
Abstract
Abstract
Context:
Methadone is increasingly being used to treat patients whose pain does not respond well to other opioids. Advantages over morphine sulphate and its alternatives include low cost, lack of active metabolites and efficacy against neuropathic pain.
Objectives:
To describe our experience with opioid rotation to methadone and compare the morphine to methadone ratios to previously published data; To discuss two commonly used rotation methods - the Edmonton and Morley-Makin methods.
Method:
We describe two cases with cancer pain successfully switched to methadone. In both cases the dose of the previous opioid was limited by development of opioid toxicity. We used the Morley-Makin conversion method and modified it by reducing the ‘as required’ dose by a third. The initial methadone doses for these cases were lower than predicted doses.
Conclusion:
In cases where cancer patients fail to respond or develop tolerance to opioids, conversion to methadone is a reasonable approach. Although equianalgesic tables may not always predict final methadone doses, when properly selected can be useful tools for the experienced clinician. A customised and cautious approach is thus advisable when rotating to oral methadone, especially in patients who have experienced opioid toxicity.
Introduction
Conversion Methods
There are two commonly used methods of rotating opioids to methadone. The Edmonton method is a three-day switching method that involves a gradual replacement of the previous opioid with methadone.3,6 On the first day the opioid is reduced by a third and replaced by an equivalent amount of oral methadone in three daily doses. The morphine to methadone ratio used is 10:1 for patients on up to 300mg of morphine and 12:1 for those on higher doses. If the patient continues to complain of pain on the second day, a further reduction in their original opioid by a third and a similar increase in methadone follows. If pain is not a problem, the methadone dose is left unchanged. The switch is completed on the third day, when the original opioid is discontinued and the methadone dose increased if indicated. 3
The second method, known as the Morley-Makin method, involves discontinuing all previous opioid and using 10% of the morphine equivalent daily dose as the methadone dose given on an as-required basis every three hours. 7 The maximum dose of methadone that can be given is set at 30mg to prevent potential toxicity. If the patient requires a breakthrough dose before the allowed three hourly methadone doses, their previous breakthrough opioid dose is used. On day six the methadone requirement over the last two days is calculated and the patient is switched onto a twice-daily regimen.
We present two cases that were successfully rotated to methadone resulting in pain control at initial doses that were lower than predicted.
Case 1
A 42-year-old woman with a diagnosis of metastatic squamous cell cancer of the cervix was admitted to our inpatient unit with a history of back pain and lower limb swelling. She had a relatively high burden of disease with widespread lymphadenopathy particularly in the pelvis, abdomen, and supraclavicular areas. At the time of diagnosis she also had extensive bony and pulmonary metastases. Despite treatment with radiotherapy to her pelvis and lumbar area she continued to complain of back pain radiating down to her thighs. It was felt that her pain was both neuropathic and nociceptive, and we continued to titrate her oxycodone to 100mg twice daily and pregabalin to 150mg twice daily. Unfortunately, her pain escalated and she developed opioid toxicity and was rotated to hydromorphone 24mg twice daily (using conversion ratios morphine:oxycodone 1.5:1 8 and morphine:hydromorphone 5:16,9 with a dose reduction). Neither her pain nor the opioid toxicity improved on hydromorphone. In view of the neuropathic nature of her pain, we decided to rotate her opioid to methadone with the aim of achieving better pain control and reversing the opioid side effects. We opted for a modified Morley Makin regimen given the history of toxicity and the fact that there had been a recent escalation of her opioids. (See Tables 1 and 2 and Fig. 1.)
