher mean intensity of assistance to the patients (M±SD=12.6±3.5 versus 11.0±3.7, p=< 0.001) than those who did not complete the follow-ups. Furthermore, the FCs of deceased patients perceived that their ill relative suffered from greater symptom distress (M±SD=32.5±8.8 versus 26.8±8.0, p<0.001).
The majority of FCs participating in this study were female (68.9%), married (78.8%), spouse of the patient (46.6%), or an adult child (37.3%) who lived with the patient (80.7%), and had a mean age of 46.3 years (SD=13.1, range=21–83). They had at least a high school education (60.1%), no chronic diseases (68.4%), and reported their financial status as making ends meet (82.5%). Slightly over half (55.4%) of the patients were male, with an average age of 60.2 years (SD=13.9, range=25–93). Common sites of patients' cancer were the stomach (23.8%), pancreas (16.6%), lung (11.9%), colon-rectum (10.9%), and breast (5.7%). The majority of patients (59.1%) had comorbidities. On average, the patients had been diagnosed with cancer for 23.4±29.0 months (range=1–202, median=13.0) when the FCs were first interviewed. Patients' mean survival time after the FCs enrolled into this study was 74.2±82.5 days (range=1–367; median=39), with the proportions of patients surviving 1–30, 31–90, 91–180, and >181 days as 41.5%, 28.5%, 18.7%, and 11.4%, respectively. On the whole, FCs were interviewed 7.0±7.2 times (range=1–30; median=5.0).
Trajectory of caregiver burden
Results of simple GEE analysis showed a nonsignificant, decreasing linear trend in caregivers' mean total CRA score (β=-0.011, p=0.11; see Table 1) over time away from the patient's death (see Figure 1). The mean total CRA scores (SD) at 1–30, 31–90, 91–180, and >181 days from the patient's death were 2.50 (0.43), 2.47 (0.50), 2.49 (0.54), and 2.41 (0.54), respectively. However, the CRA subscale scores for Schedule (β=-0.006, p=0.03) and Health (β=-0.004, p=0.01) decreased significantly with increasing time away from the patient's death. CRA subscale scores for Lack of Family Support, as well as for Impact on Finance and Self-Esteem did not change significantly as the patient's death approached (see Table 1 and Figure 2).

Pattern of changes in family caregivers' total Caregiver Reaction Assessment subscale scores during the dying process for Taiwanese terminally ill cancer patients.
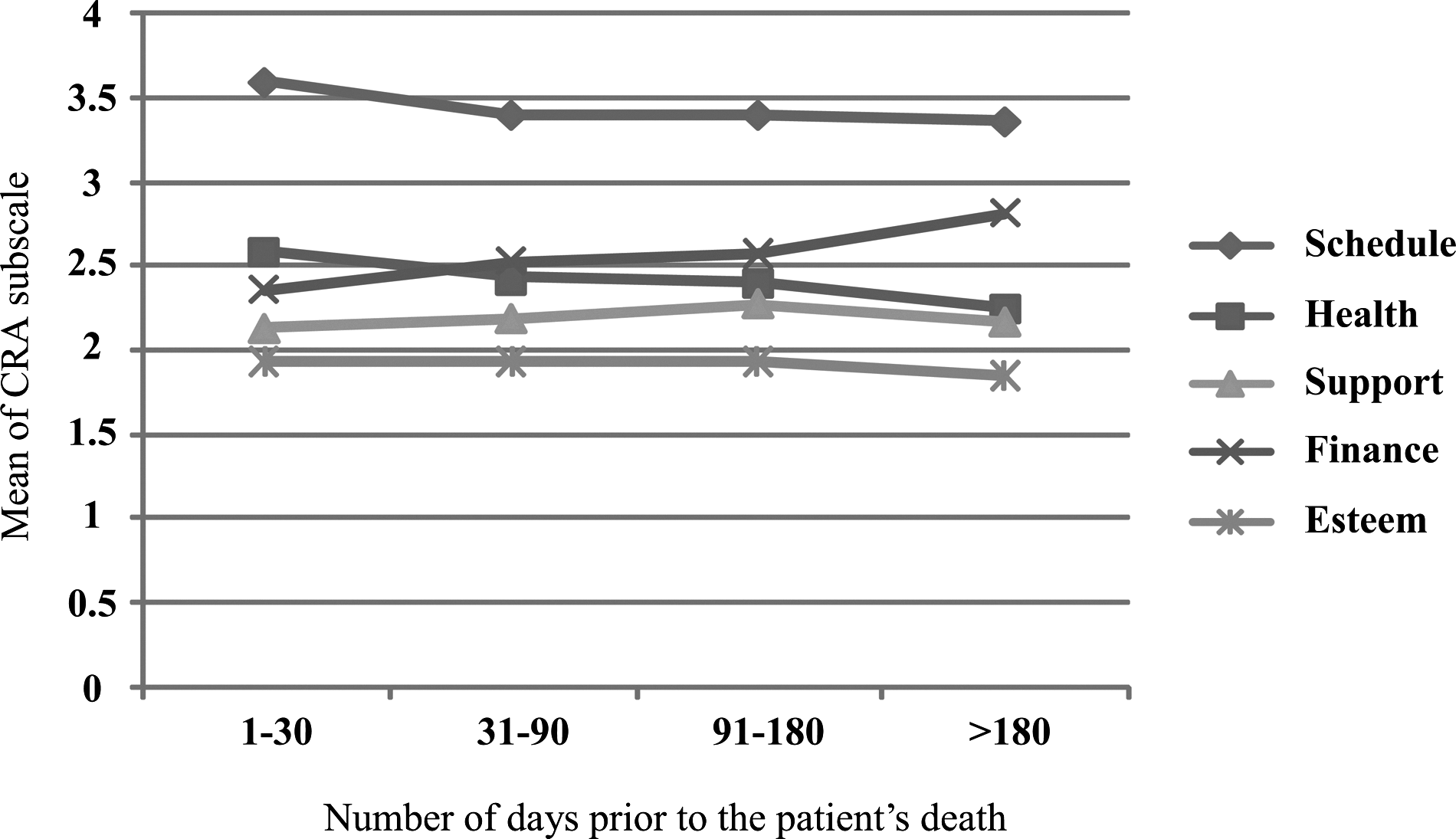
Pattern of changes in family caregivers' CRA subscale scores during the dying process for Taiwanese terminally ill cancer patients.
Determinants of caregiver burden for family caregivers of terminally ill cancer patients
