
Abstract
Abstract
Background:
Pediatric medical experiences are potentially traumatic but may lead to psychological growth.
Objective:
The study objective was to synthesize the published literature regarding posttraumatic growth (PTG) in parents and patients with serious pediatric illness (SPI) into a conceptual model.
Methods:
We systematically searched MEDLINE, CINAHL, PsychInfo, and Sociological Abstracts in December 2012 to identify articles on stress or trauma caused by medical events with PTG as an outcome, reviewing articles pertaining to the pediatric population. We additionally reviewed articles outside pediatric medicine that described a model of PTG.
Results:
Of the 605 articles identified, 55 met inclusion criteria, 26 of which examined parents or pediatric patients. Parents and children may experience PTG following medical trauma through a combination of cognitive and affective processing of their subjective experience. Components of SPI-PTG are unclear, but may include greater appreciation of life, improved interpersonal relationships, greater personal strength, recognition of new possibilities in one's life course, spiritual or religious growth, and reconstruction of a positive body image. Individual characteristics, and the level of social support, may affect the likelihood that SPI-PTG will occur. SPI-PTG in siblings and other family members has not been well studied.
Conclusions:
SPI-PTG is an important but understudied and inadequately understood phenomenon affecting children with SPI and their family members. Research should focus on clarifying SPI-PTG domains, creating measurement instruments, assessing SPI-PTG across the pediatric age range and among family members, and improving our understanding of and ability to positively intervene regarding the cognitive processes of rumination, sense making, and benefit finding.
Introduction
T
The effects of traumatic experiences are, however, not universally negative. Some people exposed to trauma do not develop PTSS or PTSD, and may even realize psychological benefits. This phenomenon, termed posttraumatic growth 15 (PTG), is the positive psychological change that results from a struggle through a life-altering experience, and in adults is found to include five domains: (1) greater appreciation of life, (2) improved interpersonal relationships, (3) greater personal strength, (4) recognition of new possibilities in one's life course, and (5) spiritual or religious growth.16,17 PTG has recently been studied in children and adolescents exposed to natural disasters,18,19 unwanted pregnancy, 20 death of a family member,21,22 parental divorce, 23 and child sexual abuse. 24
Complete psychosocial care should not merely seek to control adverse effects, but also to help the patient to realize benefits from their experience. Most traumatic stress interventions, however, seek to reduce adverse effects, rather than foster growth. PTG is a potentially useful paradigm for providing complete psychosocial care, since it focuses on this missing element. To date, however, no review of the literature has examined PTG in the specific setting of pediatric disease, which should include the experiences of parents.
This review analyzes and synthesizes the published literature on PTG following an SPI experience for parents and patients (SPI-PTG), as well as the pertinent literature on the PTG framework in general. Specifically, we present the results of this review within the framework of a conceptual model of SPI-PTG. We then discuss how this model can guide the provision of complete psychosocial care to parents and patients following SPI trauma, facilitating the path towards growth, and can help shape future areas of research.
Methods
We conducted a systematic search of the literature in December 2012 through MEDLINE, CINAHL, PsychInfo and Sociological Abstracts (see Fig. 1). Search terms included “posttraumatic growth,” “post-traumatic growth,” and “stress-related growth.” We identified and searched with MeSH terms: in MEDLINE, “resilience, psychological” and “stress-disorder, posttraumatic;” in CINAHL, “personal growth” and “trauma;” and with descriptors in PsychInfo and Sociological Abstracts, “coping behavior,” “trauma,” and “emotional adjustment.” We reviewed the reference section of each paper to find other relevant articles not detected by database searches.

Study flow diagram.
We included articles in which (1) stress or trauma was caused by a medical event and (2) positive psychological change was an outcome measure. We selected articles with samples of pediatric patients and parents of pediatric patients. Articles that were excluded were on the growth of physical tissue; environmental trauma such as war; motor vehicle accidents that did not cause physical injury; physical and sexual assault; and child maltreatment. Because of the limited literature base of PTG within pediatric disease, and in order to augment the synthesis of our conceptual model, we drew from articles that described models of PTG even if they were largely based on adults or the trauma was not a medical event. We searched for but were unable to find sufficient articles on PTG in siblings of child patients or of other family members.
