
Abstract
Abstract
Objective:
Our aim was to investigate the feasibility of completing an exercise program in patients with advanced cancer and to obtain preliminary data of its impact on physical and quality of life (QoL) outcomes.
Methods:
We conducted a nonrandomized pilot study. Participants were 26 palliative care patients with advanced cancer (mean age=54.5 years; standard deviation [SD] 8.9 years) of the outpatient clinic of the medical oncology and the urology departments of a medical center in The Netherlands. Participants followed an individually graded group exercise program, consisting of resistance training and aerobic exercise, twice a week during 6 weeks. Feasibility of the training program, muscle strength, aerobic fitness, body composition, QoL, fatigue, and physical role, social, and activities of daily living (ADL) functioning were assessed at baseline and immediately after the intervention.
Results:
Dropout rate during the training period was 35% due to disease progression. After the training period, based on intention to treat analysis, muscle strength and aerobic functional fitness had increased significantly (p≤0.01). A significant decrease in fat percentage (p≤0.02) was observed. QoL had increased significantly (p≤0.02), as well as social (p≤0.04), physical role (p≤0.01), and ADL functioning (p≤0.05). Fatigue decreased significantly on the Checklist Individual Strength (CIS) and RAND-36 questionnaires (p≤0.02), however not on the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 (p=0.48). No change in physical functioning was observed with the EORTC QLQ-C30 and RAND-36 (respectively, p=0.33 and p=0.09).
Conclusions:
These preliminary results show that physical exercise in patients with advanced cancer is feasible. A significant impact was observed on physical and QoL outcomes. These findings need to be confirmed with a larger-scale, randomized controlled trial.
Introduction
P
Cancer and its treatments can decrease physical fitness, muscle strength, and the level of physical activity.4–6 Physical exercise has been shown to diminish side effects by improving patients' health status.6,7 Fatigue and impairment of physical performance are the most common results of advanced metastatic cancer. 8 It is not only the negative catabolic effect on muscles that plays an important role in this mechanism: one third of the reduction in physical functioning in cancer patients can be attributed to physical inactivity. 8 This may lead to progressive deconditioning, which has a major negative impact on activities of daily living (ADL), participation in social life, and quality of life (QoL).4,5,8–10 Fatigue, decreased muscle strength, and reduction of lean body mass, bone mass, and aerobic capacity cause an overall decrease in QoL.5,7,11 Post-training effects in cured and curable cancer patients increased cardiopulmonary function, muscle strength, bone mineral density, and QoL, and reduced body weight, fat mass, and feelings of fatigue.6,7,12
Recently, some studies have been published showing the positive effects of exercise and physical activity on fatigue and QoL in patients with advanced cancer.8,12–14
During the palliative phase, patients have to deal with a decrease in physical and ADL functioning, which has a negative effect on autonomy. Physical exercise is considered to be effective in reducing and/or preventing functional decline in the elderly.9,15,16 Patients are willing to participate in an exercise program.13,17,18 They consider physical functioning and physical condition important determinants of QoL, and want to stay physically independent in ADL as long as possible.8,19
Objective
The primary objective of this study was to determine the feasibility of completing an exercise program in patients with advanced cancer. The effects of this exercise program on muscle strength, aerobic functional fitness, body composition, QoL, fatigue, and ADL functioning were explored.
Design
A pilot pretest–post-test intervention study was performed. The study was approved by the institutional medical ethical committee. All participating patients gave written informed consent.
Settings/Subjects
Participants were recruited from the outpatient clinic of the medical oncology and the urology departments of a medical center in The Netherlands in February and March 2010. Inclusion criteria were: 18 years of age or older, histological confirmation of incurable metastasized cancer, recurrent or progressive disease, a life expectancy of 3 months or longer, being able to walk at least 6 minutes, and the desire to increase physical activity level or endurance. Active, palliative anticancer therapy was allowed. Exclusion criteria were having a clinically relevant severe cognitive disorder or emotional instability, problems with the Dutch language, participation in a rehabilitation program in the past 3 months, or comorbidities that seriously influenced physical performance capacity (e.g., heart failure, chronic obstructive pulmonary disease). Flow of participants through the study is shown in Figure 1. Prior to the intervention an intake session was scheduled for each participant. This included a medical history, a physical examination, and physical tests to measure baseline level of physical fitness.
