
Abstract
Abstract
Background:
Nonsteroidal anti-inflammatory analgesics (NSAIDs) are useful in cancer pain but the specific use of subcutaneous parecoxib has not been previously reported.
Objective:
This pilot study aimed to establish the efficacy and side effect profile of short-term sequential single daily dose subcutaneous parecoxib sodium in patients with severe cancer bone pain.
Methods:
Nineteen hospitalized patients with advanced cancer and uncontrolled malignant bone pain (9 males, 10 females) received 24 courses of one, two, or three days sequential therapy with ‘off-label’ daily subcutaneous parecoxib. All patients were receiving opioid therapy; the median baseline daily oral equivalent dose (OED) of morphine was 180 mg. Pain was assessed at baseline, 24 hours, 48 hours, and 72 hours. Pain scores as assessed on an 11-point numeric pain rating scale (NPRS), any side effects including subcutaneous site reactions, as well as patient satisfaction rating with analgesia were recorded. A clinically significant decrease in pain scores was defined as a reduction of two or more points on the NPRS.
Results:
Median pain score of all patient treatments decreased from 7 to 4.5 at 24 hours (p<0.001) and 4.0 at 48 hours. A response was seen in 17 (71%) of the 24 treatments at 24 hours. There was no difference between median negative change in pain scores in 19 (79%) treatments where pain was either strongly movement related, or in 22 (94%) treatments where local bone tenderness was more pronounced. No major side effects were observed during treatment. One patient died from pulmonary embolism after cessation of concurrent prophylactic low molecular weight heparin prior to staging liver biopsy. Subcutaneous site reactions occurred in 2 (8%) treatments and were mild and self limiting.
Conclusions:
Short-term daily subcutaneous parecoxib injection was effective for malignant bone pain when added to existing analgesic therapy and was well tolerated. Further research is warranted into the short-term use of parecoxib in hospitalized patients with intractable malignant bone pain.
Introduction
P
The European Medicines Agency granted a marketing authorization, valid throughout the European Union, for parecoxib sodium in March 2002. 7 It is usually given in an initial dose of 40 mg, followed by further doses of 20 mg or 40 mg as required every 6 to 12 hours, with a maximum dose of 80 mg a day. The Agency recommendations are for short duration of treatment and the lowest effective dose of this agent. At the time of writing, parecoxib had received regulatory approval for use in the European Union and 74 other countries (including Australia) for perioperative analgesia. It is not available in the United States or Canada. Parecoxib was first approved by the Australian government Department of Health Therapeutic Goods Administration in May 2002, 8 and over 2050 doses annually are administered to surgical patients perioperatively in our metropolitan regional health network, most commonly as a single intravenous dose.
The drug has little or no effect on platelet function2,6 and its longer duration of action and reduced gastrointestinal risk compared with ketorolac tromethamine is considered advantageous in the postoperative setting. We postulated that this agent may also be useful in limited dose by daily subcutaneous injection for severe cancer pain, specifically malignant bone pain, and may offer some advantage in achieving more rapid pain reduction in selected patients.
Bone cancer pain is common in patients with advanced breast, prostate, and lung cancer in particular; and once tumors metastasize to bone, they are a major cause of morbidity. 9 The resultant pain can have a devastating effect on the quality of life.10,11 Recent research suggests there are both neuropathic and inflammatory nociceptive components of bone cancer pain12–14 and if pain is unrelieved, it may become chronic. 12 Nonsteroidal anti-inflammatory agents (NSAIDs) or COX-2 inhibitors remain widely used to target the somatic component of bone pain.13,14 Ketorolac tromethamine, a potent injectable nonselective cyclo-oxygenase inhibitor, was first introduced in 1986 for postoperative analgesia 15 and still remains in current use. 16 Blackwell 17 first described the short-term use for cancer pain of ketorolac by subcutaneous infusion. Subsequent small case series18–20 and an uncontrolled study of ketorolac combined with an opioid and ketamine 21 reported efficacy for cancer pain. The risks of adverse gastrointestinal and renal side effects with ketorolac are well described and limit its use. 22
To our knowledge, there have been no previously reported clinical studies describing the use of parecoxib sodium in cancer pain. There is, however, mention of parecoxib administered by continuous subcutaneous infusion for pain at the end of life in adult patients in the Northern Ireland palliative care guidelines. 23 One of the authors 24 had previously used short-term daily subcutaneous parecoxib, with good efficacy and tolerability, in 10 patients with malignant bone pain in a private palliative care unit setting. This study describes the results of short-term ‘off-label’ sequential daily subcutaneous parecoxib sodium in patients with severe bone pain when added to existing opioid and adjuvant analgesic therapy.