Using a conceptual model of PTG in adults developed previously, 25 all the articles included in this study were read and coded for the presence of elements from the original model. The most commonly occurring elements were analyzed for variations, similarities, and revisions specific to the experience of pediatric medical trauma, and from this analysis we generated a conceptual model of SPI-PTG.
Results
We identified 17 studies examining PTG in parents of children with pediatric disease5,26–41 (see Table 1), 7 studies that demonstrated PTG or benefit finding in children with pediatric disease42–48 (see Table 2), and 2 that included both parents and pediatric patients.49,50 We summarize the findings from these studies in the nine components of our conceptual model of SPI-PTG: (1) the nature and subjective experience of the traumatic event, (2) trauma and the disruption of a personal worldview, (3) PTG as rebuilding or reshaping this worldview, (4) elements of SPI-PTG, (5) cognitive processing underlying SPI-PTG, (6) affective processing underlying SPI-PTG, (7) posttraumatic after-events, (8) individual characteristics affecting SPI-PTG, and (9) social support affecting SPI-PTG (see Fig. 2). Based on the existing literature, our conceptual model primarily applies to parents and caregivers of pediatric patients, but we also consider how the model could apply to the patients themselves. What follows are the nine components of this model.
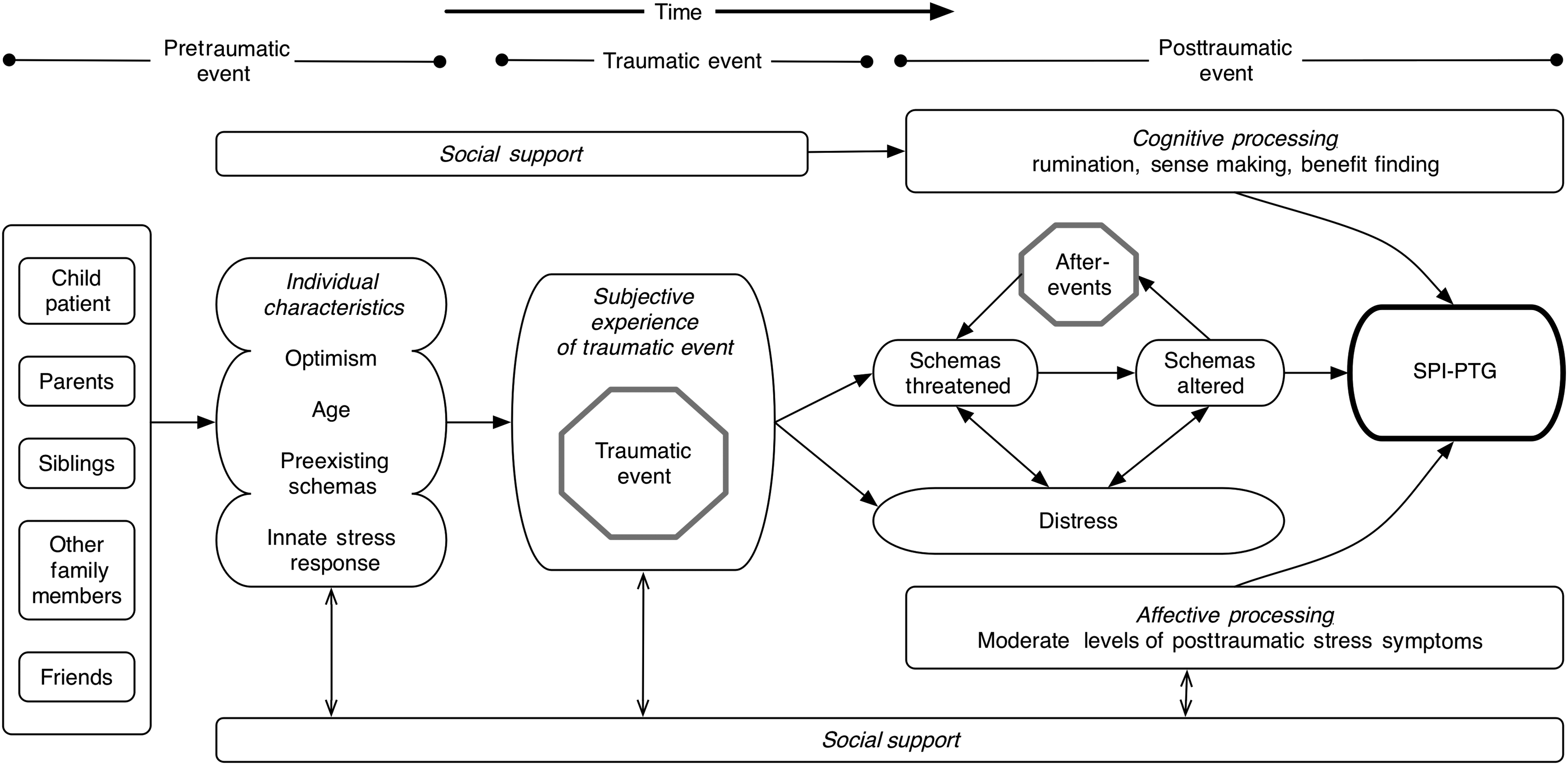
Mechanisms underlying posttraumatic growth in pediatric medical trauma.