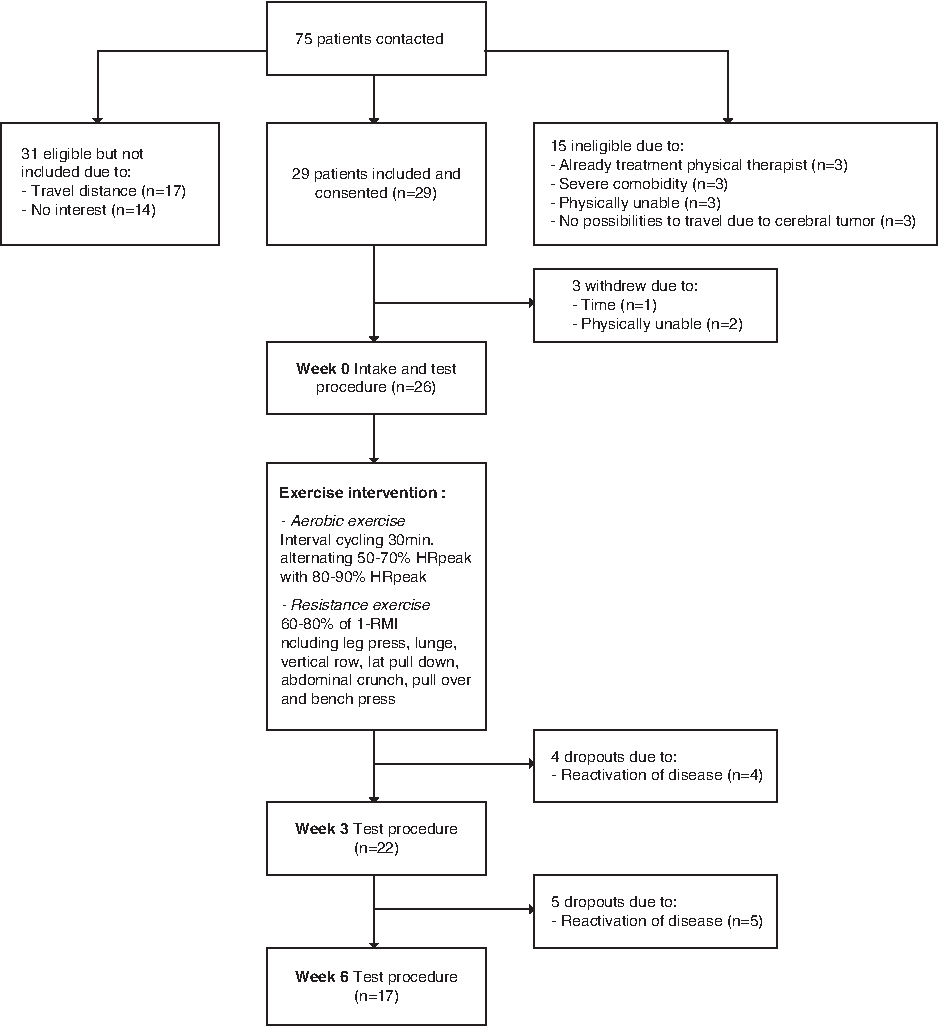
Participant recruitment and follow-up in study group.
Intervention
The intervention, developed in cooperation with a medical oncologist, took place in three physical therapy centers. The 6-week training program consisted of resistance and aerobic interval training two times a week for 2 hours (Fig. 1). Participants trained under supervision of a physical therapist, in groups of three to five persons; resistance training equipment and bicycle ergo meters were used. Every participant received a tailored, graded training program adjusted to his/her needs and abilities.
Aerobic training intervention
The aerobic training consisted of cycling on an interval basis for 30 minutes prior to the resistance training. Intervals consisted of bicycling for 4 minutes at 80% to 90% of peak heart rate (HRpeak) alternated with 3 minutes at 50% to 70% of HRpeak. Warming up and cooling down were performed at 60% to 70% of HRpeak. During cycling, heart rate was monitored using a Polar breast band (Polar T31 Breast Band, 2008, Polar Electro, Finland). On the nontraining days participants were asked to exercise aerobically at home on a moderate level (talking briefly remains possible) for 30 minutes (continuous or interrupted).
