
Abstract
Introduction
C
In the 1970s, cordotomy was a common neurosurgical procedure for chronic pain. It became clear, however, that the effects could wear off over time and could occasionally cause a new deafferentation neuropathic pain.6–8 Cordotomy was therefore usually reserved for patients with nociceptive pain of malignant origin, because the patients' reduced lifespan would reduce the likelihood of wearing off or neuropathic pain.
Since the 1990s, the widespread use of oral opioids and the more recent introduction of intrathecal opioids dramatically reduced the use of cordotomy to manage pain. 9 In the last 20 years, many neurosurgeons have been trained without ever seeing this operation. In 2012, an informal survey of all the functional neurosurgeons within Canada revealed that only 10 of these operations had been performed in the last five years. Cordotomy is a dying art.
Our rare but continued experience with this operation has reinforced our belief that there are patients with medically refractory, unilateral, nociceptive pain due to malignancy who are ideally treated with percutaneous cervical cordotomy.
In this paper we present a small, contemporary series of patients with medically intractable pain in a tertiary care hospital palliative care setting who underwent unilateral percutaneous cervical cordotomy. This cohort is used to highlight the ideal candidate for cordotomy and their expected outcome following surgery. An argument is made for the preferential use of cordotomy in the treatment of patients with medically refractory, unilateral nociceptive pain with life expectancy less than one year. We hope that the operation will continue to be utilized and will be taught to the next generation of neurosurgeons.
Methods
A retrospective review of the hospital and office charts of all patients undergoing cervical cordotomy at the University of British Columbia during the last five years was performed. Patients with complete descriptions of their pre- and postoperative pain and detailed clinical outcomes were included in this review. A brief description of the indications for cordotomy and the potential complications of this operation are also presented.
Results
Four patients met inclusion criteria and are presented briefly below. Patient #1 was a 63-year-old man with a three-year history of hepatocellular carcinoma. He developed a pathological fracture in his left femur due to a metastasis in the femur and pelvis that had previously been irradiated. Orthopedic surgery was not felt to be possible. He was admitted to hospital for pain management. He described a constant, unrelenting severe, sharp pain (“11 out of 10”) in his left hip and thigh that was exacerbated by any movement and left him bedridden. He was treated with intravenous opioid infusions of fentanyl and hydromorphone, gabapentin, nortriptyline, and medical marijuana. He was not felt to be a candidate for intrathecal opioids due to his prognosis of less than three months. His goal was to get pain relief and go home.
A right cervical cordotomy was performed without complication. The following day the patient reported no pain in his hip/thigh. He was able to move both lower limbs and self-transfer to a chair. His opioids were rapidly titrated down due to drowsiness (see Fig. 1), but once they reached 4% of his preoperative dose, he developed symptoms of withdrawal necessitating a slight increase. He was discharged home on postoperative day 10 on a regular dose of hydromorphone amounting to 5% of his preoperative dose of opioids. He reported he “almost feels himself again.” He died pain free two months later.