ASD, autism spectrum disorder; HSCT, hematopoietic stem cell transplant; PTG, posttraumatic growth; PTGI, posttraumatic growth inventory; PTSS, posttraumatic stress symptoms.
PTG, posttraumatic growth; PTGI, posttraumatic growth inventory; PTSD, posttraumatic stress disorder.
Nature of traumatic events and subjective experience of trauma
By the standard clinical definition, a “traumatic” event poses a life threat or engenders a sense of helplessness within the victim (patient) or an individual who cares deeply for the victim (parent). 51 The trauma literature has consistently demonstrated that the subjective experience of the traumatic event is a more important determinant of psychological well-being than the objective nature of the event itself.38,52–54 Correspondingly, in pediatric studies the objective severity level of medical illness or risks of treatment are generally not associated with the degree of posttraumatic stress or PTG in parents or patients (although two studies have shown that PTG varies with type of diagnosis).1,10,40,47–50
Trauma and the disruption of a personal worldview
Every individual has his or her own personal understanding of and perspective on the world and interprets life events within the context of this perspective, termed the “assumptive world.” This assumptive world consists of a set of cognitive constructs known as “schemas,” the basic units of one's understanding of oneself and the world. 55 Traumatic events threaten the stability and validity of this pre-understanding and perspective by challenging basic assumptions and expectations of how the world will operate.
PTG as rebuilding or reshaping the worldview
Early conceptions of PTG posited that the shattering of one's assumptive world, which comprises one's schemas, was a necessary condition of PTG. 16 The “seismic” event destroyed an individual's understanding of how and why events occur in the world, of purpose, and life meaning.17,55 Rebuilding schemas through thought and reflection was essential, but there was also the opportunity to construct a stronger and more resilient assumptive world.
One's assumptive world does not, however, need to be shattered by traumatic events in order to catalyze growth.20–22 In order to account for a broader range of schema alteration we introduce the term “threatened schemas” to indicate the dynamic process through which schemas are changed in response to the traumatic event. The threat and resultant change can be conceptualized through two ends of a spectrum of schema alteration: (1) the traumatic event imparts change that is incorporated into preexisting schemas, with the threat essentially altered in meaning or interpretation and assimilated into an expanded worldview, or (2) the trauma overwhelms preexisting schemas, resulting in the creation or adoption of brand new schemas, composing a markedly reconfigured worldview. 53 These processes can occur swiftly or slowly, and can result in either reduced personal resilience, PTSD, or—in the case of PTG—enhanced capacity. 62
Elements of SPI-PTG
Adult PTG is thought to consist of five elements: (1) greater appreciation of life, (2) improved interpersonal relationships, (3) greater personal strength, (4) recognition of new possibilities in one's life course, and (5) spiritual or religious growth.16,17 Studies have demonstrated these domains to be separate, meaningfully correlated, and observed across cultures.56–65 These elements can be measured by the Posttraumatic Growth Inventory (PTGI), a validated instrument.
SPI-PTG, however, may be composed of different elements. Of the studies we analyzed in the pediatric population that used the PTGI, few could distinguish between the five domains (i.e., appreciation, interpersonal relationships, personal strength, new possibilities, and religious or spiritual growth); of those that did, each domain showed prominence in at least one article and none of the five domains was identified in every article.5,27–34,37–39,42,46
The adult PTG model includes spiritual change as one of the five subscales in the PTGI, because traumatic experiences are often credited with deepening of religiousness and spirituality.16,66 There has not been, however, sufficient evidence to distinguish the degree to which an individual's ‘baseline’ spirituality contributes specifically to the spiritual change domain of PTG as opposed to PTG broadly 67 or to demonstrate whether the language used to describe one's personal beliefs or experiences of spirituality or religion tends to inherently inflate the measures of PTG. Furthermore, there is scant evidence of the role of spirituality or religiousness in parents of pediatric patients.