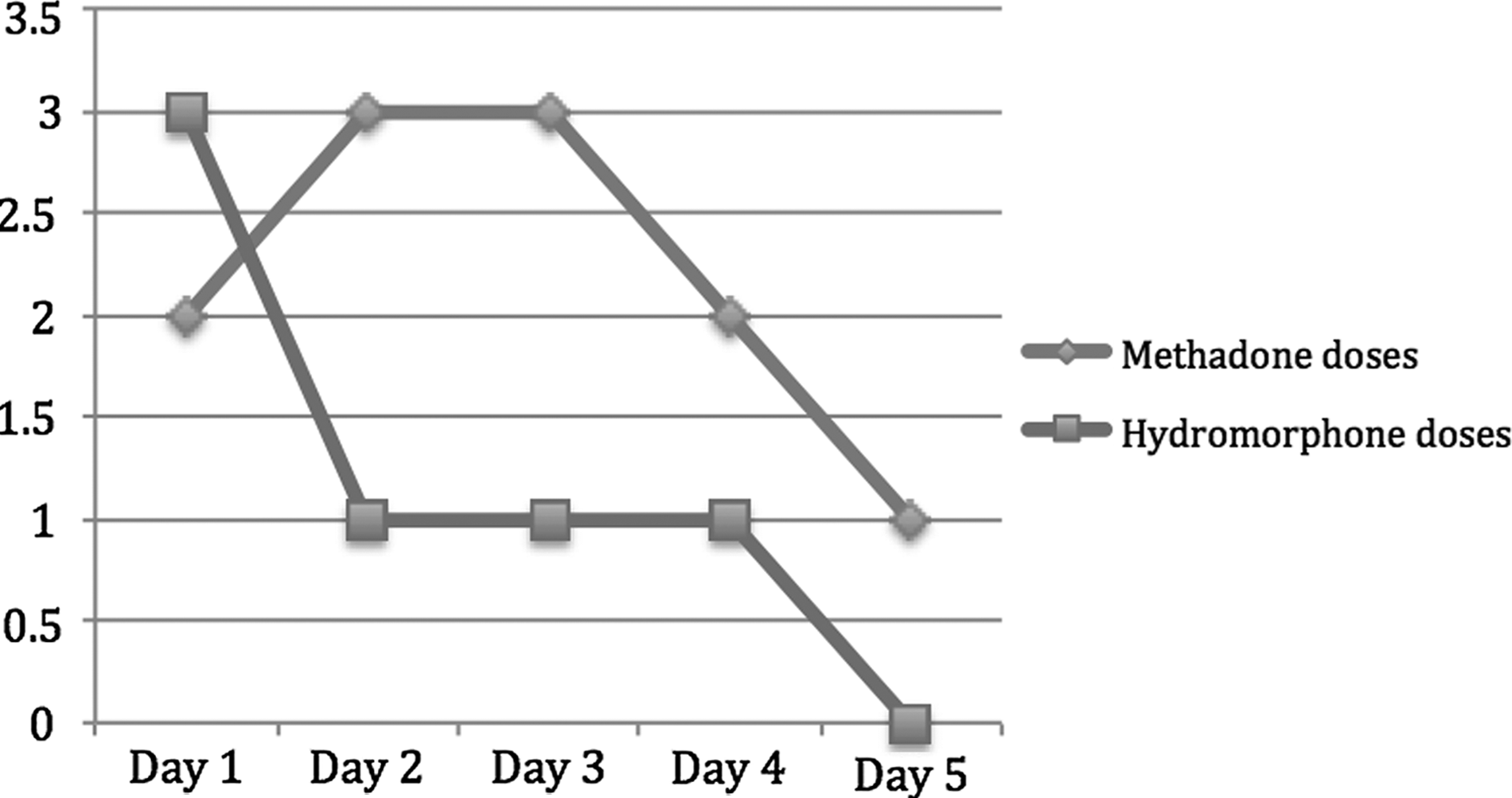
Reduction in methadone breakthrough requirements with time.
Note: Due to drowsiness, the methadone dose was reduced to 10mg on day two
MEDD, morphine equivalent daily dose.
PRN, pro re nata.
On day 6 she was commenced on regular methadone 5mg twice daily, which was then increased to 10mg twice daily. She had good pain control and infrequent breakthrough doses for the remainder of her life. However, she did require a dose reduction because of mild toxicity that was driven by a urinary tract infection. Towards the end of her life when she was no longer able to tolerate oral methadone, the route was changed to a continuous subcutaneous infusion using a 1:1 conversion of oral to subcutaneous methadone.
Case 2
A 67-year-old man with a diagnosis of prostate cancer complained of severe fleeting pain mostly involving his right upper limb, right hip, and mid spine. He had extensive skeletal metastasis to bone with a documented pathological fracture of T10. This man was previously treated with taxotere chemotherapy and received radiotherapy to his right upper limb. Six weeks prior to presentation he was rotated from sustained release oxycodone to transdermal fentanyl at a dose of 150mcg/hr. For breakthrough pain he used transmucosal fentanyl 800mcg and continued to use immediate release oxycodone 20mg. He remained in pain despite also being treated with pregabalin 150mg twice a day, receiving monthly bisphosphonate infusions and trying nonpharmacological approaches such as TENS (Transcutaneous Electrical Nerve Stimulation) and heat packs. This patient reported taking between six and eight breakthrough doses of transmucosal fentanyl and approximately one breakthrough dose of immediate release oxycodone per day. In view of his suboptimal pain control, a decision was made to admit him to a specialist palliative inpatient unit and convert his regular opioid to oral methadone (see Table 3).