Resistance training intervention
The resistance program consisted of seven exercises in a circuit, targeted to enlarging those muscle groups that are important in ADL activities. The following exercises were executed: (1) leg press (quadriceps, glutei, gastrocnemius); (2) lunge (quadriceps, glutei, hamstrings); (3) vertical row (longissimus, biceps brachii, rhomboideus); (4) lateral pull down (rhomboideus, latissimus dorsi, biceps brachii, trapezius); (5) abdominal crunch (rectus abdominis); (6) pull over (pectoralis, triceps brachii, deltoideus, trapezius); and (7) bench press (pectoralis major, triceps). Exercise level varied per patient, according to problems experienced and goals regarding ADL functioning. Resistance exercises were performed at 60% to 80% of one-repetition maximum (1-RM) and consisted of three sets of 12 repetitions. Progression was conducted by the graded activity principle, implying that the focus was on success and positive experiences; negative experiences were prevented as much as possible. 20 After 3 weeks, training progress was evaluated and the program adjusted by means of the 1-RM test.
Measurements
Feasibility measures were operationalized by adherence rate, the reasons behind dropouts and their number, possible injuries or complications during and due to the training program, and the number of participants who completed the training program and indicated that they wanted to continue training.
To measure muscle strength the indirect 1-RM test was used. 1-RM is the maximum weight (in kilograms) that can be lifted or pulled once. Indirect 1-RM values were determined in different muscle groups and then calculated from the Brzycki equation.21,22 1-RM is stated in kilograms in proportion to body weight. Muscle groups were tested with the resistance equipment that was also used for the training (leg press, vertical row, abdominal crunch, bench press, lunge, pull over, lateral pull down). For the overall muscle strength, a hand grip dynamometer (HGD) (SH5001 Saehan Hydraulic Hand Dynamometer, 2007, Saehan Corp., Korea) was used. 23 The HGD is a test that measures the maximum isometric strength of the hand and forearm muscles. This test is also frequently used as a general strength test. The HGD used in this study had a range of 0 kg to 90 kg and a deviation of 2%. The HGD test was repeated three times with rest periods of 30 seconds. Next, the three HGD test outcomes were averaged. Both the 1-RM and the HGD test were performed in weeks 0, 3, and 6. In contrast to the 1-RM muscle strength variable, the HGD variable was not part of the training program.
The 6-minute walk test (6MWT) is a test that measures aerobic functional fitness indirectly by walking distance. 24 The 6MWT was conducted indoors on a pre-measured test course of 20 m. Patients were instructed to walk as long and as fast as they could for 6 minutes, and they were allowed to rest and to use walking aids if necessary. The heart rate and saturation were registered with a fingertip pulse oximeter (Onyx II 9550, Nonin Medical Inc., 2007, Plymouth, MN). The 6MWT was performed in weeks 0, 3, and 6.
In week 0 and week 6, as anthropometric variables the participants' height, weight, and body fat percentage were measured. Body mass index was calculated using height, weight, gender, and age. Body fat percentage was measured using the Durnin and Womersley method. 25 Skinfolds on the subscapular, triceps, biceps, and suprailiacal areas were measured with a skinfold caliper at the nondominant side or, in a case of breast cancer, at the nonoperated side. Body fat percentage was calculated from the total skinfold thickness (in millimeters) taking age and gender into account.
Fatigue severity was measured in weeks 0, 3, and 6 by the fatigue severity subscale (CIS-fatigue) of the Checklist Individual Strength (CIS) questionnaire, which has excellent psychometric properties,26–29 and by the RAND-36. 30 QoL was assessed at these intervals, using the EORTC QLQ-C30. This questionnaire has been validated for patients with advanced cancer.31–34
ADL functioning was assessed with subscales of the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30, RAND-36, and CIS, namely ADL functioning, social functioning, physical role functioning, and activity level. Also, the Edmonton Symptom Assessment System (ESAS) and the Dutch version of the Distress Thermometer (DT) were used to measure total symptom distress score and number of ADL problems.35,36
Statistical analyses
Frequency analysis was performed. Paired-sample t tests and Wilcoxon signed-rank tests were used to compare pretest and post-test data. In case of dropout, the last observation carried forward procedure was used at week 3 for early dropouts and at week 6 tests for late dropouts. Because this was a pilot study, no power calculation was performed. SPSS statistical software (version 16.0, IBM Corp., Armonk, NY) was used for all analyses.