Methods
Ethics approval for the study was requested and granted by the Eastern Health Human Research Ethics Committee (LR52/1112). The project was conducted in an urban teaching health network and involved the 30-bed inpatient palliative care unit and the oncology unit of two acute hospital campuses, one of 400 beds and the other of 200 beds. The study involved three palliative care consultants (DJK, SB, SLF) and the team registrars at the palliative care unit or acute campuses. All patients were in hospital, had been either referred to the palliative care service for pain control or admitted to the palliative care unit, and gave informed consent to participate in the study. The study was conducted over a 12-month period between November 2011 and November 2012. The key inclusion criterion was severe uncontrolled malignant bone pain despite current opioid and adjuvant therapy. The occasional short-term use of the potent nonselective COX inhibitor ketorolac tromethamine by subcutaneous infusion is accepted practice in our service, and these selected patients were those in whom we would otherwise have considered ketorolac. Exclusion criteria were gastrointestinal bleeding or active peptic ulceration; acute renal failure; severe hepatic failure; coexistent ischemic heart or peripheral vascular disease; previous asthma; and allergic reactions to aspirin, NSAIDs or COX-2 inhibitors, or sulphonamides.
Nineteen patients with advanced malignancy and severe uncontrolled bone pain were selected to receive parecoxib. Between one and up to three doses of either 40 mg (or 20 mg if body weight less than 50 kg) of parecoxib sodium were administered as a single daily subcutaneous injection. Fourteen courses of treatment occurred in one or other of the two oncology wards and ten courses of treatment in the inpatient palliative care unit.
One patient received three courses of parecoxib treatment during three separate hospital admissions; 3 patients received two courses; and the majority, 15 patients, received one course of treatment. Treatment consisted of a single injection in three treatments, two injections in two treatments, and three consecutive daily injections in the remaining 19 treatments. The study design allowed for up to three days' therapy with parecoxib, although early discharge from hospital (two treatments), transfer to another hospital (one treatment), unexpected death (one treatment), and unknown (one treatment) resulted in reduced treatment duration in these patients. Parecoxib was administered via a previously sited 25G (BD Saf-T-Intima,™ Becton, Dickinson) subcutaneous catheter and the injection site was monitored daily for any reaction over the observation period.
Self-assessed pain scores were reported on an 11-point Likert numeric pain rating scale (NPRS) at baseline, 24 hours, 48 hours, and 72 hours post initial treatment injection and recorded by the palliative care service registrar at each campus. Overall patient satisfaction with treatment was also recorded on a five-point Likert rating scale, from ‘very unsatisfied’ to ‘very satisfied.’
Statistical analysis
The data were analyzed according to an intention-to-treat approach. The Kolmogorov-Smirnoff test for normality confirmed that pain variables were not normally distributed. Nonparametric tests (Wilcoxon signed-rank test) were performed on the pain scores using SPSS 21.0 (IBM, Armonk, NY). Furthermore, a repeated measures analysis, mixed-design (Split-Plot) ANOVA, was carried out on the data, using SPSS 20.0. Statistical significance for this clinical study was set at p<0.05.
Results
All patients had uncontrolled pain despite opioid and nonopioid therapy, with 22 of 24 (92%) patient treatments having an unstable opioid dose in the two weeks prior to treatment. Demographic data, primary diagnosis, site of metastases, performance status, predominant site of current pain, previous and current analgesic therapy, and details of past radiotherapy were recorded. In 17 (71%) treatment episodes pain involved the spine and in 7 (29%) episodes, the extra-axial skeleton (see Table 1).
Mean age, years±SD=64±16 (range 35–89).
GORD, gastroesophageal reflux disease; IQ, interquartile range; KPS, Karnofsky Performance Status; NPRS, numeric pain rating scale; NSAID, nonsteroidal anti-inflammatory analgesic; OED, oral equivalent dose; PPI, proton pump inhibitor.
The results of treatment are summarized in Figures 1A, 1B, 2, and 3. The median (IQ range 25%–75%) patient survival time from first injection of parecoxib was 47 (21–122) days (range 1–300 days). Pain scores at 24 and 48 hours posttreatment with parecoxib fell in 17 (71%) of 24 treatments by a median (all treatments) of 3 on an NPRS and the response was statistically significant. There was no difference between median negative change in pain scores in the 19 (79%) treatments where pain was either strongly movement related or in 22 (94%) treatments where local bone tenderness was pronounced. In 13 (54%) patient treatments where both of these features were present, the median negative change in pain score was 3.5. A significant reduction in pain score was still observed in 6 of 7 (86%) patient treatments where current regular orally administered NSAIDs or COX-2 selective agents were prescribed. The median patient treatment satisfaction rating with analgesia at 48 hours in assessable treatments (23 of 24) was 4 on the 5-point rating scale.