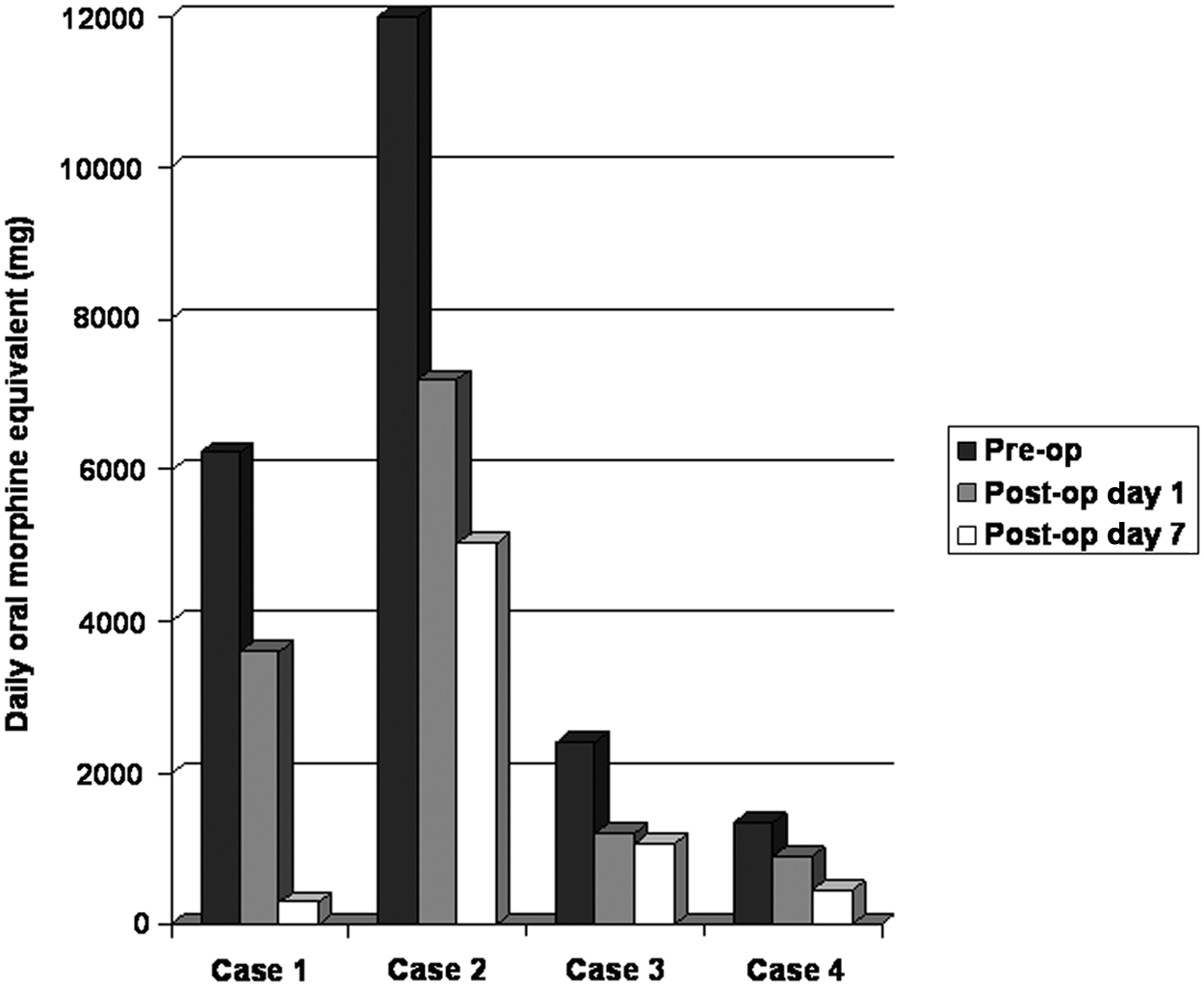
Pre- and postoperative daily oral morphine equivalent (OME). The daily OMEs are presented for each patient before and after (day 1 and 7) cordotomy.
Patient #2 was a 55-year-old woman with a six-year history of renal cell carcinoma with metastases to her pelvis and lungs. She had previously undergone internal fixation for pathological pelvic fractures, but over time the metastases had grown into the hardware causing loosening and pain. She described a severe, constant ache (“9 out of 10”) in her right buttock and thigh that was exacerbated by movement and left her bedridden. A coccygeal bedsore developed that was difficult to treat, because movement to expose it was too painful. She was admitted to hospital for pain control. She was treated with opioids (regular hydromorphone IV and methadone with sufentanil and fentanyl for breakthrough), baclofen, ketamine, and carbamazepine. The dosage left her sedated but still in pain. She was not a candidate for intrathecal opioids, as she had previous spinal surgery and multiple medical comorbidities including intermittent bowel obstruction and obesity. She had previously had a trial of epidural anesthesia which was unsuccessful. Her goal was to get pain relief and get out of bed.
A left cervical cordotomy was performed without complication. Immediately after surgery she reported no pain in her buttock or thigh and began mobilizing. She was able to mobilize to the side of the bed and transfer with assistance to a chair after six days and reported a clear sensorium, because her opioid medications were reduced (see Fig. 1). However her care needs remained complex and she continued to need hospitalization on a palliative care ward for the last few months of her life.
Patient #3 was a 60-year-old man with a one-year history of metastatic melanoma to his right shoulder. He was admitted to hospital for pain management. He described a constant ache (“8 out of 10”) in his right shoulder and scapular region that was exacerbated by any movement of that limb. He was treated with a combination of opioids, ketamine, nortriptyline, gabapentin, metoclopromide, baclofen, and antiinflamatories, which left him sedated and/or delirious at times but still failed to control the pain. His goal was to relieve the pain and get out of hospital.
A left cervical cordotomy was performed without complication. The following morning the patient reported no pain in his shoulder area and began using that limb for activities of daily living. His opioids were reduced (see Fig. 1) and he had no further delirium. He was unable to be discharged home due to complex wound care requirements as well as frailty and fall risk. He died pain free one month later.
Patient #4 was a 69-year-old Mandarin-speaking woman with breast cancer and metastases to her lungs and left chest wall region. She was admitted to hospital for pain control. She reported a constant pressure and deep ache (“10 out of 10”) in her grossly edematous left arm and forearm that was exacerbated by movement. Any care or transfers were difficult and required assistance due to pain and she could not lie flat for any length of time. She was treated with a combination of opioids, antiinflammatories, ketamine, and intravenous lidocaine. The dosage of medication required to reduce the pain to a “6 out of 10” left her confused. The patient's goals were to obtain pain relief and a clear sensorium.
