
Abstract
Abstract
Background:
Heart failure (HF) is associated with a high symptom burden and reduced quality of life (QOL). Models integrating palliative care (PC) into HF care have been proposed, but limited research is available on the outcomes of such models.
Objective:
Our aim was to assess if inpatient PC for HF patients is associated with improvements in symptom burden, depressive symptoms, QOL, or differential use of services.
Methods:
Patients hospitalized with acute HF were randomized to receive a PC consult with follow-up as determined by provider or standard care. Two hundred thirty-two patients (116 intervention/116 control) from a large tertiary-care urban hospital were recruited over a 10-month period. Primary outcomes were symptom burden, depressive symptoms, and QOL measured at baseline, 1, and 3 months. Secondary outcomes included advance care planning (ACP), inpatient 30-day readmission, hospice use, and death.
Results:
Improvements were greater at both 1 and 3 months in the intervention group for primary outcome summary measures after adjusting for age, gender, and marital status differences between study groups. QOL scores increased by 12.92 points in the intervention and 8 points in the control group at 1 month (difference+4.92, p<0.001). Improvement in symptom burden was 8.39 in the intervention group and 4.7 in the control group at 1 month (+3.69, p<0.001). ACP was the only secondary outcome associated with the intervention (hazard ratio [HR] 2.87, p=0.033).
Conclusion:
An inpatient PC model for patients with acute HF is associated with short-term improvement in symptom burden, QOL, and depressive symptoms.
Introduction
E
The field of palliative care (PC) may be well suited to address the needs of HF patients. PC assesses and treats psychological distress and pain and other physical symptoms, and it supports functional status, communicates about care goals, and provides support for complex decision making.14,15 PC has been demonstrated to improve symptom burden, depression, and QOL among patients with cancer.16,17 PC can also facilitate discussions about treatment preferences for end-of-life care that often remain unaddressed. 18 Models and guidelines for integrating PC into HF management have been proposed,7,18–21 including recommendations in the most recent American College of Cardiology/American Heart Association (ACC/AHA) guidelines 22 but studies of their impact on outcomes are needed.
The purpose of this study was to determine whether incorporating PC into inpatient care for HF patients is associated with improvements in health status or use of health services. Specifically, our research questions were: is the provision of PC to HF patients in the inpatient setting associated with 1) differences in QOL, symptom management, or depression? Or is it associated with 2) differences in advance care planning (ACP), 30-day readmission, hospice use, or mortality compared with standard care?
Methods
Setting
This study took place at Abbott Northwestern Hospital (ANW), a 629-bed tertiary-care facility located in Minneapolis, Minnesota, that is part of the Allina Health system of hospitals and clinics. In 2011, ANW had 38,000 inpatient admissions, 366,000 outpatient registrations, and treated 732 patients with a primary diagnosis of HF. The ANW inpatient PC team at the time of the study included four physicians board certified in hospice and palliative medicine, two clinical nurse specialists board certified in advanced practice palliative care nursing, a social worker, and a chaplain. PC providers conducted 1417 initial consults and 5218 subsequent visits to inpatients in 2011. At the time this study was designed, hospital records indicated that PC consults were ordered for only 9.2% of HF inpatients.
Recruitment, randomization, and study sample
Patients were considered eligible for the study if they were adult inpatients with a diagnosis of acute HF. Patients were not eligible if they were in the intensive care unit (ICU), on a ventilator, undergoing evaluation for a heart transplant or a left ventricular assist device (LVAD), post-transplant or post-LVAD, determined to be actively dying, or if they had cognitive impairments such that informed consent and data collection would not be possible or if they spoke limited English. Additionally, patients who had already had a PC order request by their attending physician during the hospital stay were ineligible.
Potentially eligible patients were identified using reports from the electronic health record (EHR). Eligibility was verified by reviewing patient records and talking with a floor nurse if needed. Patients determined to be eligible were visited by the research nurse who explained the study and enrolled patients who were interested in participating. After enrollment and baseline data collection, patients were immediately randomized to the study group and notified of whether they were in the intervention or control group so they would know whether to expect a visit from a PC provider.
Power calculations were done to identify a goal sample size using mean baseline values of summary scores from 26 pilot study patients for each of the three study data collection instruments. Calculations assumed an α of 0.05 and 80% power. Results indicated a total sample size of 500 (250 per group) would be sufficient to detect an effect size (Cohen's d) of 0.25, which equates to a minimum detectable mean differences between intervention and control groups of 1.5 points in the Patient Health Questionnaire-9 (PHQ-9), 6.4 points in the Minnesota Living with Heart Failure (MLHF) Questionnaire, and 3.3 points in the Edmonton Symptom Assessment Scale (ESAS).