Results
Thirteen men and 13 women with a mean age of 54.5 (standard deviation [SD] 8.9) years and with several types of cancer took part in the study (Table 1). Mean Karnofsky Performance Scale (KPS) was 79.2 (SD 9.4). Nine patients (35%) dropped out, all because of progression of disease: four participants in the first 3 weeks of the intervention and 5 in the last three weeks. The remaining participants completed all 12 training sessions. Eighty-five percent (22/26) of the participants completed a minimum of eight training sessions. Participants receiving chemotherapy (n=10) missed training sessions the most. In half of the cases, the first training session after chemotherapy was missed due to nausea or severe fatigue. There were no complications or injuries due to the exercise intervention.
Values are presented as absolute figures or means with standard deviation.
BMI, body mass index; KPS, Karnofsky Performance Scale.
Figure 2 shows the evolution in muscle strength for all seven exercise elements over the 6 weeks of follow-up. Muscle strength improved significantly (p≤0.01) between pre- and post-test for all exercises. Overall muscle strength measured with the HGD also improved significantly (p<0.01) during the intervention period.
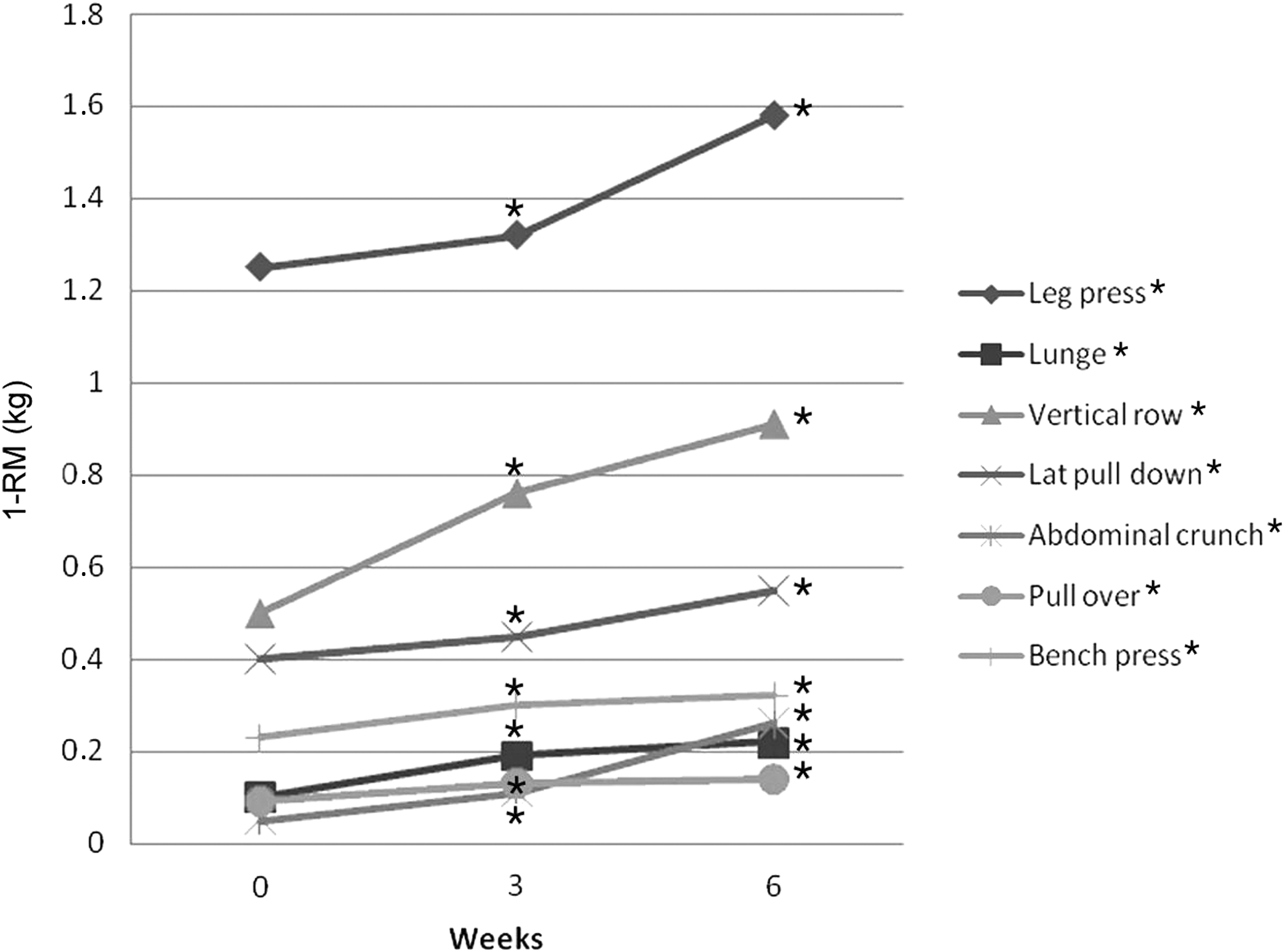
Effect of training on muscle strength (*significant difference).
