
Abstract
Abstract
Background:
Uremic pruritus is a common and distressing symptom occurring in 42% to 75% of end-stage renal dialysis (ESRD) patients, even in patients who are adequately dialyzed.
Methods:
We conducted a retrospective review of consecutive patients who presented to the renal palliative care clinic in a single institution with pruritus refractory to antihistamines between April 2011 and September 2012. A total of 99 patients were screened during this period; 20 were eligible for this study. Sertraline was initiated at 25 mg daily orally for the first month, with dosage increment of 25 mg monthly according to clinical response up to a maximum of 200 mg daily as necessary. Patients were followed up every 2 to 4 weeks in the renal palliative care clinic.
Results and Conclusions:
Study results showed that low-dose sertraline was effective for antihistamine-refractory uremic pruritus in renal palliative care patients. Further placebo-blinded randomized-controlled studies are warranted to clarify our findings.
Introduction
The pathophysiology of uremic pruritus is poorly defined and, as a result, the development of specific therapies has been a challenge. Numerous therapies have been attempted; however, none has been proven definitive. For instance, although topical tacrolimus was found to be effective based on an uncontrolled observation, 13 a vehicle-controlled study of the same product demonstrated no efficacy. 14 Topical agents that are currently recommended without evidence-based support for uremic pruritus include capsaicin, corticosteroids, and emollients. 15 Other therapies are often inadequate and poorly tolerated. A placebo-controlled double-blind study in 25 patients with ESRD-associated pruritus found that 300 mg of oral gabapentin administrated after each hemodialysis session was effective for ESRD pruritus; however, its safety in ESRD patients not on dialysis has not been evaluated so far. 16 Nalfurafine (TRK-820), a kappa-receptor agonist, showed an antipruritic effect in the treatment of uremic pruritus in patients on hemodialysis, but it is not available commercially yet. 17 The 5-HT3 antagonist, ondansetron, has been suggested as a possible therapeutic intervention for uremic pruritus. In a systemic review, it was demonstrated to have negligible effect on uremic pruritus. 18
Antidepressants have been used to treat pruritus. Several studies have shown paroxetine, a selective serotonin reuptake inhibitor (SSRI), to be effective in the treatment of systemic itch of different types due to neurotic excoriations, atopic dermatitis, systemic lymphoma, and solid carcinoma.19–23 Mirtazapine, which is a noradrenergic and specific serotonergic antidepressant (NaSSA), has been reported to be effective in the treatment of itch associated with primary biliary cirrhosis, ESRD, and lymphoma. 24 However, both paroxetine and mirtazapine require dosage adjustment in ESRD, especially in patients not on dialysis. Sertraline is a suitable alternative as it does not require dosage adjustment in ESRD. 25 Previous reports have indicated that sertraline can improve pruritus related to liver cholestasis 26 or psychogenic pruritus. 27 A recent open-labeled small-scale study showed it might be useful for the treatment of uremic pruritus in patients with ESRD on hemodialysis. 28
Methodology
Patients
Retrospective review of consecutive patients who presented to the renal palliative care clinic in a single institution with pruritus refractory to antihistamines between April 2011 and September 2012 was performed. A total of 99 patients were screened during this period; 20 were eligible for this study. All were Chinese-Cantonese patients aged 18 years or above, with stage 5 ESRD (defined as glomerular filtration rate of <15 mL/min/1.73 m2) managed conservatively without dialysis. Patients had ESRD-related chronic pruritus for 6 weeks or more, uncontrolled on antihistamines. Subjects were excluded if they had primary skin disorders causing pruritus, such as atopic dermatitis or urticaria, or exposure to new skin products or infections associated with pruritus. Patients already on antidepressants, opioid antagonists, corticosteroids, immunosuppressants, capsaicin, cholestyramine, or ultraviolet B phototherapy prior to the study, and those with any contraindications for sertraline were also excluded. All patients consented to the study.
Follow-up procedures and study outcomes
Baseline laboratory tests including complete blood count, liver and renal function tests, and serum levels of sodium, potassium, calcium, and phosphate were obtained. Sertraline was initiated at 25 mg daily orally for the first month, with dosage increment of 25 mg monthly according to clinical response up to a maximum of 200 mg daily as necessary. Patients were followed up every 2 to 4 weeks in the renal palliative care clinic. No other medication change, including use of over-the-counter agents, was allowed during the treatment period. The severity of pruritus was assessed by using Numerical Rating Scale (NRS), which consisted of numerical scores from 0 (no pruritus) to 10 (worst ever imaginable pruritus), on every patient visit by the same investigator. The primary outcome was defined as the pruritus NRS when the patient had subjective satisfactory control of pruritus (“time to control”) at the minimum dosage of sertraline that was effective (“effective dosage”). Other aspects of pruritus including anatomical distribution (localized or generalized), duration, frequency (similar throughout the day, worse in daytime or night-time), sleep (mildly, moderately, severely, or not affected) and concomitant depressed mood were recorded at each visit. Evaluable patients were defined as patients who had completed at least 2 weeks of treatment.
