
Abstract
Abstract
Background:
Little is known about the determining factors related to the administration of continuous palliative sedation. Knowledge of these determinants may assist physicians in identifying patients who are at high risk of developing refractory symptoms, enable physicians to inform patients, and optimize close monitoring.
Objective:
The aim of this systematic review was to identify determinants of the administration of continuous palliative sedation.
Design:
A systematic review of PubMed, EMBASE, and CINAHL was performed to identify English, Dutch, and German language papers published from January 1990 through April 2011. Inclusion was based on the following criteria: patient-based research on continuous palliative sedation, studies investigating determinants of palliative sedation and/or comparison between sedated and nonsedated cohorts, and studies using multivariate analyses and of fair to good or good methodological quality.
Results:
In total, eight papers were reviewed. The following nine factors were found to be associated with the administration of continuous palliative sedation: younger age, male sex, having cancer, feelings of hopelessness, dying in a hospital, living in a Dutch speaking community setting, very nonreligious or extremely nonreligious physicians, physicians working in “other hospital” specialties, and physicians in favor of assisted death.
Conclusions:
Given the variation in study designs and the limitations of the included studies, the outcomes should be interpreted carefully. Further research is needed, particularly regarding factors that can be influenced and that may alter the course of a patient's symptoms and the patient's eventual need for palliative sedation.
Introduction
P
Over the past decade there has been considerable discussion concerning the terminology for and definition of palliative sedation. Current definitions include the following similarities: (1) pharmacological agents used to reduce consciousness, (2) reserved for the treatment of intolerable and refractory symptoms, and (3) only considered in a patient who has been diagnosed with an advanced progressive illness.3–8 The term “palliative sedation” refers to distinct types of interventions: brief or intermittent sedation or continuous sedation administered until death. 3 Continuous palliative sedation may be superficial or deep. In the latter, there is a complete loss of the ability to communicate. The degree of symptom control rather than the degree to which consciousness must be reduced determines the dose, combination, and duration of the drugs administered. 3 Over the past 10 years, continuous palliative sedation has been the subject of considerable debate in the field of palliative care. Questions have arisen as to whether palliative sedation is a euphemism for euthanasia and about where to draw the boundary between sedation for refractory symptoms that are primarily physical and sedation that includes existential suffering.9–13 Currently, continuous palliative sedation, if correctly applied, is increasingly accepted as a part of medical practice. 4 The frequency of palliative sedation has been reported to range from 2.5% to 64% among terminally ill patients.14,15 This wide range likely reflects variations in the definition of the term and differences in culture and clinical settings.
Although continuous palliative sedation is not an uncommon end-of-life intervention, little is known regarding the possible determinants of this intervention. A determinant is an element that identifies or determines the nature of something or that fixes or conditions an outcome. 16 Knowing the determinants of continuous palliative sedation could help physicians to better identify patients who are at high risk of developing refractory symptoms and thus optimize the use of close monitoring. Such strategies would allow physicians to respond to a patient's symptoms earlier and to potentially prevent a refractory state of such symptoms, thereby possibly limiting the future need for continuous palliative sedation. Moreover, in acute situations there is often insufficient time to make well-informed, balanced decisions concerning palliative interventions. Thus, the physician must proactively develop a comprehensive care plan and establish end-of-life interventions that will meet the patient's goals, values, needs, and preferences. This planning will enhance the patient's autonomy and inform the patient or the patient's representative about the indication and preconditions for continuous palliative sedation.17,18 The objective of this study was to perform a systematic review of published literature to identify possible determinants of the administration of continuous palliative sedation.
Methods
Data sources and search strategy
For this review we searched all articles written in English, Dutch, and German and published from January 1990 through April 2011. A computerized search was performed in PubMed, EMBASE, and CINAHL. The following search terms and combinations were used: (determinant* OR predict* OR correlat* OR characteristic* OR compar* OR associat* OR probability OR survival OR (life AND expectancy)) AND ((palliative AND sedation) OR (terminal AND sedation) OR (sedation AND for AND terminally AND ill AND patients) OR (end AND of AND life AND sedation) OR (continuous AND palliative AND sedation)).
Study selection
To create an initial list of potential studies, the first reviewer (RvD) excluded all studies that reported on the following: (1) patients who were admitted to an intensive care unit; (2) palliative sedation that was restricted to children; (3) sedation therapy for invasive procedures and operations; (4) sedation therapy in animals; and (5) medication administered at low doses to relieve insomnia and/or dyspnea or sedation as an unintended side effect of medication. Subsequently, two reviewers (RvD and JH) independently screened all abstracts that were retrieved, and these two reviewers then applied the following two inclusion criteria:
1. The paper had to report on patient-based research on continuous palliative sedation. 2. The paper had to report on determinants (or terms such as “associations” and “predictors”) of palliative sedation or on a cohort study on sedated and nonsedated patients in a palliative trajectory.