The results of multivariate GEE analyses of associations between total CRA scores and independent variables are presented in Table 2. FC burden was not significantly predicted by the time proximity to the patient's death. In the GEE model, however, seven factors remained significant. FCs experienced a higher level of subjective caregiving burden if they were the patient's spouse (β=4.209, p=0.01), had insufficient financial support (β=3.814, p=0.03), their ill relative suffered from a higher degree of symptom distress (β=0.107, p=0.05), and they provided higher intensity of assistance to the patient (β=0.438, p=0.001). Caregivers who spent <8 and 9–12 hours/day providing EOL care to their ill relative also reported significantly greater caregiving burden than those who spent 13–24 hours/day (β=1.879, p=0.02 and 1.639, p=0.02, respectively). In contrast, lower caregiving burden was experienced by FCs who perceived stronger social support (β=−0.162, p<0.001), had stronger SOC (β=−0.129, p=0.01), and reported higher confidence in providing EOL care (β=−0.600, p=0.003) to their ill relative.
CRA, Caregiver Reaction Assessment; GEE, Generalized Estimation Equation; Ref*, reference group; SE, standard error.
Discussion
This study shows changes in caregiving burden of FCs of terminally ill cancer patients over the 180 days before their death in Taiwan. The CRA scores measured at different times during this period indicate that providing EOL care to a terminally ill Taiwanese cancer patient was only at a moderate level (mean [SD] scores ranged from 2.41 [0.54] to 2.5 [0.43] on a 1–5 Likert scale). These scores are slightly higher than those reported for FCs of terminally ill cancer patients in the United States (2.2) 14 and Norway (2.3). 22 For CRA subscale scores, our results are similar to those of other studies,12,14,21 indicating that the impact of caregiving on self-esteem is the lowest, whereas the impact on daily schedule is the highest. Our CRA scores may reflect the influence of Confucianism and familism, which recognize filial piety as the most important virtue in Chinese culture and regard caring for family as a responsibility and compulsory duty. 31 Failure to fulfill one's duty and obligations of caring for an ill/dying relative often leads to feelings of guilt and shame as well as social blame for offenses against filial piety. 32 Therefore, our participants only recognized their caregiving burden as moderate, and its impact on their self-esteem was lowest even when their relative's death approached. However, caregiving in Chinese culture focuses more on practical assistance than emotional expression, 32 resulting in caregiving burden having the greatest impact on daily schedule.