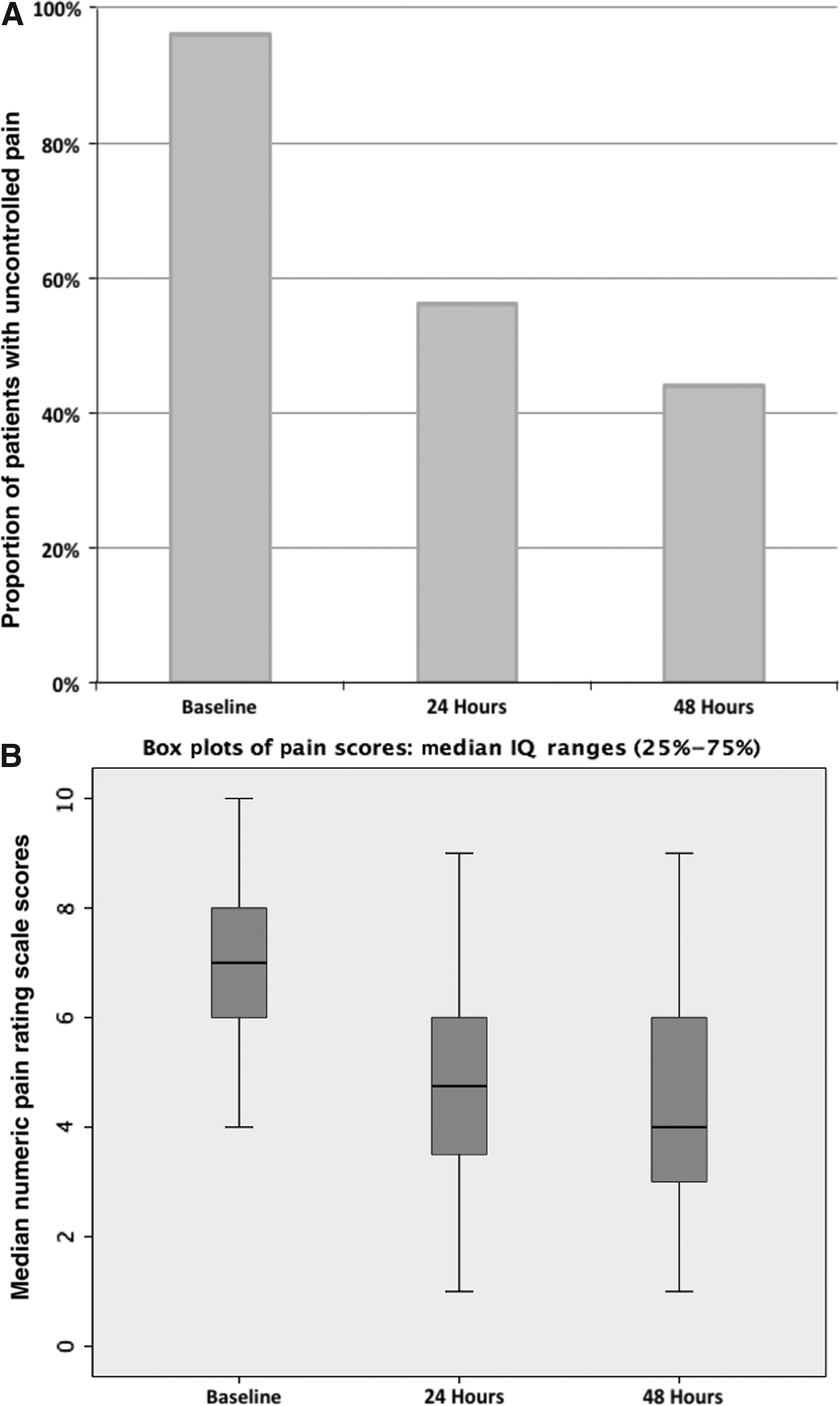
Proportion of patients with pain score >4 at baseline and intervention times (24 and 48 hours).

Changes in pain scores from baseline to 24 hours. Reduction in NPRS at 24 hours.