The two reviewers then compared their lists of selected abstracts to reach a consensus. In cases in which there was doubt concerning the inclusion of an article, the full-text article was retrieved. A final list of selected papers was compiled after retrieving the full-text articles that met the inclusion criteria. These papers were then screened for the presence of multivariate statistical analyses, and the methodological quality of the selected papers was assessed using an assessment tool devised by Hawker and colleagues. 19 Only papers that included multivariate analyses and were of fair to good or good methodological quality were included (see Figure 1).
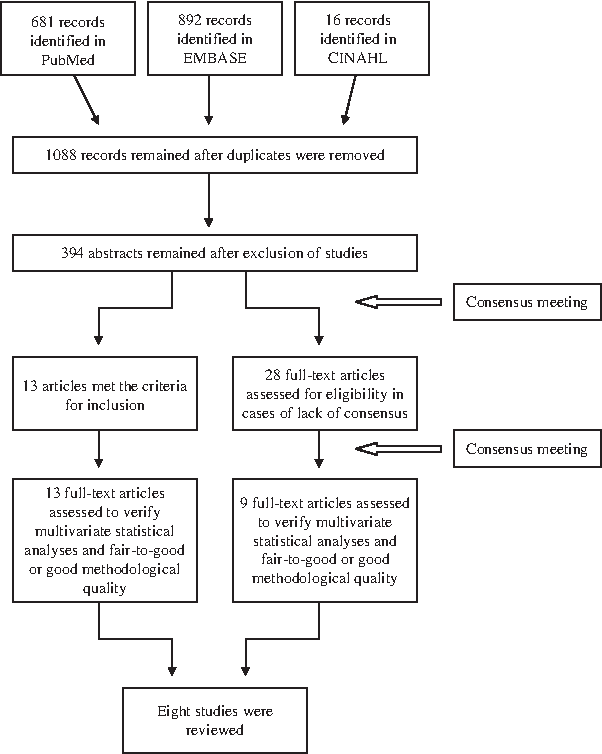
Flow diagram of the studies that were assessed and included.
Data extraction
From each selected paper, the following information was extracted: first author, year of publication, research design (prospective or retrospective), setting, patient diagnosis, specialty of the physician, study population, number of included patients who received palliative sedation, depth of sedation, determinants, and outcomes.
Statistical analysis
Because the study design, setting, participants, and reported determinants varied markedly between the studies, we chose to describe the studies, their results, and their limitations rather than combining or ranking the study data using a meta-analytic statistical approach.
Results
Study selection
The search initially identified a total of 1088 unique papers. After an initial screening of the abstracts, 694 papers were excluded, and 394 were deemed eligible for screening by the two reviewers. For 13 of these papers, the reviewers reached immediate consensus that the papers met the inclusion criteria (see Figure 1). For an additional 28 papers, the full-text articles were screened, and 9 of these papers met the inclusion criteria after a consensus meeting. Finally, after screening for the presence of multivariate analysis and fair to good or good methodological quality, 8 of 22 articles were included.
Study characteristics
All of the included studies used a retrospective design. Of the studies that reported on a clinical setting, all combined the settings of hospital and home (see Table 1). Other settings included nursing homes, hospices, palliative care units, institutions, care homes, and other settings. Nearly all of the studies included cancer and noncancer patients. In half of the studies, the specialty of the attending physician was reported. The number of patients to whom palliative sedation was administered varied from 31 to 1260 (total, 3525 patients). All studies focused on deep palliative sedation. Based on Hawker's method, all of the studies had fair to good methodological quality. 19
All of the studies used a retrospective design.
Maessen and colleagues included only patients with amyotrophic lateral sclerosis. 24 All other studies included cancer and noncancer patients.
In the article, deep sedation was defined as “The patient received drugs, such as barbiturates or benzodiazepines, to keep him/her continuously in deep sedation or coma until death.”
The number was calculated on the basis of the data (the incidence of continuous deep sedation (percentage) and the incidence of end-of-life decisions (number)) in the original article.
The result remained statistically significant in a logistic regression; however, the odds ratios or relative risks were not mentioned in this study.
In the article, deep sedation was defined as “A patient being deeply and continuously sedated or in a coma until death, by means of e.g benzodiazepines or barbiturates.”
In the article, deep sedation was defined as “The administration of drugs to keep the patient in deep sedation or coma until death.”
Only results reporting continuous palliative sedation “with” or “without” nutrition and hydration with the same outcome were included in this review.