Patient recruitment began in April 2012 and ended in February 2013. Of the 822 patients screened, 547 were eligible and 470 (86%) were approached. Of those approached, 232 were enrolled (49%) (Fig. 1). Of the 116 intervention patients, 4 withdrew from the study at the time the provider came to the room because they changed their mind. An additional 11 intervention patients did not receive the intervention because the PC team was unable to conduct the consultation prior to the patient's discharge. Thus 13% of those initially randomized to the intervention group did not get the intervention. There were 19 deaths during the study period and 14 withdrawals from the study. Most of the withdrawals came in the form of refusals to respond to mailed surveys. Because PC could not ethically be withheld from subjects, n=8 patients in the control group received inpatient PC consults via standard care.
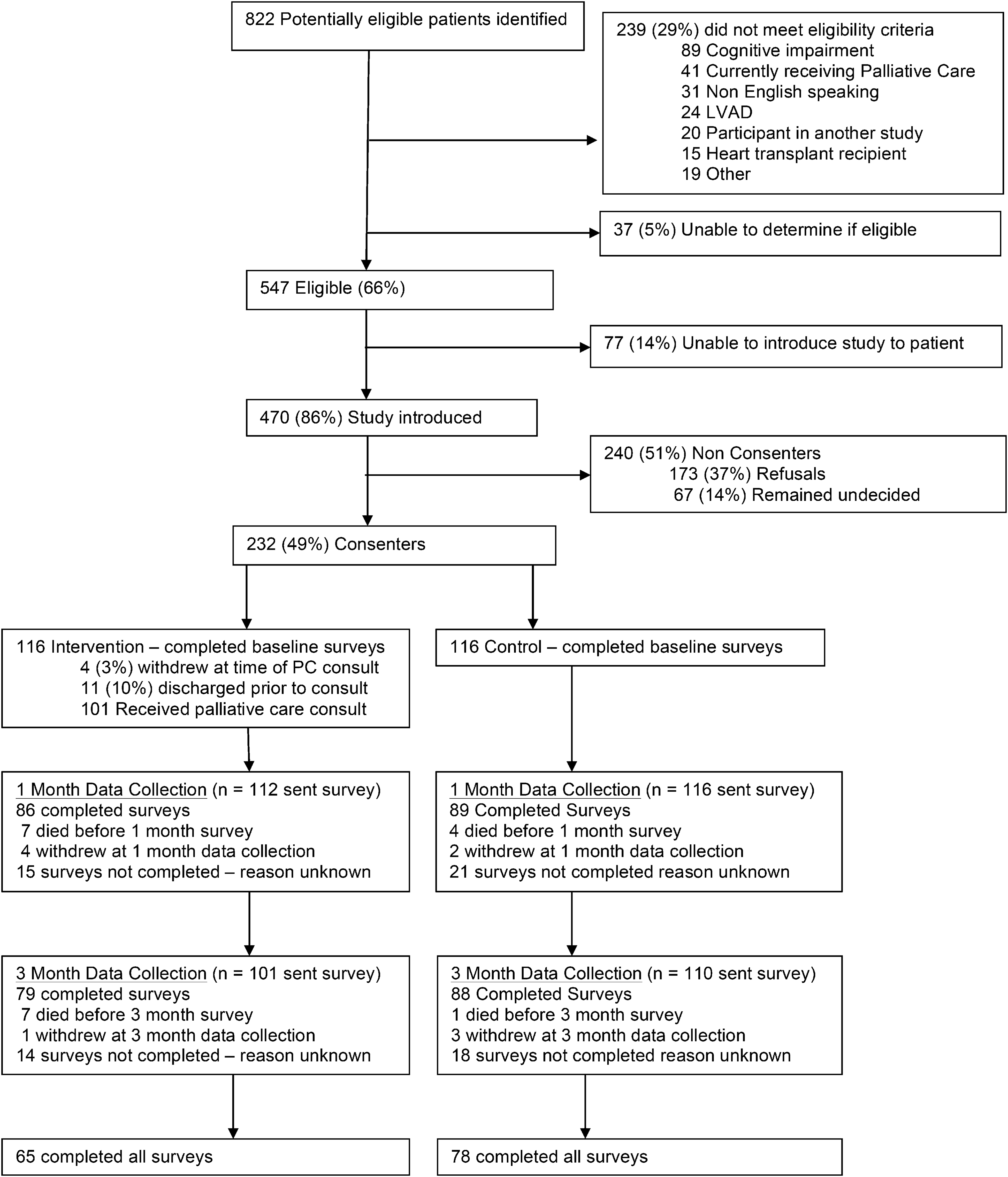
Recruitment, enrollment, retention, and data collection.
