
Abstract

Dear Editor:
Introduction
The integration of palliative medicine into the care of patients with chronic incurable diseases requires major changes in the structure and processes of health care delivery.1,2 These changes can only take place when there is effective collaboration among different health care professionals involved in the care of these patients. Unfortunately, there are few opportunities for health care professionals to freely express the perspectives of each of their areas of expertise and explore together ways in which they can successfully interact in developing palliative care.
The conference “Cure palliative prima: ma come?” (Early palliative care: how?) was held on May 14, 2012, at the Castle in Bentivoglio, a small village near Bologna where the Academy of the Sciences of Palliative Care is based. Many Italian representatives of palliative care in oncology and other fields as well as famous oncologists were present. The issues debated in the conference are topics for the creation of a consensus document on early palliative and continuing care. We believe that the findings and conclusions of this conference may be helpful to colleagues from other regions in Europe and in the rest of the world who are interested in the development of integrated palliative care programs.
The Conference: Summary of the Main Lectures and Position Statements
Session I: Clinical aspects and expertise
The session started with a critical analysis of the scientific evidence encouraging early palliative care for patients with advanced cancer who have a poor prognosis. The second part of this session focused on the disciplinary settings and possible psychological implications of interacting simultaneously with the patient and his or her family.
Speaking from the point of view of the palliative care physician, Adriana Turriziani, president of the Società Italiana di Cure Palliative (SICP), discussed that a palliative care physician should be a specialist with a specific education and skills in palliative care. The palliative care specialist should know how to care for and manage the terminally ill patient and his or her family; evaluate and manage pain and physical symptoms; evaluate and manage related psychosocial and spiritual issues; communicate openly; manage end-of-life care, including support and bereavement for the family; provide continuity of care and close collaboration with other professionals involved with the care of the patient, fulfilling all of the needs arising from the evolution of a disease with poor prognosis; and search for integration between his or her expertise and the patient's needs during the progression of the disease.
The role of the medical oncologist was summarized by Vitorina Zagonel, coordinator of the Associazione Italiana di Oncologia Medica (AIOM) Continuum of Care in Oncology working group. It is important that the medical oncologist receive basic training in palliative care to detect, prevent, and treat the main symptoms that can occur during the entire trajectory of the disease. This training guarantees a better quality of life for patients and allows a more gradual transition to palliative therapy in advanced terminal disease.
The psycho-oncologist, according to Anna Costantini, president of the Società Italiana di Psico-Oncologia (SIPO), supports patients and families during the entire trajectory of the disease. The psycho-oncologist also guides professionals during their training in difficult communication and supervises during these conversations with patients and families. Acknowledgment of conscious and unconscious psychological motivations between staff members and patients and families, especially in the setting of advanced disease, is essential. A psycho-oncologist has to understand patients' preferences to conduct supportive and hopeful but realistic conversations about the goals of therapy; using approaches like this can help professionals to avoid burnout and improve their quality of life.
Danila Valenti, responsible for the palliative care network within the local health organization in Bologna, pointed out that a palliative care network can work effectively only by recognizing the different roles of all health care workers committed to this service. The division between the cancer and palliative care cultures is still marked, and there is a need for clarification of expertise and roles, which can lead to acknowledgment of the phases of intervention and professional responsibilities. In palliative care it is fundamental that specialists with different points of view come to consensus to work through improving therapeutic and communication strategies. The risk of confusing the cancer and palliative care domains can lead to distortions, as is noticeable in hospitals where palliative care culture has not been established yet. In these hospitals that lack a continuous care service, terminally ill patients fail to receive appropriate clinical management and so often receive treatments that are useless, expensive, and harmful.
The role of the university, as explored by Gianluigi Cetto, oncologist at the University of Verona, should be to guarantee homogeneity in the education and examination of health workers committed to palliative care. At present, a wide variety of disciplines, even within the Italian Academy, are related to palliative care; this variety reflects a lack of homogeneity, which also exists internationally. Palliative care culture can gain strength and establish ground within the clinical medicine arena only if its professionals are well trained, with specific skills. All medical schools should have educational programs covering palliative care for undergraduates.
Session II: Organizing models, roles, and cost of care
Giovanni Zaninetta, past president of the SICP, pointed out that a useful organizational structure for the definition of roles and expertise in palliative care is based on inpatient residential settings, such as hospices, which also deliver palliative care at home. Residential settings are expensive but necessary, for example, when the family is not present or control of symptoms is unsatisfactory.
Raffaella Pannuti, president of the Fondazione Antitalia Onlus (ANT), and Giancarlo Furlò, representing the Associazione Nelson Frigatti, emphasized that the functions of home care organizations such as ANT and the Associazione Nelson Frigatti naturally extend from the beginning to the end of an incurable disease. The practitioner can guarantee continuous care. Home care professionals must be skilled in both symptom treatment and palliative care delivery. Home palliative care should be integrated with the other components of the palliative care network, that is hospital and hospice.