Walking distance improved significantly (p<0.01) with a mean of 45 m. Mean body fat percentage decreased significantly (p=0.02) with 1% (Table 2). All results are based on intention to treat measurements.
Values are presented as means with standard deviation.
T1 is week 0; bT2 is week 3; cT1 is week 6.
1-RM, one-repetition maximum; 6-MWT, 6-minute walk test; HGD, hand grip dynamometry.
Fatigue, measured with the CIS and with the RAND-36, decreased significantly (respectively, p≤0.01 and p=0.02) (Table 3). Although fatigue also decreased as measured with the fatigue subscale of the EORTC QLQ-C30, this difference was not significant. QoL, measured with the EORTC QLQ-C30, improved significantly (p=0.02). ADL functioning increased, as measured with subscales of the EORTC QLQ-C30, RAND-36, ESAS, and DT. Social functioning improved significantly on the subscale of the EORTC QLQ-C30 (p≤0.04) and the RAND-36 (p=0.04). There was no significant difference in physical role functioning when measured with the EORTC QLQ-C30 and RAND-36. However, using the RAND-36, physical role functioning increased significantly (p=0.01). Symptom burden was significantly (p≤0.04) reduced, as measured with the ESAS. However, the DT showed no decrease in visual analogue scale score. Finally, a significant (p≤0.05) decrease in the number of ADL problems was found, as measured with the DT.
Values are presented as means with standard deviation.
T1-T2; bT2-T3; cT1-T3.
ADL, activities of daily living; CIS, Checklist Individual Strength; EORTC, European Organisation for Research and Treatment of Cancer; ESAS, Edmonton Symptom Assessment System; QoL, quality of life; VAS, visual analogue scale.
Conclusions
The effect of exercise on fatigue and QoL in patients with advanced cancer has not been extensively studied. To our knowledge, this is one of the first studies that investigated an exercise program combining aerobic exercise and resistance training in patients with advanced cancer in the palliative phase. The study results show that a physical exercise intervention in palliative patients with advanced cancer is feasible. All participants who completed the exercise program wanted to continue the exercise intervention after the study period. Sixty-five percent of the participants were able to complete the entire program.