In addition to the five psychological domains, physical disease also challenges one's understanding of one's own body and, in the framework of SPI-PTG, may lead to a new body awareness, set of priorities, and health behaviors that might be considered a sixth domain of SPI-PTG.53,68
Cognitive processing underlying SPI-PTG
Cognitive processing is a broad term that describes how an individual works through threatened schemas and restructures his or her assumptive world. In early conceptualizations of PTG, recurrent, event-related, and sometimes-intrusive thinking about the traumatic event was termed “rumination” and espoused as the cognitive processing necessary for growth to occur.16,17,23,69,70
Ruminative thinking has been divided into two types: “intrusive” (unintentional recollection), often occurring soon after the event, and “deliberate” (intentional reexperiencing of the event), often occurring later. While both intrusive rumination and deliberate rumination are independently positively correlated with PTG, deliberate rumination may be more strongly correlated.17,54,71–73 Two other forms of cognitive processing, “sense making” and “benefit finding,” have been shown to be separate processes independently linked to PTG.
Sense making occurs during the initial posttraumatic period during which schemas are threatened, when the individual attempts to cope with the adjustment by making sense of the situation. The individual references preexisting schemas to attempt to comprehend the event, and through this sense making takes an intermediate step toward PTG.17,55,74
Benefit finding, on the other hand, is the process by which an individual assigns positive value to how the trauma affected them.53,55,69,74 Empirical evidence suggests benefit finding is associated with more positive well-being and is related to the presence of an optimistic disposition in parents and pediatric patients, though benefit finding may occur without PTG, and vice-versa.48,50,75,76 A victim of trauma may see value in the experience that does not lead to growth, or may experience some PTG without recognizing it as such.
Overall, sense making shows a greater effect soon after the trauma, while benefit finding grows more important over time.53,70,74
Affective processing underlying SPI-PTG
In addition to the cognitive restructuring that occurs in the aftermath of trauma, an affective component of the posttraumatic coping process can produce clinical distress. This distress manifests the syndromes of anxiety, depression, and PTSD; and the management and prevention of these symptoms has been the primary focus of trauma-informed care, which emphasizes that after the ABCs of resuscitation and life support, one may continue intervention by applying DEF (reduce distress, emotional support, family). 77
Cross-sectional studies suggest that PTSS, which includes intrusive thoughts, avoidance, and hyperarousal, is associated with PTG, and that a certain level of posttraumatic stress (that is, not too much and not too little) likely correlates with PTG.28,40,49 These studies do not clarify whether posttraumatic stress precedes PTG or is a by-product of the process; PTG can also occur in the absence of posttraumatic stress.20–22 The relation of depression and anxiety to PTG is less clear. Longitudinal studies have shown that both high and low levels of anxiety and low levels of depression correspond to PTG.28,30,42,48 Other cross-sectional studies have, however, shown no association between depression or anxiety and PTG.28,30,31,46
Posttraumatic after-events
A life-threatening illness experience often extends beyond the initial traumatic event (such as a terrifying diagnosis) and includes subsequent events (surgeries, treatments, complications, relapses, or even something that would normally be perceived as low stress, such as sleeping overnight in the hospital) that further incite stress and re-threaten schemas. These after-events, like aftershocks following a major earthquake, can be understood and accommodated by an individual as an expected continuation, albeit of diminished intensity, of the initial trauma, or be responded to with a full-blown sense of a new traumatic event. 45 As with the initial traumatic event, parents and pediatric patients may experience these after-events differently; a pediatric patient may take chemotherapy toxicity in stride while being distressed at the loss of their hair, with their parents experiencing the reverse. Interestingly, both parents and pediatric patients exhibit a greater propensity to experience PTG when the disease continues to engender a certain degree of emotional distress.45,50 There is likely a balance between ongoing threat and overarching sense of safety that optimally fosters SPI-PTG in parents and pediatric patients.