A right cervical cordotomy was performed without complication. Immediately after surgery her left upper limb pain was gone. She helped transfer herself off the surgical stretcher. Her bed mobility improved, but her functional status remained limited due to dyspnea and fatigue. Her opioids were dramatically reduced (see Fig. 1) and she was able to participate in discussions concerning the end of her life. Five days postprocedure she complained of shocks in her left arm that were brought under control by restarting the lidocaine infusion. She died comfortably on the palliative care ward three weeks later.
Discussion
This paper highlights that percutaneous cervical cordotomy can be effective in the palliative care setting. The vignettes presented serve to demonstrate that medically refractory pain can be eliminated following cordotomy with a resultant improvement in quality of life. Cordotomy remains an excellent option for the right patient. Unfortunately, this operation is vastly underutilized in Canada and may disappear if the next generation of neurosurgeons is not exposed to the technique.
Like all neurosurgical procedures, two things are required for a successful outcome—choosing the correct patient and performing the operation correctly. How to perform the operation correctly cannot be taught on paper—it must be seen. A detailed description of the operation is therefore not the intention of this paper. We hope to highlight the ‘ideal’ patient, so that pain specialists and palliative care physicians are aware of this option for their patients and can develop therapeutic collaborations with their neurosurgeons.
Indications for percutaneous cervical cordotomy
Our indication for percutaneous cervical cordotomy is medically refractory, unilateral nociceptive pain in a patient with an expected lifespan of less than one year.
The World Health Organization has produced recommendations for the medical management of pain. 10 A number of articles in the palliative care literature have also provided guidelines for clinicians.11,12 When pain becomes ‘medically refractory’ depends on the expectation of the patient. In our experience, pain treated medically is refractory when (1) the patient continues to feel pain or (2) the dosage of medication required to control pain causes intolerable side effects (e.g., sedation and opioid toxicity). We would also consider pain inadequately treated medically when quality of life is adversely affected by the treatment (e.g., the need for hospitalization to provide adequate pain relief).
For cervical cordotomy to be successful, the location of the pain must be in a dermatome at or below the shoulder (below C4). Pain above this level (in the head and neck) must be addressed with procedures aimed at the trigeminal caudalis nucleus and is beyond the scope of this paper. Unilateral cordotomy interrupts the pain pathway from the contralateral side of the body. After the primary pain fibres have entered the spinal cord ipsilateral to the pain, they synapse in the deep dorsal horn on secondary neurons which send their axons across the anterior commissure and ascend in the contralateral anterolateral fasciculus (where cordotomy can interrupt pain transmission). If pain is bilateral, then a unilateral procedure will not help the pain on the ipsilateral side of the operation. It is possible to perform bilateral cordotomy as an open procedure in the thoracic cord in order to avoid respiratory complications, but we have no experience with this more demanding operation. The quality of pain must be nociceptive, since this is the modality transmitted through the anterolateral spinothalamic tract. Pain due to compression of a nerve is still nociceptive (and therefore responds well to cordotomy) although technically can be considered ‘neuropathic’ since it is originating from a neural structure. Deafferentation pain, however, would not be expected to respond to cordotomy, because its origin may be higher in the neural axis. Pain of visceral origin (e.g., autonomic discomfort from the bladder, gastrointestinal tract) travels in the dorsal midline of the spinal cord and can respond to a different operation—punctuate midline myelotomy. 13
The inclusion criterion of an expected lifespan less than a year is, of course, a rough guideline. The patient's improved quality of life following cordotomy may be lost if the effect wears off, if the disease spreads to the contralateral side, or if the patient develops a deafferentation neuropathic pain. All these complications are less likely to occur if the patient lifespan is shorter.
Contraindications for percutaneous cervical cordotomy
Patients must be able to lie supine and keep their head and neck still for the length of the procedure (approximately 30 to 60 minutes). Severe orthopnea or agitation would preclude this. Patients must be able to provide reliable feedback during physiologic testing. Dementia or delirium would therefore be a contraindication. Our patient #4 was Mandarin speaking and the operation was performed with the aid of a translator. The patient was tested with the translator preoperatively to ensure she could understand our questions and provide reliable feedback. A language barrier is therefore not an absolute contraindication. Puncturing the spinal cord requires intact hemostasis and a coagulopathy or thrombocytopenia would be a contraindication. Since the dura is punctured and will allow some CSF loss, an intracranial mass, which could cause tonsilar herniation, is a contraindication. The spinal pathway controlling automatic breathing (while sleeping) travels in the anterolateral cord and can be damaged during cordotomy.14,15 This is usually not a problem during unilateral cordotomy because the contralateral side remains intact. Occasionally the contralateral lung is defective because of disease burden or hemidiaphragm paralysis and cannot support automatic ventilation while sleeping. These patients are at risk for Ondine's curse—the inability to breathe when asleep. We did have one patient decline the procedure due to this risk.