Statistical analyses
Wilcoxon signed-ranked test to compare means was used. Statistical analyses were performed using the statistical software SPSS Statistics, version 19 (SPSS Inc., Chicago, IL). Significance was assumed at p<0.05.
Results
Patient demographics
Twenty patients were recruited (Table 1). The mean age was 81 years (range 56 to 92 years). The majority (70%) were female. The mean plasma creatinine level was 7.2 mg/dL (range 2.75 mg/dL to 10.37 mg/dL), urea was 98.25 mg/dL (range 30.81 mg/dL to 164.99 mg/dL), and phosphate was 4.38 mg/dL (range 1.86 mg/dL to 5.88 mg/dL). The causes for ESRD in the patients included diabetes mellitus (50%), hypertension (25%), and others. They had pruritus for a mean duration of 13.6 months (range 8 to 20 months) before the study. Most patients (70%) reported generalized pruritus; others had localized pruritus. Excoriation was found in none of these patients. Thirteen patients (65%) had pruritus of similar severity throughout the day, whereas in the remaining patients pruritus was worse at night. Activities of daily living were mildly affected in 75% of the patients, moderately affected in 20%, and severely affected in 5%. Sleep was mildly, moderately, and severely affected in 45%, 40%, and 15% of the patients, respectively. Concomitant depressed mood was observed in 25%.
Pre-NRS was the pruritus score in the range of 0–10 before receiving sertraline.
Post-NRS was the pruritus score in the range of 0–10 when the patient had subjective satisfactory control of pruritus with minimum dosage of sertraline.
N18, N19, and N20 were nonevaluable patients.
Plasma Cr (normal range 0.7–1.4 mg/dL). Plasma urea (Normal range 10–20 mg/dL).
Plasma PO4 (normal range 2.54–4.33 mg/dL). Plasma bilirubin (normal range 0.23–1.35 mg/dL).
Cr, creatinine; CrCl, creatinine clearance; PO4, phosphate.
Response to sertraline
There were 17 evaluable patients who responded to sertraline after a mean duration of 5.1 weeks (range: 2 to 12 weeks) on treatment. The mean±standard deviation (SD) pre- and post-treatment NRS were respectively 7.47±1.605 and 2.47±1.281. The pruritus NRS significantly reduced by a mean of 5 after sertraline treatment (p<0.01) (see Fig. 1). The mean effective dose was 35 mg (range 25 mg to 75 mg) and the median was 25 mg.
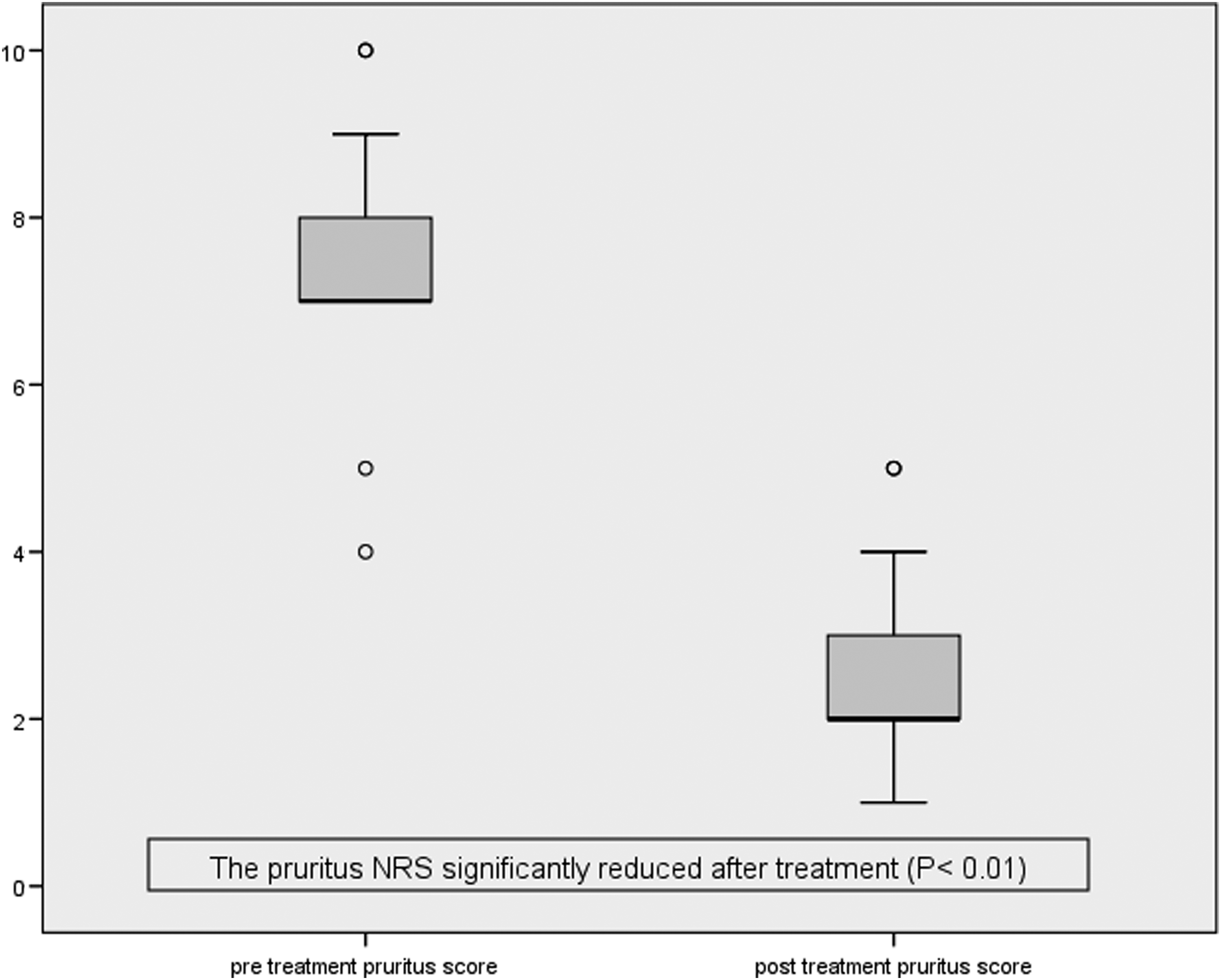
Box-Plot of NRS before and after treatment with sertraline.