Angelo Martoni, medical oncologist at the Policlinico S. Orsola-Malpighi in Bologna, discussed the Migliorare l'Appropriatezza di Uso della Terapia Antitumorale e l'Integrazione tra Oncologia Medica e Cure Palliative nei Pazienti Oncologici in Fase Avanzata con Attesa di Vita Breve (MIRTO) project (Improving the Appropriate Use of Cancer Treatments and the Integration between Medical Oncology and Palliative Care in Patients with Advanced Cancer at the End of Life), which is directed at multidisciplinary simultaneous assessments of the course of the cancer patient. This intervention is the basis for the standards necessary to gain European Society of Medical Oncology (ESMO) acknowledgement of medical oncology units as palliative care centers, said Carlo Barone, oncologist at the Università Cattolica del Sacro Cuore in Rome. Vittorio Franciosi, medical oncologist at the University-Hospital in Parma, presented a survey on the different types of integration models operating in Italian ESMO-designated cancer centers. Preliminary results showed that the “integrated care” model operated in 75% of centers, but approaches for integration depended to a large extent on local factors.
Finally, Rita Maria Melotti, professor of anesthesia at the University of Bologna and member of the National Board for Palliative Care and Pain Treatment, explained the significance of Law 38, recently passed in Italy, which calls for organization of palliative care and pain treatment centers and distinguishes palliative care for adults versus that for children. It also identifies the need for early palliative care in an integrated, recognized, and operating setting (see Table 1).
Focusing the issues
To properly develop a palliative care delivery system integrated with the active treatment of a disease with poor diagnosis, it seems necessary to solve some aspects leading to confusion (see Table 2).
One of the main issues is to identify when a specialist should stop active treatments and care for the patient's quality of life only.
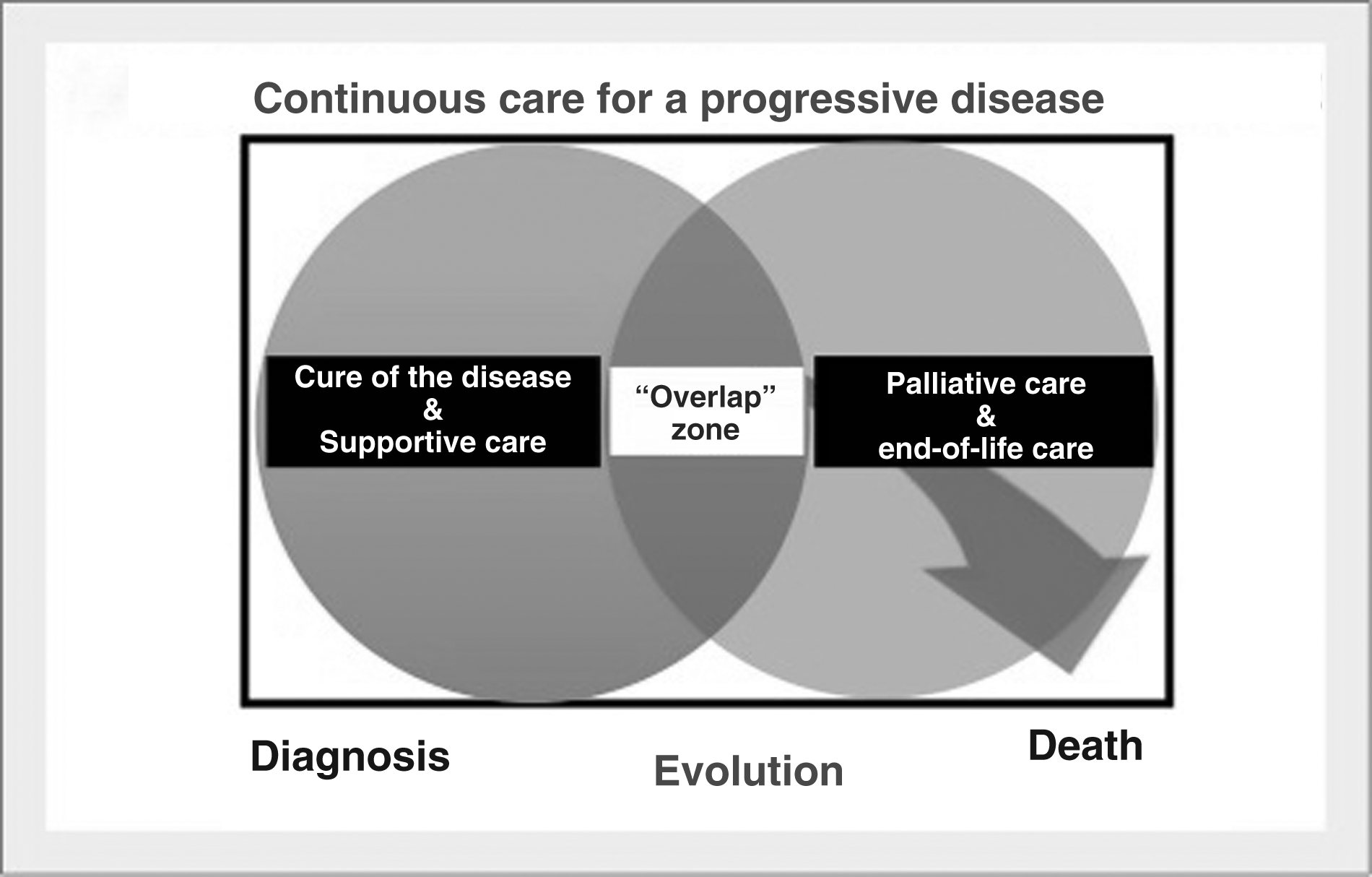
The difficulty for the physician who has been caring for the patient up to that time lies in his or her ability to find the right words to explain the shift in strategy and, at the same time, abandon the specialist treatment of the disease to start an end-of-life treatment course. To recognize the appropriate moment, the specialist must set a limit; to do this, the specialist needs to be aware of palliative care issues. Being aware consists of practicing to ensure care for the terminally ill patient until the end (Fig. 1). Being unaware implies a lack of palliative care, a belief that palliative care is unnecessary, and ignorance of the existence and activity of several palliative care organizations.3,4

The need for palliative care increases with the progression of a degenerative disease (not only cancer).
In both cases, the lack of a sense of limit leads to bad management of the end of life, which results in overtreatment—often delivered as a consequence of a poor capacity to communicate and bad symptom management, which should focus first of all on the management of the patient's pain and the family. 5 Recently some articles have examined the opportunity to act early in the management of patients with cancer with a poor prognosis to help create an easier transition into palliative care while active treatment is still being delivered. 6