Intervention
The intervention followed the standard process of the hospital PC team. After patients were randomized to the intervention group, an order for PC was immediately entered, and triaged by the PC team with a goal of conducting the PC consult within 24 hours of the order. Providers did an initial consult and then determined whether further appointments were necessary and discussed that with the patient. The study intervention differed from the standard PC process in two ways. First, baseline study measures of symptom burden, depression, and QOL were available to the providers to review at the time of the consultation. Second, the study paid only for the initial PC consultation and any subsequent visits were billed to the patient's insurance as standard care. This information about billing was shared with patients during the consent process. Actions of PC providers during visits generally included assessment of symptom burdens; emotional, spiritual, and psychosocial aspects of care; coordination of care orders; recommendations for change in current or future treatment; referrals; and future care planning assessment and discussions.
The comprehensive ACP process examined as an outcome was not conducted by the PC providers but may have been introduced and encouraged as part of the PC consult. All HF patients receive a referral to the ACP process through their discharge orders. Those who had not completed the process received a call postdischarge offering the ACP process. The ACP process, described in detail elsewhere, 23 is often referred to as disease-specific ACP. This version of ACP uses a trained facilitator to guide communication between patients and their caregivers regarding patient values and goals for treatment in specific scenarios related to progression of their disease. The process usually takes place in their home with their family members who may serve as proxies for future health care decisions. The process includes completion of a health directive, a disease-specific plan and goals that are documented in the medical record, and identification of needed resources.
Data collection
This study and use of patient data for this project was approved by the Allina Health Institutional Review Board. Study data came from two sources: patient self-reported measures and EHR data. Self-reported measures were collected using three questionnaires to assess depression, QOL, and symptom burden. Baseline self-reported measures were collected by the research nurse at the time of enrollment either by allowing the patient to complete the questionnaires themselves or by reading aloud the questions to the patient and completing the forms depending on patient preferences. The same questionnaires were administered via mailed surveys at 1 and 3 months after enrollment. Patients who did not return mailed surveys within a week after the 1- or 3-month follow-up date were called by the research nurse and encouraged to return the survey or were offered the option to complete the survey over the phone. Up to three follow-up phone calls were made.
EHR data were extracted after the study was complete. Each participant had an order indicating study participation and randomization outcome. Outcome measures from the EHR were excluded for the patients who withdrew from the study, depending on time of withdrawal.
Data measures and definitions
The ESAS was used to measure symptom burden, the PHQ-9 assessed depression symptoms, and the MLHF was used to measure QOL. The ESAS 24 was created to assess symptoms of patients receiving PC. The ESAS rates ten symptoms (pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, well-being, shortness of breath, and “other”) using a visual scale line with labels of “none” at 0 and “worst possible” at 10. The scores from each of the first nine items are combined to create a summary distress score. The instrument showed positive results for internal consistency, criterion, and concurrent validity as well as test-retest correlation at 1 day.24,25 The ESAS is recommended for use with HF patients. 19
The PHQ-9 is a brief, validated instrument used widely in clinical and research settings to assess risk for depression.26,27 The PHQ-9 has been used in research on HF patients.28,29 PHQ-9 questions address the previous 2 weeks and ask about physical and mood symptoms of depression that align with diagnostic criteria. Responses indicate how often symptoms were experience and each item is scored from 0 (“not at all”) to 3 (“every day or nearly every day”).
The MLHF Questionnaire 30 was created to be representative of the ways HF and treatments can affect key physical, emotional, social, and mental dimensions of QOL. The instrument has high reliability for repeated measures, internal consistency, and high reliability between in-person and telephone data collection.30–32 The MLHF contains 21 items that assess how much a person's HF has affected many aspects of their life during the prior month. Responses range from 0 (“no”) to 5 (“very much”). In addition to a summary score, the instrument has physical dimension and emotional dimension scores.
For all three instruments and individual components of the instruments, we calculated change from baseline to 1 month and baseline to 3 months by subtracting the follow-up value from the baseline value. For all of the instruments we used, a higher number is an indication of worse severity in the measure. A positive value for the calculated change from baseline indicates an improvement in that measure since baseline while a negative value in the change measure would indicate a worsening in the severity of that measure.
Readmissions were defined as an inpatient readmission for any cause within 30 days; hospice use was any hospice admission within 6 months. ACP was defined as documented completion of the disease-specific ACP process in the record within 6 months of the study hospitalization.
