
Abstract
Abstract
Background:
Episodic breathlessness is a common and distressing symptom in advanced cancer and nonmalignant diseases but there is a lack of evidence on the characteristics of the symptom.
Objective:
The aim of this study was to determine the duration, severity, frequency and timing of breathlessness episodes in patients with advanced diseases.
Methods:
Explorative analysis of pooled cross-sectional data on episodic breathlessness collected in personal interviews with patients suffering from chronic obstructive pulmonary disease, lung cancer, chronic heart failure, or motor neuron disease. Interviews were conducted as part of two studies in the UK and in Germany that included the same questions on duration, frequency, timing, and peak severity of breathlessness episodes. Severity was measured on the modified Borg scale (0–10).
Results:
One hundred and twenty-nine patients, 61% male, mean age of 67 years (SD 9.8), were included. The episodes described were mainly short (75%≤10 min), severe (mean 6.5 (SD 2.4), and occurred mostly daily. Frequency of episodes triggered by exertion could hardly be determined as these varied depending on patients' activity.
Conclusion:
Our study reveals clinically important information on the characteristics of episodic breathlessness in patients with advanced diseases. Findings have implications for the treatment of episodic breathlessness since most short-acting drugs in use have a longer onset of action compared to the duration of episodes. We need to determine patient-relevant therapeutic targets for future evaluation of adequate pharmacological and nonpharmacological management options that are urgently warranted.
Introduction
Methods
This is a planned explorative subanalysis of pooled crosssectional data that were prospectively collected within two studies. The overall aim is to describe the experiences and characteristics of (episodic) breathlessness in patients with advanced disease. The first study was a longitudinal study assessing patients with LC and COPD in Germany in order to describe the course of breathlessness, other symptoms, distress, and palliative care needs over a period of 12 months. Baseline data, including demographic and clinical data, were obtained in personal interviews followed by monthly telephone interviews. Participants were recruited in two inpatient units and two outpatient clinics in Oldenburg, Germany, from February 2010 to April 2011. The study was supported by the German Federal Ministry of Education and Research. Baseline data about the characteristics of episodic breathlessness were used in our analysis.
The second study was a mixed method, crosssectional study examining patients with LC, COPD, CHF and MND in the United Kingdom in order to explore the experience of episodic breathlessness. Participants were recruited in five outpatient clinics of two university hospitals in South London in 2010. Further results of the qualitative part of the second study and the description of methods in more detail have been published elsewhere.7,9
Research ethics board approvals have been obtained from the Joint UCL/UCLH Committees on the Ethics of Human Research Alpha (09/H0715/81) in the United Kingdom and the State Medical Chamber of Lower Saxony (Bo/20/2009) in Germany.
Both studies used the same method to obtain data, including the same inclusion and exclusion criteria of participants. Participants needed to be breathless (irrespective the level of severity), ≥18 years, without cognitive impairment and with advanced diseases defined as follows:
• LC: primary lung cancer at any stage, cancer of any origin with lung metastases; • COPD: stage III or IV of the Global Initiative for Obstructive Lung Disease classification; • CHF: stage II to IV of chronic heart failure according to the New York Heart Association classification; • MND: all participants with chronic obstructive pulmonary disease suffering from breathlessness.
Herein, we report on the data collected from participants suffering from episodic breathlessness. Episodic breathlessness was defined as “a clinically significant aggravation of dyspnea in patients with continuous dyspnea or occurring intermittently.” 5
Patients were assessed by personal interviews in both studies using the same questions regarding episodic breathlessness. First, the peak severity of breathlessness episodes, that is the maximum severity level of a typical episode as experienced by the patient, was assessed by the modified Borg Scale (0–10). 10 Second, patients were asked to quantify the duration (in seconds, minutes, or hours) and the frequency (per day, per week, or per month) of their episodes. Third, patients were asked to state the timing of their episodes (at night, during the day, or both). Finally, we asked whether patients experienced breathlessness episodes on exertion and/or at rest. In addition to that, functional performance (Karnofsky Performance Status Scale) and severity of breathlessness in general (over the last 24 hours) were assessed (modified Borg scale [0–10]). 10
We used descriptive analysis only because of the explorative approach of data collection (mean, standard deviation [SD], median, range, numbers and percentages [%]). Categories were built post hoc for the characteristics duration and frequency according to the episodes described as some patients could only determine a range rather than a number. Differences between the four underlying diseases were tested using ANOVA for peak severity and Chi-square test for duration (≤or>10 minutes) and frequency (≥or<daily) of episodes (α=0.05). The decision for cut-offs (10 minutes and daily) was based on the findings of Reddy et al. and on clinical relevance. 5 Some patients reported different manifestations of episodes (e.g., more severe or less severe; at rest or at exertion) which we counted separately in order to consider all relevant information. Therefore, the unit of analysis was episodes of breathlessness rather than patients.
Results
In total, 129 patients (COPD 61, LC 46, CHF 14, MND 8), 79 (61%) male, with a mean age of 67 (SD 9.8; range 39–92) were included. Patient characteristics are summarized in Table 1. All patients experienced episodic breathlessness on exertion, 44 (34%) experienced episodes also at rest and 74 (57%) patients reported continuous breathlessness in addition.
Missing data=4.
The characteristics and numbers of breathlessness episodes described by the patients are presented in Table 2. More than 75% of the episodes were described to last ten minutes or less (fig.1). Forty patients reported different manifestations of episodes and these were assessed and counted separately. Therefore, the total number of episodes (n) is higher than the number of patients. The number varies between each characteristic because some patients could not describe each of these for their episodes.
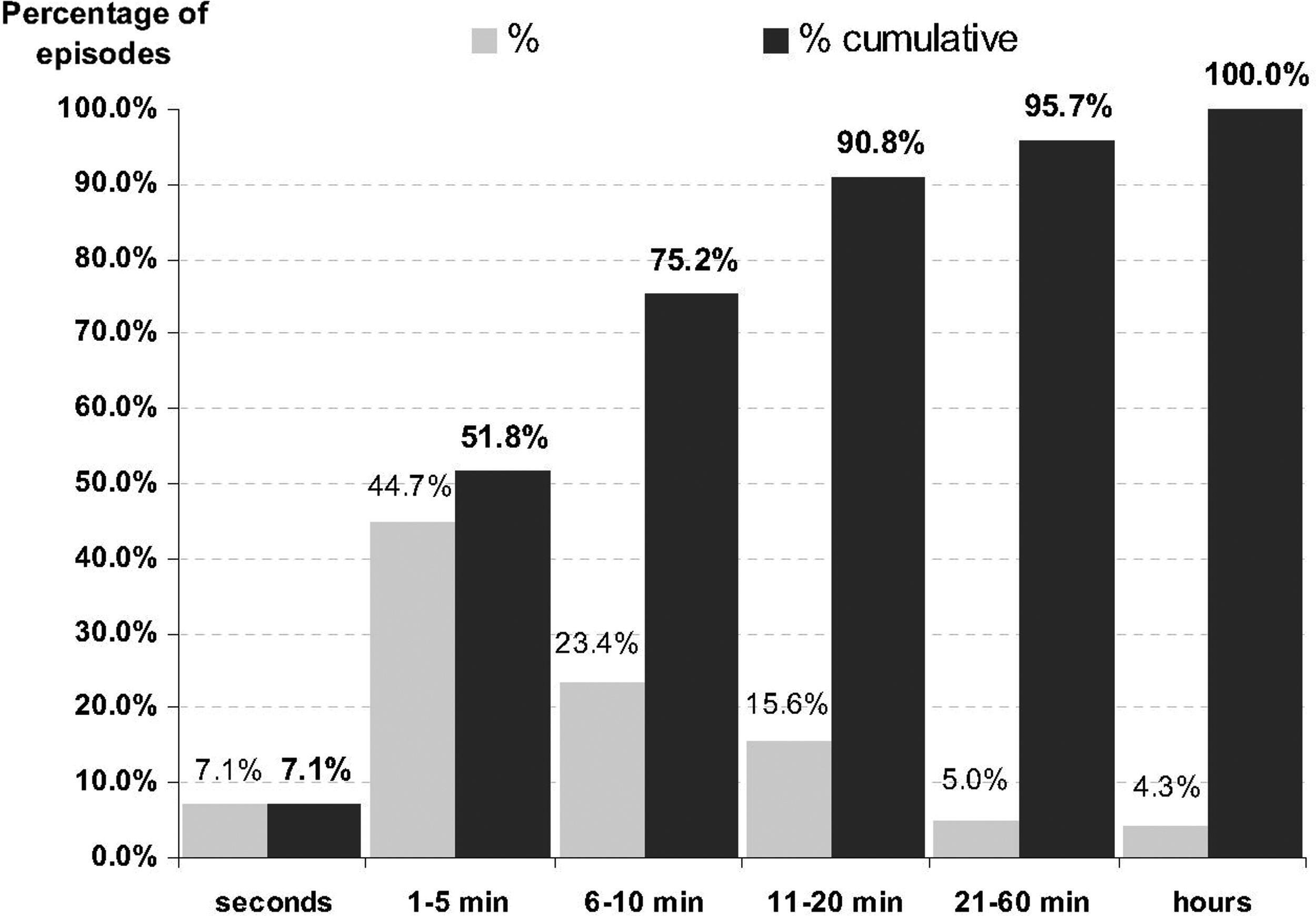
Duration of the breathlessness episodes described by the patients.
Total number of episodes was higher than number of patients, because 40 patients experienced different manifestations of episodes, and characteristics were assessed for each, separately. In addition, few patients described each characteristic of their episodes and, thus, total numbers of episodes vary per characteristic.
For additional six episodes, patients could not report numbers but ranged the duration as follows: seconds (1), minutes (4), hours (1).
The low number of episodes relates to the difficulty of most patients to determine the frequency of a triggered episode (e.g., by exertion) as “it depends what I am doing.”
NA, not applicable
There were no statistically significant differences in characteristics between the four underlying diseases (see Table 3).
ANOVA was performed to test differences in mean between the four disease groups.
Chi-square test was used to test for differences in duration between the four disease groups (≤or>10 minutes).
Fisher's exact test was used to test for differences between the four disease groups (≥or<daily).
COPD, chronic obstructive pulmonary disease; LC, lung cancer; CHF, chronic heart failure; MND, motor neuron disease
Discussion
This is the first study on the characteristics of episodic breathlessness including patients with different underlying diseases. Our results suggest that breathlessness episodes are short (75% ≤10 min), severe, and occur daily. The majority of patients could not exactly determine the frequency of episodes, because they varied depending on patients' activity.
Considering these findings, breathlessness episodes show some similar characteristics to breakthrough pain, e.g., high severity and frequency. However, breathlessness episodes seem to differ in a shorter duration since a median duration of 60 minutes is reported for episodes of breakthrough pain—compared to one to five minutes in our study for episodic breathlessness. 11
Implications for Clinical Practice and Future Research
Our results on the short duration of breathlessness episodes suggest that patients tend to recover quickly from episodes. The results are supported by a recent study on recovery time of exercise induced breathlessness in patients with thoracic cancer that found a median duration of four minutes. 12 These findings have important implications for the management of episodic breathlessness as the onset of action of immediate release morphine, the standard treatment and only drug group with evidence for the symptomatic relief of breathlessness, takes 20–30 minutes and thus may be inappropriate for these short-lasting episodes.13,14 Fast-acting drugs (e.g., fentanyl) are now available and used for pain episodes but effectiveness in breathlessness is unknown. 15 Furthermore, nonpharmacological strategies (e.g., panic control techniques, distraction, or hand-held fan) that are patient-led, supportive of patients, and accessible at any time might be more appropriate but need specification and evaluation for episodic breathlessness.
Patient-relevant therapeutic targets have to be identified by patients and experts: Do we need to reduce peak severity or frequency? Does the duration of recovery time have impact for the patient? The identified relevant targets should serve as primary outcomes in future clinical trials that aim to improve symptom management. These questions are planned to be addressed in an ongoing research framework, with the overall aim ito advance the understanding and management of this distressing symptom. As part of this plan, an international consensus on a definition and categorization of the symptom has been reached and will be published soon. 16
The explorative design limits the generalization of our results and the use of statistical tests for difference, because no sample size was calculated beforehand and the categories tested were built post hoc. Therefore, the results of the tests need to be interpreted with caution.
Conclusions
Our study reveals a first picture of and clinically important information on the characteristics of breathlessness episodes in patients with advanced disease. Findings should be confirmed by a fully powered survey with larger subsamples than in our study. In order to reduce occurrence, severity, and burden of episodic breathlessness in patients with advanced disease, clinical trials are urgently warranted to evaluate adequate pharmacological and nonpharmacological interventions. For this, patient-relevant therapeutic targets need be identified and adequate endpoints should be developed in order to conduct well-designed clinical trials that aim at improving symptom management.
Footnotes
Acknowledgments
The authors would like to thank Hamid Benalia, Verena Gerdes, Nicole Sowinsky, and Birgit Kannenberg-Otremba for their support of this study.
Author Disclosure Statement
This study was presented as a poster presentation in 2012 at the 9th Congress of the German Association for Palliative Medicine, Berlin, Germany.
Steffen Simon and Rau Voltz received research funding for a clinical trial from TEVA Ltd., after this study was conducted. All of the other authors declare that no conflicting financial interests exist.
Funding
This study was supported by a research grant from the Dr. Werner Jackstädt Foundation, Wuppertal, Germany, the Cicely Saunders Institute, King's College London, London, United Kingdom, and the German Federal Ministry of Research of Education and Research (grant number BMBF 16KT0951) without any influence on study design, analysis, interpretation, or presentation.