Consideration of a spinal ‘pain’ pump
Percutaneous epidural or spinal catheters can deliver medications to the spinal cord at concentrations that reduce systemic side effects. There are risks associated with these techniques (e.g., infection, cord injury), and patients often must be in a hospital setting, which can reduce their quality of life. If successful, however, the pump can be surgically internalized and refilled in an outpatient setting. Philosophically, this method of modulating pain is preferable to any destructive procedure such as cordotomy. Although the technology is expensive, it may be ideal for bilateral lower body pain. We still favor cordotomy for unilateral pain, because (1) some nociceptive pain remains refractory to spinal analgesia, (2) spinal anesthesia can produce intolerable side effects at doses required for pain relief, (3) pain higher up the body can be difficult to control without systemic side effects when using a spinal catheter, and (4) it is much less expensive and does not require continuous follow-up care.
Cordotomy technique
The technique of percutaneous cervical cordotomy has been previously described in the neurosurgical literature.4,5 We have used computer tomography to help guide the approaching needle through the neck and into the anterolateral cord. Infusion of a contrast agent into the subarachnoid space helps outline the cord prior to puncturing it. Local anesthesia is used for the needle penetration through the muscles of the neck and a bolus of Propofol for the cordotomy lesion. The lesioning electrode (Rosomoff) can be used for physiologic confirmation of positioning prior to lesioning. Macrostimulation (50 Hz, 1 ms, <1.0 V) should produce a sensation of pain or temperature in the desired region of the body. Macrostimulation (2 Hz, 1 ms, 1.0 V) should not produce ipsilateral muscle contractions unless the electrode is too close to the corticospinal tract. The final lesion(s) are made incrementally until the desired body area has lost its ability to distinguish sharp from dull (pain) or hot from cold (temperature).
Postoperative care
After a few hours of observation, all our patients returned to the palliative care ward. The pain relief following cordotomy is immediate and care must be taken to ensure appropriate opioid reduction. Typically patients no longer ask for prn doses of pain medications, which is an effective titration down, however all patients had their regular opioid dose reduced by 50% immediately postoperatively as a precaution. The regular doses continued to be reduced as tolerated based on levels of drowsiness and acceptable levels of pain. None of our patients required withholding of doses of opioids or the use of naloxone as would be necessary in patients who were not rousable and had respiratory depression. It should be noted that, as in the case of our patient with hepatocellular carcinoma, there is a risk of developing symptoms of withdrawal if titrated down too quickly.
Cordotomy complications
In our very small cohort of patients there have been no major complications such as permanent motor weakness. There are many potential complications, however, that can follow percutaneous cervical cordotomy.16–18 Of foremost concern is unintended damage to the spinal cord causing death from respiratory arrest or hemiplegia from injury to the corticospinal or other descending motor tracts. Ondine's curse and urinary incontinence are unusual following unilateral surgery unless the contralateral functioning has been compromised by the underlying malignancy. CSF leak with resultant low-pressure headaches is a possibility as is local infection in the immune compromised cancer patient. We have not seen loss of pain relief or the development of neuropathic pain, but our patients have not lived long postoperatively.
All patients complained of neck pain postprocedure described as either a stinging sensation or stiffness related to the positioning in the scanner. In the case of our patient with breast cancer, neck pain persisted, but in the other three cases the duration was only a few days.
There were some unanticipated outcomes observed by the team in the weeks following cordotomy. Once the refractory pain was relieved and the opioids dramatically reduced, all the patients had increased clarity of thought. This was felt by most to be beneficial, but in the case of our gentleman with the melanoma, he became increasingly distressed related to symptoms of continued bleeding despite maximum embolization as well as odor from the tumor site. Our patient with the renal cell carcinoma showed signs of depression and expressed frustration that she could not be at home. She did become more hopeful once we were able to arrange a transfer to another palliative care unit closer to home so her family could visit more frequently.
Conclusions
Percutaneous cervical cordotomy provides excellent pain relief in the contralateral hemibody. Patients with medically refractory, unilateral nociceptive pain can expect a dramatic reduction in their pain and a concomitant improvement in their quality of life. This operation continues to be rarely utilized in Canada and is in danger of becoming no longer available if the next generation of neurosurgeons is not appropriately trained. A close working relationship should be developed between the palliative care team and their neurosurgeon in order to provide optimal care for their patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.