Data extracted from the EHR included patient characteristics (age, gender, race, marital status, prior recent hospitalizations as a measure of disease severity), measures of the intervention (number of PC visits, date of PC consultation), and secondary outcomes (ACP, readmissions, mortality, and hospice use). Mortality and hospice data were also collected from the study patient tracking database as these were sometimes identified when calling patients to follow up on surveys.
Analysis
All analysis was conducted using SPSS version 18 (SPSS Inc., Chicago, IL). Analysis used an intention-to-treat model including all patients regardless of amount of intervention received. Baseline values were compared between the study groups using χ2 tests for categorical measures and t tests to compare mean values of continuous measures. The comparison of change from baseline to the follow-up periods was conducted using general linear regression models with adjustment for age, gender, and marital status. Survival analysis using proportional hazards regression was conducted to examine outcomes of 30-day inpatient readmissions, ACP completion, hospice admission, and mortality (all within 6 months). These models were adjusted for age, gender, and marital status. Analysis on ACP completion excluded people who had already completed the process prior to the study.
Results
Baseline demographics were comparable across the study groups with the exception of age (Table 1). Patients in the intervention group were on average 5.1 years older than patients in the control group. Inpatient and emergency department admissions and total inpatient length of stay in the 6 months prior to the study were compared as proxy measures for disease severity, but no differences were found between the two groups for these measures. Additionally, there were no differences at baseline between the groups on the three primary outcome summary measures. Individual symptom components from the ESAS were examined as well and the only measure with different baseline results was tiredness, with the mean being 0.8 points higher in the intervention group (p=0.03).
ESAS, Edmonton System Assessment Scale; IP, inpatient; LOS, length of stay; PHQ-9, Patient Health Questionnaire-9; MLHF, Minnesota Living with Heart Failure Questionnaire; SD, standard deviation.
Among the 101 patients receiving the PC intervention, 80 received 1 visit from the PC team, 13 received the initial consult plus 1 additional visit, and 8 received a total of 3 or more visits. Some patients were referred to receive visits from the team social worker (n=10) or chaplain (n=5) in addition to visits from the PC provider.
Outcomes at 1 and 3 months show larger improvement on all three summary outcomes in the intervention group than the control group after adjustment for age, gender, and marital status (Table 2). The mean change in the intervention group was 3.69 points more than that in the control group on the ESAS Distress score at 1 month and 4.31 points higher at 3 months. Symptoms showing statistically significant improvement include shortness of breath, anxiety, and tiredness at both time periods and pain at 3 months only. Shortness of breath and tiredness had the largest improvement compared with the control group. The PHQ-9 summary score was significantly different at both times with a 1.42-point higher improvement in the intervention group compared with the control group at 1 month and 0.72 points at 3 months. None of the individual items showed significant differences between the two groups.
Calculated as baseline minus 1 month or 3 month scores. Positive number indicates improvement since baseline and negative indicates worse condition than baseline.
CI, confidence interval; PHQ-9, Patient Health Questionnaire-9.
The intervention group improvement on the MLHF total score was 4.92 points higher than in the control group at 1 month and 3.06 points higher at 3 months. At 1 month, the biggest difference was in the physical subscale, which improved 3.51 points more in the intervention group, whereas the emotional difference was 0.96. At 3 months, the emotional score change was 1.72 points higher and the physical score change was 1.2 points higher in the intervention group compared with the control group.
When change in total summary scores (Table 2) was examined as a percent of the total mean baseline values (in Table 1), the percent of additional improvement from baseline experienced by the intervention group was 11% for the ESAS (3.69/32.7), 17% for PHQ-9, and 10% for the MLHF.
Results of the survival analysis (Table 3) found no significant associations between study group assignment and 30-day inpatient readmission, hospice use, or death within 6 months after adjustment for age, gender, and marital status. Those in the intervention group were 2.87 times more likely to have completed the disease-specific ACP process within 6 months.
The hazard ratios (HR) are adjusted for age, sex, and marital status.
CI, confidence interval.
Discussion
This study contributes to the growing literature reporting that PC may improve symptom burden, depression, and QOL. Specifically, this study found significant associations with inpatient visits and improvements in summary measures for the three outcomes over a short time period in HF patients.
The differences identified in the current study are from an intervention conducted in the context of short lengths of stay in an inpatient setting with many patients receiving only one visit with the PC provider. As such, the significant results at 1 and 3 months are promising for the role of inpatient PC for HF patients. However, it is unclear on how changes of these levels translate into experiences of patients. An improvement of 5 points in the MLHF has been identified as clinically meaningful.30,33 The 1-month study mean difference of 4.92 approaches this level. A decline of 5 points in the PHQ-9 is considered a clinically meaningful response to treatment for depressed patients. 34 Our study found an increased improvement of 1.42 in the intervention group, which represents all participants regardless of depression status.
To date, research on the integration of PC for HF has occurred primarily in outpatient settings35–37 with a few inpatient studies focused on feasibility.38,39 One outpatient study 37 reported a 2.9-point greater improvement in the ESAS Distress score in the intervention group at 3 months, which is comparable to the 3.7 point (1 month) and 4.3 point (3 months) improvement observed in our study. The same study demonstrated mean improvement in the PHQ-9 to be 4.4 points higher in the intervention group, which is slightly higher than the 1.4 and 0.7 differences reported here at 1 and 3 months. The baseline averages for the PHQ-9 in the outpatient study were notably higher than ours however (14.2/14.5 versus 8.6/8.1 in the current study). The MLHF improvement in the outpatient study (5.6 points more in intervention) are comparable to the differences of 4.9 at 1 month and 3.1 at 3 months in the current study. The average age of study participants in the outpatient study was 53.6 whereas ours was 73.4, and this stark age difference should be considered when comparing results. However, both studies generally provide evidence that PC visits likely improve symptom burden in either setting.
In addition to the role of PC in addressing specific symptoms burdens, PC is well known for eliciting goals of care, and helping patients and their caregivers with complex medical decision making. 14 For HF patients, ACP is one tool to help patients in this process. 23 A referral to ACP is a standard part of the discharge order set for HF patients at this institution but may not be sufficient to result in participation without a discussion about the process. Indeed, results indicate patients in the intervention were more likely to complete the ACP process after discharge, most likely based on discussions about the ACP process and recommendation from the PC provider during the intervention. Completion of the ACP process focuses on enabling proxies to be able to make decisions in alignment with patient preferences and documents more detailed preferences in the medical record than could be done with a typical advance directive. Completion of the ACP process for HF patients is also associated with increased hospice use at the end of life. 23
One of the challenges to implementing the current study was limited PC provider time. This resulted in some patients assigned to the intervention group not receiving a PC consult and also prohibited the study team from incorporating outpatient PC follow-up visits into the intervention. The study was stopped before reaching the desired sample size because of increased referrals to PC as part of usual care in the hospital. Future models may benefit by combining inpatient and outpatient PC. Advantages of outpatient follow-up care include: follow-up on medical orders or referrals started in the inpatient setting, establishing the relationships with patients and families that enable comprehensive ACP, and improved patient contact to assess changes in symptoms. A model that combines inpatient and outpatient PC delivery would build on prior work supporting the association of outpatient PC with improved symptom burden for a variety of conditions.36,37
Limitations
There are several limitations to this study that should be considered when interpreting results. First, by not achieving the original intended sample size of 500 subjects, the study may be underpowered and the randomization process may not have sufficiently distributed patient characteristics evenly between study conditions. We were able to adjust analysis for the characteristics we could measure, but there may be additional differences that we were not able to measure or address in the analysis. Second, the intervention effect may have been attenuated by the patients assigned to PC who did not ultimately receive the intervention, either because they withdrew or because the PC team did not conduct the consult due to work load. Additionally, a subset of control patients (8) received some PC during the study hospitalization. These limitations are the product of conducting research in an applied setting.
Losses to follow-up resulted from patient withdrawal, death, and nonresponse to the survey. It is unknown how this may have altered outcomes. Additionally, in assessing readmission and hospice use, we were limited to information on readmissions that took place within our health system, were documented by providers within our system, or were identified by the research nurse during follow-up calls. It is possible that patients were admitted to hospitals or hospice care external to our health system, and it is not possible to know whether the distribution of missing information on health services outside our system was evenly distributed across the study conditions.
Conclusion
This study contributes to the growing evidence that PC may improve symptom burden, depressive symptoms, and QOL in HF patients. The study also provided evidence that interactions with PC providers were associated with increased participation in ACP. Further research is needed to determine how best to provide PC to HF patients in a coordinated manner across both inpatient and outpatient settings in ways that achieve clinically meaningful long-term improvement in symptom burden, depression, and QOL.
Footnotes
Acknowledgments
This study was funded by the Abbott Northwestern Hospital Foundation.
The authors gratefully acknowledge the members of the ANW Palliative Care team for incorporating visits with study patients into their schedules and serving patients.
Author Disclosure Statement
No competing financial interests exist.