Adverse effects
Sertraline was generally well-tolerated. However, side effects of dizziness and fatigue were observed in three patients (15%), and discontinuation of the medication was preferred by these patients after a mean on-treatment period of 4.7 days.
Discussion
This report presents first evidence that sertraline can reduce uremic pruritus in renal palliative care patients not on dialysis. The exact mechanism by which sertraline might improve pruritus is not known. It inhibits neuronal reuptake of serotonin, resulting in increased local concentration of serotonin in the synaptic cleft. Serotonin plays different roles depending on its location of action. In peripheral unmyelinated polymodal C fibers, it leads to excitation and the perception of itch.29–31 In the central nervous system, however, it reduces transmission of nociceptive stimuli through inhibitory pathways that descend from the midbrain to the dorsal horn.32,33 This might account for the antipruritic and analgesic effects of SSRIs.34,35 Finally, the antidepressant effect of sertraline might enable patients with concomitant mood disturbance to cope better with their pruritus.
In this study, we chose a starting sertraline dosage of 25 mg. This is in concordance with a dose-escalation protocol suggested for liver pruritus, although the optimal dosage reached 75mg to 100 mg in the particular study. 26 In another study investigating sertraline in ESRD patients on dialysis, sertraline at a fixed dose of 50 mg showed antipruritic effect. 28 As for the treatment of depression, the usual dosages ranged from 50 mg to 200 mg. 36 Interestingly, the median effective dosage to control pruritus in our study remained a low dose at 25 mg. This observation may imply that the role of serotonin in the pathogenesis of renal pruritus and other conditions are different, and that the mechanisms of action of sertraline in these conditions are also distinct. Importantly, the use of low-dose sertraline can control symptoms while minimizing side effects associated with higher dosages. Low-dose sertraline was shown in the present study to be well tolerated. Moreover, dosage adjustment according to renal function is not necessary with sertraline as opposed to other commonly used SSRIs in palliative care37–39 ; this supports its role in the management of uremic pruritus in ESRD patients. Compared with paroxetine, the “time to control” is longer (3.6 weeks versus 5.1 weeks) when sertraline was used. 20 The faster action of paroxetine might be due to its higher serotonin reuptake inhibitory effect. 40 Antihistamines are frequently prescribed for renal palliative care patients despite often not being useful. 41 Antihistamine-refractory patients are therefore a significant clinical burden. The present study was designed to provide insights into treatment of these patients, and also to eliminate any confounding effect of concomitant antihistamines. Our results demonstrated the efficacy of sertraline in this setting.
There were several limitations in the current study. First, there were a small number of participants and lack of a control arm, although consecutive patients were recruited to minimize selection bias, and the results were significantly positive and readily appreciated. Second, the full side-effect profile and duration of effect of the medication were not fully evaluated. In addition, there might be placebo effect given that all the patients knew they were taking the active drug, which might result in subjective improvement in symptoms. Furthermore, pruritus, like other symptoms, might improve spontaneously. Finally, the causes of uremic pruritus, for example, psychogenic or peripheral neuropathy, were not classified; this might have pathogenesis and treatment implications.
Conclusion
The present study showed that low-dose sertraline was effective for antihistamine-refractory uremic pruritus in renal palliative care patients. Further placebo-blinded randomized-controlled studies are warranted to clarify our findings.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. W. K. Lo, Consultant, Renal Unit, Tung Wah Hospital, Hong Kong, for his support and advice on the management of renal palliative care patients.
Author Disclosure Statement
No competing financial interests exist.