The number of patients who received sedation was not reported in this study, so the number was copied from a study by Van den Block et al. 26 that reported on the same cohort.
In the article, deep sedation was defined as “A patient being deeply and continuously sedated or in a coma until death with drugs such as benzodiazepines or barbituates.”
In the article, deep sedation was defined as “A patient is continuously and deeply sedated or kept in a coma before death.”
The number of patients who received sedation was not reported in this study, so the number was copied from a study by Seale et al. 23 that reported on the same cohort.
CI, confidence interval; NA, not applicable; OR, odds ratio; RR, relative risk.
Determinants
The studies analyzed a total of 14 factors (see Table 2). Five factors were listed in more than one study—four factors were listed in two studies and one factor was listed in three studies—and nine factors were found in only one study.
Five factors showed no significant association with the administration of continuous palliative sedation.20,21 Of the remaining nine factors, eight showed an increased probability of the administration of continuous palliative sedation. These eight factors were patients who were younger; patients who were male; patients with a cancer diagnosis; patients with feelings of hopelessness; patients dying in a hospital; and patients whose attending physicians were very or extremely nonreligious, working in “other hospital” specialties, or in favor of assisted death.14,20, 22–25 The factor “patients living in a Dutch speaking community setting” showed a decreased probability of receiving continuous palliative sedation. 26
Discussion
In this review, we found nine factors associated with the administration of continuous palliative sedation. Three studies showed an increased probability of receiving continuous palliative sedation among younger patients.14,22,23 An explanation for the association between younger age and the administration of continuous palliative sedation could be related to the disease trajectory in such patients. Among younger patients, the average disease trajectory tended to be more aggressive, thus resulting in a higher likelihood of administering palliative sedation. 27 Furthermore, many older patients experience spontaneously diminished consciousness in their final days of life, which may reduce the apparent need for palliative sedation. 28 In addition, because of dementia and inadequate diagnostic tools, signs of pain and other types of suffering may not be well recognized at the end of life among very old patients, which could explain the limited usage of palliative sedation among these patients. 22 For these reasons, we conclude that the association between age and continuous palliative sedation may be the result of an indirect or mediated causal relationship, although the mentioned underlying factors have to be identified as determinants in future research.
With respect to sex, Miccinesi and colleagues stated that it is difficult to explain why male patients are more likely to receive palliative sedation. 14 A study by Caraceni and colleagues, published after April 2011, confirmed the result of Miccinesi and colleagues by showing that palliative sedation was more frequently indicated in male patients (odds ratio 3.2; 95% confidence interval 1.5–7.0). 15 In general, women have different trajectories at the end of life than men. Indeed, women tend to live longer and have a different disease epidemiology and are more likely to receive care in a nursing home at the end of life, which may lead to different medical end-of-life decisions. 29 In addition, at the end of life, men can become more isolated and receive less social support and tend to be more reticent and less willing to discuss emotional and psychological issues, thus making male patients more vulnerable than female patients.29,30 Although this review's findings regarding sex were inconsistent, the aforementioned factors could contribute to a patient's endurance and may exacerbate symptoms in male patients, ultimately resulting in the administration of palliative sedation. Therefore, sex, although associated, seems to be not an independent determinant but rather a contributing factor because of underlying patterns in the health status of and care for male patients.
Van den Block and colleagues used language to differentiate between two communities in Belgium and found that although language and culture are strongly related, specific underlying cultural factors, e.g., the degree to which curative, technological, and specialist medicine is appreciated, could more fully explain the difference between patients living in Dutch speaking and French speaking community settings. 26
Miccinesi and colleagues suggest that palliative sedation is more commonly performed among cancer patients because the clinical condition is more severe in these patients. 14 In addition, cancer patients may experience a more aggressive disease trajectory, and there could be a higher prevalence of refractory symptoms among these patients, thus explaining the association of cancer with a higher probability of receiving continuous palliative sedation.27,31 Moreover, the end or terminal stage of the disease is better defined in this patient group than in patients suffering from COPD or heart failure. 32 In this case, the cancer diagnosis itself seems to be the explanatory factor that results in an increased likelihood of requiring continuous palliative sedation and therefore can be considered a determinant.
Cohen and colleagues indicated that hospital policies that consider continuous palliative sedation to be an acceptable alternative to euthanasia may be a possible reason for the increased use of palliative sedation in these settings. 25 In addition, Cowan and colleagues found that in the state of Tennessee in the United States, nursing homes, in contrast to hospitals, are often inadequate with respect to the standards of care, protocols, and training that are needed to support palliative sedation. This inadequacy may decrease the prevalence of palliative sedation at these care centers, even in cases in which sedation may actually be indicated. 31 Additionally, when a patient reaches an adequate level of symptom control, the patient is discharged from the hospital to receive end-of-life care in a hospice or at home. Therefore, it is not surprising that patients who are not discharged from the hospital because of complex clinical conditions are presumably more likely to receive palliative sedation prior to dying. 14 It is likely that factors other than being an inpatient determine the administration of palliative sedation, e.g., the patient's symptoms and symptom severity and attitudes toward euthanasia. 23
Seale and colleagues reported an increased probability of receiving continuous palliative sedation in patients treated by very or extremely nonreligious physicians. 20 It would seem advisable that doctors become more aware of how broader sets of values, such as those associated with religiosity or a nonreligious outlook, may enter into their decision making in end-of-life care. 20
Maessen and colleagues reported an association between patients' feelings of hopelessness and continuous palliative sedation. 24 However, Maessen and colleagues provided no interpretation of this finding, and no odds ratio was reported. 24 In addition, because patients' proxies retrospectively answered questions about feelings of hopelessness, an under- or overestimation bias may have been present; thus, caution should be used in interpreting this finding.
Seale and colleagues provided no interpretation of their finding that palliative sedation was more likely to be reported by physicians working in “other hospital” specialties. 23 Because the term “other hospital specialties” was not clearly defined, the implications of the outcome of this study are difficult to understand. Additionally, in this study, physicians from several “other hospital” specialties indicated that sedation was provided for reasons other than refractory symptoms. 23 Another study by Seale and colleagues reported on the same cohort as in the aforementioned study and found no difference regarding the use of continuous palliative sedation among physicians from different specialties. 20
Strengths and limitations of this study
To the best of our knowledge, this is the first systematic review of published factors associated with the administration of continuous palliative sedation. However, several issues limit the interpretation of the findings in this review. First, several of the studies did not use determinants of palliative sedation as a primary outcome; rather, the studies considered such factors during a secondary analysis of the data. Accordingly, our methodological assessment according to Hawker's method evaluated the aims, methods, analysis, results, and implications of research questions that were not directed toward the purpose of our review. Second, all of the reviewed studies were retrospective and primarily used questionnaires with response rates varying between 42% and 75%, which carry their own associated limitations because of recall bias and nonresponder bias. Moreover, in this type of study, it is only possible to examine associations; cause-and-effect relationships cannot be studied. Third, several of the findings were based on the answers of patients' proxies or based on information from general practitioners who provided information about patients who died in the hospital, thus making the findings susceptible to under- or overestimation bias. Fourth, all included studies focused on continuous deep palliative sedation, whereas the objective of this study was to identify the determinants of the administration of continuous palliative sedation in general, which potentially limits extrapolation from the studies. Additionally, the study designs varied with respect to population, setting, and attending physician, all of which make comparisons difficult and limit the generalizability of the results. Fifth, in several studies, multivariate calculations of an odds ratio or relative risk were lacking, and descriptions of the statistical methods were inadequate, e.g., information on the factors used in the multivariate models was absent. In addition, none of the multivariate models included factors such as the patient's symptom severity. Moreover, comparing one determinant across several studies can be problematic because of differences in the underlying multivariate models and the number and types of factors used in the analyses. Furthermore, the results of different studies regarding the same determinant are not always consistent. Finally, there is wide variation in terminology for independent variables. Terms such as “determinant” or “predictor” are often used in the literature, even in cases in which a causal relationship is not present. In such cases, terms such as “association” or “correlation” would be more appropriate.
Conclusions
Although the literature suggests that there are several determinants of the administration of continuous palliative sedation, this review uncovered important gaps in our current understanding of these determinants and even questioned whether the identified factors are actually determinants or would be better labeled as factors associated with the administration of continuous palliative sedation. This gap in our current understanding of the mechanisms leading to continuous palliative sedation limits our ability to offer proactive care to patients requiring palliative measures. In particular, determinants that can be acted upon early in the clinical palliative care trajectory are more relevant from a clinical perspective, e.g., factors such as medication, symptoms, and symptom severity. In such cases, appropriately applied interventions can alter the course of symptoms and the patient's eventual need for palliative sedation. However, knowledge of determinants of the administration of continuous palliative sedation does not exclude the need for qualified personnel. Physicians must be competent in the assessment of symptoms and the symptoms' correct treatment prior to starting continuous palliative sedation and in the administration and evaluation of continuous palliative sedation.
Future research regarding determinants of the use of palliative sedation should be performed using a prospective multicenter study design and a research protocol that includes clear and timely baseline measurements during the patient's trajectory, e.g., at admission to a hospital. Such studies should use a multivariate analysis after clearly defining continuous palliative sedation and should focus on clinically relevant determinants.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.