Individual characteristics affecting SPI-PTG
Several personal and psychological characteristics may predict how individuals process traumatic experiences. Optimism, defined as one's expectation for positive outcomes to occur more often than negative ones,17,69 may be related to PTG, 78 and to benefit finding.26,50,74–76 Age could also affect the SPI-PTG process. Children, prior to adolescence, have not typically acquired the life experiences or the cognitive skills to assemble sophisticated assumptions about the world. They consequently have less fully formed schemas, and their process of change through trauma is likely distinct from adults. 18 In the PTG process in adults, schemas altered by trauma are subsequently reconstructed. Because a child's assumptive world is underdeveloped, PTG in children is theorized to occur through development of completely novel schemas, rather than reconstruction of pre-formed ones, although the data in support of this hypothesis is mixed.19,22,47,48,54,79 Additionally, PTSS in the aftermath of cancer diagnosis is more likely to persist if diagnosis occurs during the adolescent period than at a younger age.1,4 These findings suggest that the process of SPI-PTG depends on accumulated life experience as well as the cognitive maturation of the individual.
Social support affecting SPI-PTG
Social elements of support can be separated into two levels—general, relating to social values and cultural influence, and local, including family, friends, and peers.70,80–82 At the general level, race and ethnicity appear to play an important role, although evidence is conflicted.54,67,76
More robust evidence exists for the role of local elements in PTG. Several studies have demonstrated a strong correlation between social support and PTG.40,53,78 Social support involves both the contribution of an individual's support network to the individual's PTG and the individual's influence upon that network. The patient's behavioral response itself can serve as a stressor for other family members and may result in family members exhibiting a greater degree of both PTSS and PTG. 80 The empirical evidence for the role of these relationships in pediatric disease is, however, limited; one study has shown that mutual coping and thinking can lead to more pronounced PTG among parents, 29 while another showed no correlation between parental PTG and the pediatric patient's degree of benefit finding. 50
Discussion
Serious pediatric illness, such as is found among patients receiving pediatric palliative care, threatens to dramatically alter the lives of children and their families. In the struggle through traumatic medical experiences, patients and families can suffer symptoms that undermine their ability to cope with the illness. Most families, however, find ways to endure the trauma—and may, in fact, benefit from the experience, depending in part on personal characteristics like age, optimism, and worldview, and through cognitive and affective processing aided by their social support network. The SPI-PTG conceptual model outlines the various processes through which families experience SPI as trauma and helps clinicians identify the aspects of that recovery so that they may facilitate the path to growth.
This study incorporates a large body of literature from psychology and medicine, and is consistent with major schools of thought on traumatic stress. The major limitation is the relative dearth of published work on responses to medical trauma among children and their caregivers, which at this time makes it difficult to make specific recommendations to pediatric caregivers seeking to promote PTG. Drawing upon all potentially relevant PTG research, our conceptual model should promote research into interventions that facilitate families' movement away from dysfunction or deterioration and toward growth.
Work in this direction is already underway: “Trauma informed care” emphasizes that after the ABCs of resuscitation and life support, clinicians continue intervention by focusing on DEF (reduce distress, emotional support, family). The SPI-PTG conceptual model suggests that we direct research in six main areas. First, we have to clarify the domains of SPI-PTG and develop valid and sensitive instruments to measure them. Second, we need to comprehensively assess SPI-PTG in not only parents but also child patients, siblings, other family members (such as grandparents), and friends (such as close school peers) This may include studies of when and how children are informed of their diagnoses, as different times and methods may have different traumatic impact. Third, we must investigate how SPI-PTG varies in children of different developmental ages. Fourth, we must determine how the cognitive processes of rumination, sense making, and benefit finding can result in PTG following an SPI experience, and develop clinical interventions to facilitate these processes. Fifth, we must clarify the seemingly paradoxical role of distress in the prompting or promotion of PTG following an SPI experience. Sixth, using the conceptual model as a guide we must develop reliable and practical clinical interventions for health care providers to promote PTG in pediatric patients and their families.
Although the experience of SPI can mark some of the darkest days for patients and families, the possibility exists for PTG, and to that end we should advance our care and future research.
Footnotes
Acknowledgments
The authors gratefully acknowledge comments on earlier versions of the manuscript by Chris Renjilian.
Author Disclosure Statement
No competing financial interests exist. No conflict of interest exists regarding the conduct or report of this study. Core funding was provided by the Research Institute of The Children's Hospital of Philadelphia, and preparation of this paper was also supported by K05CA128805 (Kazak).