It is clear that the concept of delivering palliative care early, at the diagnosis of an incurable disease or soon after, clashes with the natural history of the disease. 7 Therefore, the question of when to deliver palliative care also involves determining the prognosis of an incurable disease with possible treatment. There are several prognostic or validity scores available with distinctive features and limits. These rates are generally used to determine the best therapeutic strategy. 8 However, there is an opportunity to apply one of these rates to identify the moment when it is appropriate to start thinking about starting a palliative care program. This process has not been done yet, because it would be necessary to first develop integration between teams with different tasks (treatment and care) using objective dimensions that can be evaluated in studies (Fig. 2).9,10
Continuous care is guaranteed by a phase during which the disease specialty team and the palliative care team work together. The size of the “overlap” between specialty treatment and palliative care is determined by (1) therapeutic changes of the disease, (2) performance status of the patient, (3) preference of the patient and family after comprehensive discussion, and (4) costs and availability of a competent palliative care team. EOL, end of life.
Team composition, feasibility, and costs
The feasibility of a palliative care program integrated with an active treatment program is related to the characteristics of the health and social service setting in which the project of integration develops. The costs of the program are also related to the team composition. Several studies have shown that a palliative care team within a general hospital or cancer center promotes savings because of the reduction in the number of both useless diagnostic and therapeutic exams and the duration of the patient's stay in hospital. Differences in team composition are seen all over the world by choice or necessity. The composition and role of a palliative care team inside and outside the hospital potentially integrated with the active treatment team to create a continuous care service are still to be defined.11,12 Without well-defined roles and structures, palliative care teams do not yet have the authority to impose their specific care plan in the course of the disease. But can the potential savings offered by a palliative care team be modified by its early inclusion in the course of treatment of an incurable patient?
Different health systems in different countries
Different health systems do not always allow a homogeneous assessment of costs and saving. The lack of homogeneity of the research models and methods in this field make comparison among the different studies in the literature more difficult. The issue requires pragmatic prospective studies that take into account the different cultural backgrounds in addition to the economic and structural differences of the different settings.13–15 If the rationale for an integrated program starting at the early stages of an incurable disease clashes with an inability to demonstrate cost reduction, then the future potential of the program is scarcely sustainable. In a recent article, Temel and colleagues 16 argued that the savings associated with starting palliative care early are the result of suspending ineffective treatments. However, the cost analysis seems to be more of a hypothesis than documented evidence. Not all therapies have the same economic impact nor does every team. 16 Discussion with disease specialists has lacked a pragmatic examination of the effectiveness and costs of palliative care provision models, even if they were adjusted to different social and cultural backgrounds.