Note: For accuracy, we included the PRN transmucosal fentanyl and oxycodone in the calculation.
MEDD, morphine equivalent daily dose; PRN, pro re nata.
On day 6 he was converted to regular methadone 20mg twice daily and 6mg PRN. At this point we discontinued his immediate release oxycodone and continued with transmucosal fentanyl, as he favored this in managing incident pain. He was observed in hospital for five days and remained well controlled with no signs of toxicity. After discharge his methadone was gradually increased over three weeks and maintained at 40mg twice daily. Over this period he was found to have rapidly progressive disease and required further radiotherapy to his right upper limb. This patient also had significant psychological distress related to coping with the progressive nature of his disease that made management of his pain extremely challenging.
Discussion
Methadone's incomplete cross-tolerance to opioids means that there can be a significant reduction in dose when switching to methadone. 11 In both cases above, the final oral methadone dose was much lower than that predicted by the conversion method. This was evident whether there was a recent dose escalation of the previous opioid (case 1) or when the dose had not significantly changed (case 2). Some authors suggest that in situations such as the former, the dose prior to the rapid dose escalation should be used for the conversion.3,12 We used the Morley-Makin method for the conversions, which as described, involves a PRN stop and go approach with a methadone limit of 30mg, and modified it by reducing the dose by one-third in view of the history of opioid toxicity. Discontinuing all of a patient's opioid can be daunting, especially if the opioid doses are very high. Both our patients tolerated the switches using the stop and go strategy similar to studies by previous authors.7,13,14 A recent Norwegian randomized phase II trial comparing patients switched by a stop and go strategy to those switched by a three-day switch reported that the former had a trend of more pain, serious adverse effects, and more dropouts. 15 Two patients died in the stop and go group, one from a myocardial infarction and the other from cardiac tamponade and pulmonary embolism. Based on these findings, the authors concluded that in seriously ill patients requiring large opioid doses, the stop and go method should not replace the three-day switch. It is important, however, to note that the stop and go switching procedure used in this trial involved replacing the previous opioid with an equianalgesic dose of methadone on day one and switched patients over a three-day period followed by observation and titration.
MEDD, morphine equivalent daily dose.
Several authors have published morphine:methadone equianalgesic ratios.16–18 These range from 3:1 to 20:1 depending on the dose of morphine as shown in Table 6. All of these reports confirm a significant association between the MEDD and MEDD:methadone ratio. In a review of 100 outpatient methadone rotations, Parsons and colleagues found that greater MEDD:methadone ratios were associated with older age and higher previous opioid doses. 19 Another possible reason for the variation in these ratios is the indication for rotation. Patients who require rotation because of uncontrolled pain may have a different ratio compared to those who are rotated because of opioid induced neurotoxicity.6,13,19 The reasons for rotation in our patients were uncontrolled pain and toxicity in case 1 and uncontrolled pain alone in case 2. The predicted final dose ratio (morphine equivalent dose 300mg for case 1 and 810mg for case 2) was approximately 10:1 for case 1 and 15:1 for case 2 (Ayonrinde). 18 The actual intial ratios were 30:1 and 20:1 and the final ratios were 15:1 and 10:1 for cases 1 and 2, respectively. These cases illustrate the difficulty in predicting final doses from standard equianalgesic tables.
Adapted from Pollock, et al. 16
Morphine dose in mg/day.
Conclusion
Methadone is an effective medication for both nociceptive and neuropathic pain. It has variable pharmacokinetics and a long half-life and is therefore not recommended as a first-line agent. In cases where cancer patients fail to respond or develop tolerance to opioids, conversion to methadone is a reasonable approach. Although equianalgesic tables may not always predict final methadone doses, when properly selected they can be useful tools for the experienced clinician when treating patients in both inpatient and outpatient settings. Otherwise using a stepwise conversion as described in the methods above should provide the desired therapeutic effect. A hasty opioid rotation based on recognized ratios would have resulted in potentially serious toxicity in our cases. A customized and cautious approach is thus advisable when rotating to oral methadone, especially in patients who have experienced opioid toxicity, and this is perhaps more important than the switching method used. Certainly the benefits of using methadone in patients with severe cancer pain far outweigh the risks.
Author Disclosure Statement
No competing financial interests exist.