Studying the feasibility of completing an exercise program was our primary aim; the pilot study showed also significant improvements in muscle strength, aerobic functional fitness, body composition, ADL functioning, and QoL. Oncology rehabilitation is a relatively new area in palliative care; there is no consensus about the optimal type of training in a rehabilitation program. The Dutch guideline for oncology rehabilitation 37 recommends that the personal goals and preferences of patients (and their families) should be central in a palliative care rehabilitation program. In doing so, one can strive to prevent and treat symptoms on the one hand, and optimize QoL on the other. As part of this training, it may also be essential for patients and their families to attempt to maintain physical functions, such as climbing stairs. Exercise interventions described in previous studies vary considerably, from cycling and home-based exercises to circuit training. Most other studies used aerobic exercises only and no resistance exercises, although one of the side effects of cancer and its treatment is severe muscle atrophy. 38 Furthermore, cancer-related cachexia is a considerable problem in these patients.4–6,39 When one wants to improve muscle strength and increase muscle mass, resistance exercise seems to be more contributive than aerobic exercise. Also, the ability to participate in ADL and therefore the patient's QoL is related to muscle strength. 40 A study by Lowe and colleagues also showed a significant positive association between physical activity and QoL in patients in a palliative trajectory. 41 In an exercise study by Oldervoll and coworkers 42 all patients with advanced cancer performed circuit training and not resistance training, following the graduated exercise principle. Muscle strength was measured with an HDR instead of with 1-RM measurements of specific muscle groups. 42 A randomized controlled exercise study by Adamsen et al. 9 included patients with cancer undergoing chemotherapy who received a combination of aerobic and resistance training during 6 weeks. A significant difference in muscle strength of the lower extremity was found as well as maximal oxygen consumption, indicating an improvement in physical capacity. However, no significant difference in QoL was found. 9
The patients in our study had a mean KPS score of 79.2, which is comparable to the figures in the 2011 study by Oldervoll et al. 42 This KPS score means that patients are able to perform ADL with effort. Patients in these studies therefore had a relatively fair to good condition, which makes them suitable for an exercise study. For patients such as these, exercise can be very important in sustaining their ADL functioning, and social functioning. More research is needed to decide if exercise is also suitable for patients in poor physical condition.
In our study, physical role functioning increased on the subscale of the EORTC QLQ-C30 as well as on the RAND-36 subscale. Other variables contributing to physical role functioning also increased significantly, such as the activity subscale of the CIS. In addition, the number of ADL problems on the DT decreased. This is in agreement with our hypothesis that exercise improves physical role functioning. The 2006 study by Oldervoll et al. only measured physical functioning with the EORTC QLQ-C30 subscale and showed a slight increase, although not significant. 8 It is remarkable that in our study the physical functioning level is far above those in the studies by Oldervoll and colleagues8,42 and by Scott et al. 43 The physical functioning level of the EORTC QLQ-C30 and the physical functioning level of the RAND-36 increased from week 0 to week 3 and decreased slightly from week 3 to week 6. This can be caused by the principle regression to the mean. Still, there was an increase in these physical levels between week 0 and week 6.
In our study, QoL, also measured with the EORTC QLQ-C30, improved significantly. In the 2006 study by Oldervoll and coworkers, there was a slight but not significant improvement in QoL. 8 In another study, the QoL scores were higher than the norm values for QoL in patients with recurrent or metastatic cancer. 43 A change in any scale of the EORTC QLQ-C30 of at least 10 points is considered to be clinically relevant. 44 In our study, the scale of QoL improved by 6.4 points in the total study population. According to the literature, this could be considered as clinically of limited relevance, but participants did show that they were still improving up the sixth week of training without levelling off. Potentially, patients may benefit from a longer training period so the improvement could also become clinical relevant.
Study limitations
The promising results of this study must be considered with precaution, as a control group was lacking. Other factors than the intervention may have contributed to the observed improvements. As our primary aim was to study the feasibility of the intervention, patients with different types of advanced cancer were included, instead of those with a single type of cancer. Because this was a nonrandomized pilot study, results cannot be generalized for all patients in the palliative trajectory. Further research should focus on specific groups of patients with advanced cancer. Finally, the professional who conducted the physical training also collected the data, which could potentially have caused bias.
The participants in this study were tested three times during the intervention period. Theoretically, the positive outcomes may be a result of improvement in how to perform the tests (learning curve). However, the tests were performed three times with a 3-week interval. The improvement of all patients occurred from week 0 to week 3, as well as from week 3 to week 6. Also, improvements occurred on the subjective measures. A learning effect is generally the greatest between the first two tests, with mean increases of 0% to 17%.45,46
The results of this study suggest that physical exercise is a feasible intervention for patients with advanced cancer in a palliative phase. The effects on physical and subjective outcome variables on psychosocial domains are promising, even in patients with advanced cancer. A randomized controlled trial, with long-term follow-up is needed to substantiate our results and to further assess the impact of exercise interventions on clinical end points such as survival and the effects in specific groups of palliative patients with cancer.
Footnotes
Author Disclosure Statement
This work has not been funded, because this was part of a master thesis.
We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated.