
Abstract
Abstract
Background:
Consciousness is an important factor of survival prediction in advanced cancer patients. However, effects on survival of changes over time in consciousness in advanced cancer patients have not been fully explored.
Objective:
This study evaluated changes in consciousness after admission to a palliative care unit and their correlation with prognosis in terminal cancer patients.
Methods:
This is a prospective observational study. From a palliative care unit in Taiwan, 531 cancer patients (51.8% male) were recruited. Consciousness status was assessed at admission and one week afterwards and recorded as normal or impaired.
Results:
The mean age was 65.28±13.59 years, and the average survival time was 23.41±37.69 days. Patients with normal consciousness at admission (n=317) had better survival than those with impaired consciousness at admission (n=214): (17.0 days versus 6.0 days, p<0.001). In the analysis on survival within one week after admission, those with normal consciousness at admission had a higher percentage of survival than the impaired (78.9% versus 44.3%, p<0.001). Patients were further classified into four groups according to consciousness levels: (1) normal at admission and one week afterwards, (2) impaired at admission but normal one week afterwards, (3) normal at admission but impaired one week afterwards, and (4) impaired both at admission and one week afterwards. The former two groups had significantly better survival than the latter two groups: (median survival counted from day 7 after admission), 25.5, 27.0, 7.0, and 7.0 days, respectively.
Conclusion:
Consciousness levels one week after admission should be integrated into survival prediction in advanced cancer patients.
Introduction
A
Deterioration of consciousness near death has been previously reported. 8 However, in most studies, consciousness was evaluated at admission or registration.4–7 Little is known about the impact on survival of changes in consciousness over time. This study investigated the impact of changes in consciousness status after admission on survival in advanced cancer patients.
Methods
Patients and palliative care setting
Consecutive advanced cancer patients who were admitted to the palliative care unit of the National Taiwan University Hospital between October 2002 and December 2003 were recruited. Patients were divided into two categories according to consciousness level: normal (alert) and impaired (including lethargic, obtunded, delirious, stupor, or comatose). Patients were under active total care provided by a multidisciplinary team comprised of physicians, nurses, psychologists, social workers, clinical Buddhist chaplains, and volunteers.
Data collection
The condition of all patients during admission was reviewed daily by the same staff member who assessed and recorded consciousness status. Patient demographic and diagnostic data were obtained from routine medical records. The consciousness levels were assessed at the time of admission and one week after admission. The study was approved by the ethical committee of the National Taiwan University Hospital, and written informed consent was obtained from the participants or surrogates before their inclusion in the study.
Statistical analysis
Consciousness levels and changes at different time points are illustrated in the consort diagram (see Fig. 1). We identified groups comprising representative numbers of people with consciousness data at admission and one week after admission. Chi-square test was used to examine if consciousness status was associated with dying within one week after admission. Two models of the Kaplan-Meier survival analysis and the log-rank test were used to examine survival-length differences among consciousness groups. Cox proportional hazards survival analysis was used to adjust for dyspnea, anorexia, fatigue, the Eastern Cooperative Oncology Group (ECOG) score, and edema among the consciousness groups at the time of admission and one week after admission. A probability of less than 0.05 (p<0.05) was considered statistically significant. Data were analyzed using SPSS 11.0 (SPSS Inc., Chicago, IL).

Consciousness status and subgroups at admission and one week after admission.
Results
We enrolled 531 terminal cancer patients, 275 (51.8%) males and 256 (48.2%) females, in this study. The mean age was 65.28±13.59 years. The lung was the most frequent primary cancer site (20.2%), followed by the liver (17.7%) and colon/rectum (10.0%). The average survival time was 23.41±37.69 days (see Table 1).
Among the 317 patients in the normal group, 146 maintained normal consciousness and 60 became consciously impaired one week after admission; 61 expired and 50 were missing. In those missing patients of the normal group, 22 were discharged within one week, 21 without consciousness data and 7 without survival data. Among the 214 patients in the impaired group, 20 patients returned to normal consciousness, 64 still showed consciousness impairment one week after admission, 113 expired, and 17 were missing. Of those missing patients in the impaired group, 8 were discharged within one week, 6 without consciousness data and 3 without survival data (see Fig. 1).
In survival analysis, we initially examined differences in survival length and mortality hazard ratios between the patients with normal consciousness and those with impaired consciousness, both at admission. Kaplan-Meier survival analysis showed that the median survival length after admission was 17.0 days (95% confidence interval [CI]: 14.4–19.6) and 6.0 days (95% CI: 5.0–7.0) for those with normal consciousness and those with impaired consciousness at admission, respectively. The log-rank test showed that patients with normal consciousness at admission had a significantly longer survival time than those with impaired consciousness (χ2=71.12, p<0.001) (see Fig. 2a). Cox proportional hazard survival analysis indicated that the mortality hazard ratio for patients with impaired consciousness at admission was 1.71 (95% CI: 1.37–2.12, p<0.001) that of the patients with normal consciousness at admission, after adjusting for ECOG, fatigue, dyspnea, anorexia, and ascites (see Table 2, upper part).
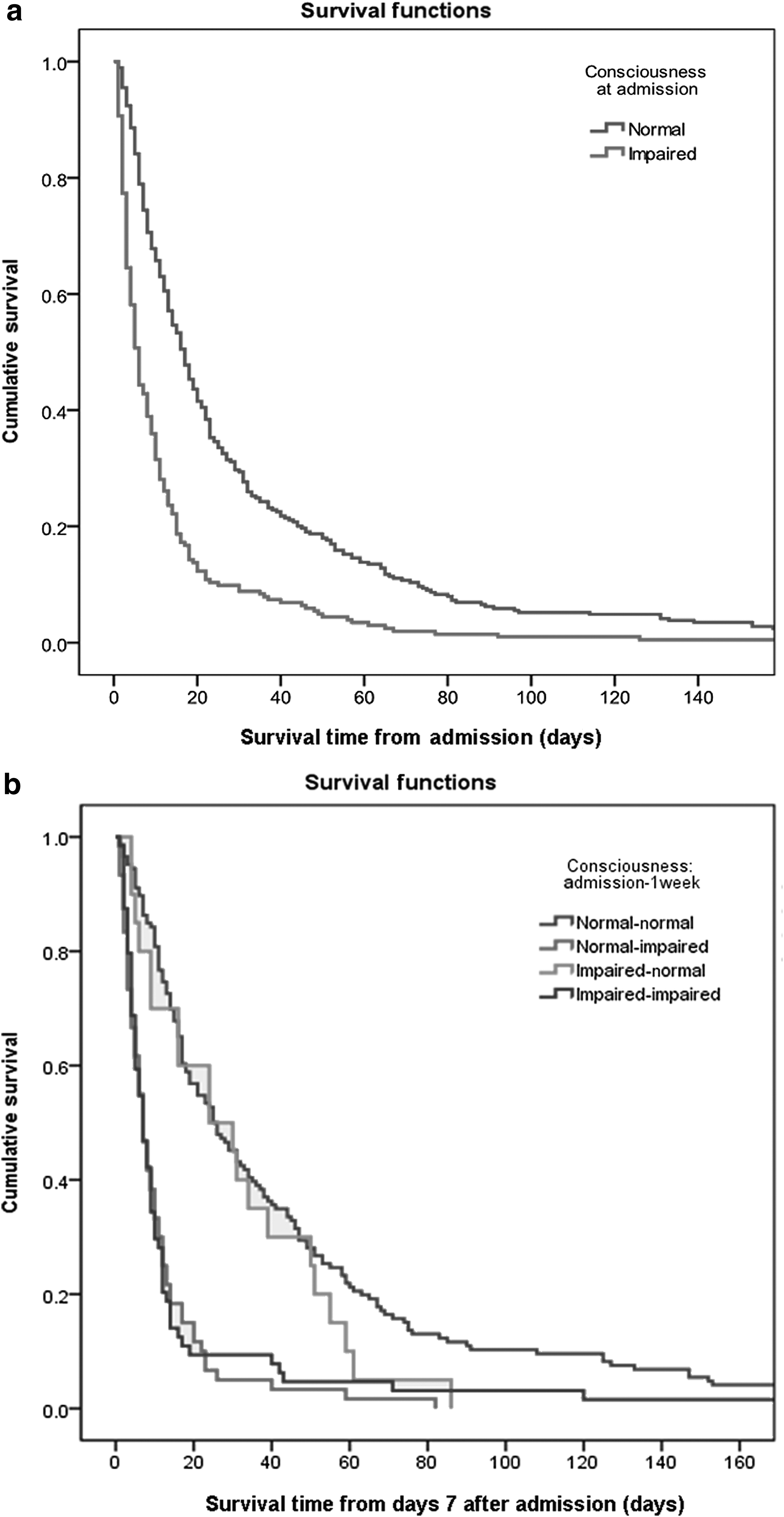
Kaplan-Meier survival analysis.
The following variables were entered as covariates at the time of admission: dyspnea, anorexia, fatigue, ECOG, and edema.
1: Group 1; 2: Group 2; 3: Group 3; 4: Group 4; 5: Group 5; 6: Group 6.
CI, confidence interval; HR, hazard ratio.
In analysis on survival within one week after admission, the chi-square test showed that those with normal consciousness at admission had a higher percentage of survival than the impaired (78.9% versus 44.3%, χ2=62.30, p<0.001; data not shown).
Furthermore, we analyzed the survival time one week after admission (follow-up time starts at day 7 after admission) and also the mortality hazard ratio based on status change one week after admission. The Kaplan-Meier analysis revealed that the median survival (counted from day 7 after admission) was 25.0 days (95% CI: 17.9–32.2) for the patients with normal consciousness both at admission and one week after admission (normal-normal), 7.0 days (95% CI: 5.1–8.9) for patients with normal consciousness at admission but impaired consciousness one week after admission (normal-impaired), 24.0 days (95% CI: 3.5–44.5) for the patients who had impaired consciousness at admission but normal consciousness one week after admission (impaired-normal), and 7.0 days (95% CI: 4.9–15.3) for patients who had impaired consciousness both at admission and one week after admission (impaired-impaired). The log-rank test showed no statistical difference between the normal-normal group and the impaired-normal group (χ2=1.27, p=0.260). Nevertheless, significant differences were found between the normal-normal group and the normal-impaired group (χ2=66.28, p<0.001) as well as between the normal-normal group and the impaired-impaired group (χ2=51.39, p<0.001). In addition, no difference was found when comparing the normal-impaired group and the impaired-impaired group (χ2=0.06, p=0.809) (see Fig. 2b).
After adjusting for ECOG, fatigue, dyspnea, anorexia, and ascites, Cox proportional hazard survival analysis revealed that the mortality hazard ratios for patients in the normal-impaired group and patients in the impaired-impaired group were 3.22 (95% CI: 2.29–4.53, p<0.001) and 3.17 (95% CI: 2.20–4.57, p<0.001) that of the hazard ratio for patients in the normal-normal group, respectively. However, no difference was found when comparing the hazard ratios between patients in the normal-normal group and patients in the impaired-normal group: 1.25 (95% CI: 0.75–2.10, p=0.239) (see Table 2, lower part).
Discussion
We have demonstrated that survival was better in advanced cancer patients with normal consciousness at admission than in those with impaired consciousness at admission. To the best of our knowledge, this is the first study to show that consciousness levels one week after admission to a palliative care unit are important for survival prediction in advanced cancer patients.
The consciousness level is an important prognostic factor for survival in most prediction tools.5–7 In most of the previous studies, prognostic factors for survival prediction are evaluated at a single time point, such as admission or case registration, except for two recent studies that demonstrated that changes in functional performance during the disease trajectory are potentially useful for survival prediction.9,10
Our previous studies have demonstrated that a majority of symptoms in advanced cancer patients with survivals of two to three weeks improved one week after admission to a palliative care unit.11,12 Thus, one week after admission is a critical time point for far-advanced cancer patients. In this study, patients whose consciousness levels deteriorated one week after admission had poorer prognoses than patients whose consciousness was impaired at admission but recovered within one week after admission. This suggests that an initial normal consciousness level alone does not accurately predict prognosis and that changes in consciousness after admission must be taken into account for survival predictions.
One of the major limitations of our study is the missing data. Among the total of 67 patients with missing outcomes, 30 (44.8%) patients were censored because of discharge from the hospital within one week. Possible causes of discharge included patients having stable conditions or impending death. Families and patients often wish to die at home, a Taiwanese custom of breathing the last breath at home. 13 Unable to control terminal symptoms at home, many families choose to have the patient discharged only when the death is very near. 14 Future studies could draw on the death registry to compensate for the censored data and address this limitation.
There are some other limitations in this study. First, this study was conducted in Taiwan, so patterns of origins and prevalence of cancers might be different from those in other countries. Second, origins of cancers enrolled in this study were mainly solid organs. Hematologic malignancies were less discussed. Thus, further large-scale studies are warranted.
In conclusion, not only consciousness at admission, but also changes in consciousness after admission to a palliative care unit significantly affected the survival of advanced cancer patients. The consciousness level at admission and the consciousness levels one week after admission to a palliative care unit should be integrated for survival prediction of advanced cancer patients.
Footnotes
Acknowledgments
The authors are indebted to the participants and the faculty of the Department of Family Medicine at the National Taiwan University Hospital for their full support of this study. This study was supported by the National Science Council (NSC 91-2314-B-002-224), the Department Of Health (DOH92-HP-1506), and the National Health Research Institutes (NHRI-102A1-PDCO-0100028), Executive Yuan, Taipei, Taiwan.
Author Disclosure Statement
No competing financial interests exist.