Our results showed that overall caregiving burden did not increase significantly as the patient's death approached. This result is the same as for Australian caregivers, 21 but in contrast to that for Canadian FCs. 7 However, as previously reported,16,33 we found that the impact of EOL caregiving on Taiwanese FCs' schedule and health increased significantly as the terminally ill cancer patient's death came closer. As terminally ill cancer patients' physical condition deteriorates, 16 the caregiving impact on FCs' schedule obviously rises and the caregivers' physical health worsens and exhaustion appears.
The multivariate GEE results indicated that FCs suffered greater caregiving burden (1) when their relative experienced greater symptom distress, (2) if they were spousal caregivers, provided high intensity assistance to the patient, spent fewer hours in caregiving, and reported financial insufficiency, and (3) when they had lower social support, psychological resources, and confidence in caregiving. Our finding that spousal caregivers had greater caregiving burden differs from other research. 16 According to the familistic view, married women must fulfill the expectations of a patriarchal culture by obeying and taking care of their husbands; they are also expected to refrain from expressing any sense of pressure and difficulty when providing EOL care to their loved one. 34 Therefore, our largely female sample of Taiwanese spousal caregivers may have experienced a higher degree of caregiving burden.
We found that caregiving burden was positively influenced by higher intensity of total assistance provided and the patient's greater symptom distress, in line with the literature. 16 Our results also showed that FCs with higher confidence in caregiving had lower caregiving burden, as previously reported. 18 However, our results differed from a previous report 18 by showing that the less time caregivers spent each day in providing EOL care, the higher caregiving burden they experienced. In our study, the proportions of FCs with a full- or part-time job and spending <8 hours, 9–12 hours, and 13–24 hours/day in caregiving were 64.0%, 43.8%, and 24.2%, respectively. Thus, FCs with a full- or part-time job may bear both caregiving burden and job stresses. Similar to previous reports, our results showed that higher income12, 14 and stronger family and social support of FCs13,14,35 may lower caregiving burden. We also found caregivers with stronger SOC had lower caregiving burden due to their greater coping capabilities. 36
This research had several limitations. First, we used convenience sampling to select research participants. Thus, the findings may not be generalizable to all Taiwanese FCs of terminally ill cancer patients. Second, we did not explore in-depth the impact/influence of Chinese cultural norms (such as sense of filial obligation or commitment to the family and the intensity of cultural affiliation with Confucianism and familism) on caregiving burden. Finally, we did not cover other potential variables that influence caregiving burden such as depression, anxiety, and quality of life. To more comprehensively understand the factors predisposing and buffering caregiving burden for family caregivers while providing EOL care to their dying relative, further research should incorporate a broader scope of potential influencing factors, i.e., the intensity of cultural affiliation with Confucianism and familism as well as caregivers' depression and anxiety.
In conclusion, our results demonstrated that Taiwanese FCs experience moderate caregiving burden, which did not change significantly as the patient's death approached. The effects of caregiving burden while providing EOL care to terminally ill cancer patients may be tempered substantially by enhancing FCs' caregiving confidence, social support, and psychological resources. Therefore, caregiving burden may be decreased by developing strategies to enhance FCs' caregiving skills and to facilitate financial and social support. Health care providers can also strengthen FCs' psychological strength, e.g., by helping them to find meaning in caregiving, to appropriately recognize caregiving demands, and to mobilize resources to efficiently cope with the demands of caregiving. By doing so, Chinese/Taiwanese FCs may fulfill their filial obligation without suffering from extraordinary caregiving burden.
Footnotes
Acknowledgments
This study was supported by the National Health Research Institute (NHRI-EX94-9806PC and NHRI-EX101-99006PI
Author Disclosure Statement
No financial or other conflict of interest was involved in this study. None of the funding sources had any role in designing and conducting the study; collecting, managing, analyzing, and interpreting the data; or preparing, reviewing, or approving the manuscript.