Terminology
A commonly shared terminology has not yet developed in the palliative care field. Expressions such as “supportive care,” “palliative medicine,” and “end-of-life care” are often used synonymously, and this can lead to confusion when different studies and experiences are compared. The message given to colleagues outside our field is confusing, and this weakens the “palliative movement.”17–20
In particular, “supportive care” should indicate every treatment delivered during the active treatment of the disease. In oncology, supportive care should be delivered to control the symptoms related to the disease and its therapeutic treatment (e.g., vomiting caused by chemotherapy, hydration, diarrhea control). During this phase it is possible to also deliver the more specific treatments of palliative care (e.g., psychological support to the patient and his or her family, pain control).
On the other hand, the World Health Organization (WHO) definition of palliative care seems to exclude the delivery of palliative care when the disease is still curable. 21 The WHO definition has been accepted because it defines the context of the treatment delivery. Under this definition we could not use the term palliative care for treatments that are delivered during the active treatment of an incurable disease. Consistent with this definition, the Multinational Association of Supportive Care in Cancer (MASCC) approaches the issue of supportive care as not related to palliative care in its strictest definition but recognizes palliation where the supportive care is delivered.
Expertise definition and training
In the United Kingdom, the United States, and Canada, which have been developing palliative cultures and organizations for a long time through educational and training programs, palliative care is a subspecialty of medical oncology. In other words, a wide knowledge of medical oncology is required of those interested in practicing palliative care in oncology. By getting specific training, the oncologist–palliative care specialist can understand the problems of the patient with cancer, because he or she knows the disease history and can interpret the limits of the patient's specific cancer treatments.1,22,23
In Italy, a recently passed law regulates the organization of palliative care and pain treatment centers. 24 This law has resulted in a training program initiative (master's degree) reserved in part for physicians who have specialized in medical oncology, geriatrics, neurology, pediatrics, anesthesia, or radiation therapy. The Italian Council itself is considering the possibility of including a palliative care course in the medical sciences degree program. This provision is important, because a real palliative care culture can be achieved only by starting from the roots of physician education.
Natural history of the disease
Palliative care began and has developed mainly in oncology. But in the future it is desirable to expand the care to other incurable diseases. It will be necessary then to select the areas of palliative care intervention based on the setting of patients and diseases. A more or less integrated palliative program for children would be different from that for adults; and such care for the elderly would differ from that for young adults, in the same way that treatment for a patient with amyotrophic lateral sclerosis is different from that for a patient with incurable cancer or heart failure. We therefore are faced with a scenario that requires pragmatism and clear and comparable definitions of the diseases.
Conclusions: Toward a Consensus
This conference has been a great opportunity to document a consensus point of view among different health care professionals in palliative care. Everybody recognized that psychological and physical assessment throughout the trajectory of the disease is now possible and that there is a common body of knowledge in palliative care with validated tools, and we can know the pathophysiology of the patients' illness. Different professionals with their expertise were present, and it is necessary that they work together inside the available structures we already have (i.e, hospitals, hospices, home care).2,25,26
However, there is still a lack of clarity about some issues. The delivery of palliative care needs a highly flexible model to adapt to different resources in different countries. For this, a consensus in interdisciplinary care is required. We need only the good will to develop processes that comply with the rules and disciplinary roles of the different actors in this field of medicine, which still needs to establish itself permanently. Consensus in the medical and scientific community can greatly contribute to the affirmation of palliative care.
Meetings like this one are important to identify barriers, challenges, and opportunities for care in the palliative setting. We hope this document can help other teams focus the dialogue in the development of palliative care.
Footnotes
Acknowledgments
Adriana Turriziani, president of SICP, the Italian Society for Palliative Care
Vitorina Zagonel, chairman of the cancer continuous care working team of the AIOM
Anna Costantini, president of the SIPO
Danila Valenti, responsible for the Palliative Care Network within the local Health Organization in Bologna
Gianluigi Cetto, oncologist at the University of Verona
Giovanni Zaninetta, past president of the SICP
Raffaella Pannuti, president of the ANT, the National Tumor Association Foundation in Italy
Giancarlo Furlo representing the Nelson Frigatti Association
Angelo Martoni, medical oncologist at the S. Orsola-Malpighi Hospital in Bologna; MIRTO project (Improving the Appropriate Use of Cancer Treatments and the Integration between Medical Oncology and Palliative Care in Patients with Advanced Cancer at the End of Life)
Carlo Barone, oncologist at the Università Cattolica del Sacro Cuore in Rome
Vittorio Franciosi, representative of the European Society of Medical Oncology (ESMO) Centers in Italy
Rita Maria Melotti, professor of Anesthesia at the University of Bologna and member of the National Board for Palliative Care and Pain Treatment