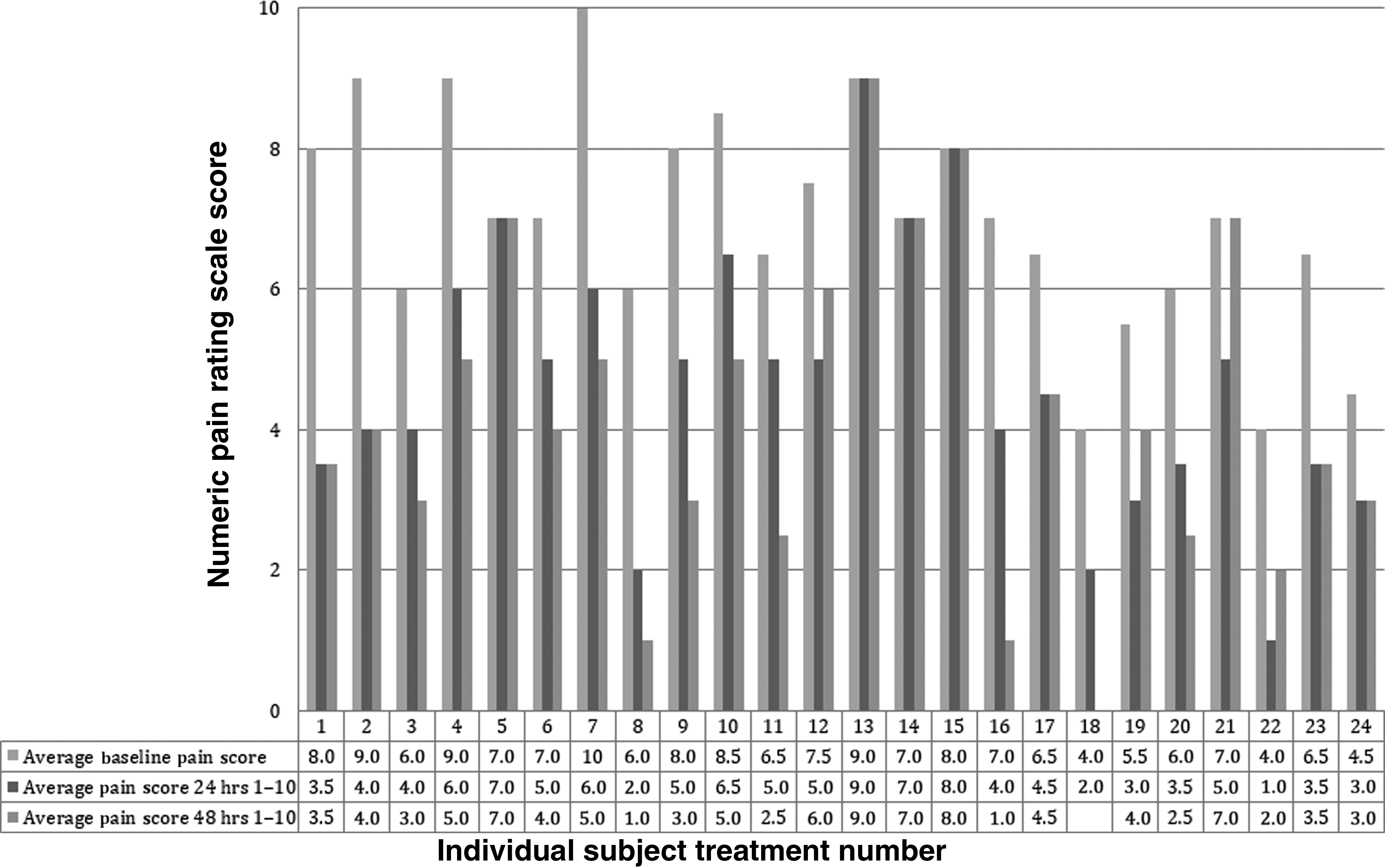
Pain scores for individual subject treatments versus time at baseline and intervention times (24 and 48 hours).
Discussion
A short three-day ‘burst’ of one to three daily subcutaneous injections of parecoxib sodium was effective therapy in our patients with severe cancer-related bone pain when added to their existing treatment and appeared comparable to that obtained in our service with the past selective use of ketorolac tromethamine 30 mg daily by subcutaneous infusion. The potency of parecoxib was noteworthy, and current therapy with corticosteroids and prior or current oral NSAIDs or COX-2 inhibitors did not appear to preclude a therapeutic response. Several of our patients could continue with oral NSAID therapy after receiving parecoxib without apparent loss of pain control: some patients received palliative radiotherapy and parecoxib treatment resulted in better pain control in the period until treatment commenced. The simplicity of a single daily subcutaneous injection was advantageous compared to the need for continuous subcutaneous drug infusion. The two self-limiting site reactions appeared no worse than those observed with subcutaneous administration of other drugs. Also, the subcutaneous cannulae were not used exclusively for parecoxib and hence site reactions could not be confidently attributed solely to this agent.
As this was a pilot study, our dosing was conservative and was limited to a single 40 mg daily injection; some of our patients might have achieved greater response to a higher dose of parecoxib, albeit with an increased risk of adverse events. Treatment was limited to three days, as this agent is licensed for single-dose perioperative use in Australia, and we were also aware of the possible longer-term adverse cardiovascular risks of orally administered COX-2 inhibitors, including rofecoxib and valdecoxib.25,26
The efficacy of parecoxib for noncardiac postoperative analgesia is well described.3–6 Parecoxib is rapidly converted to valdecoxib by hydrolysis after administration,1,2 and analgesia is said to begin within 15 minutes of an intravenous or intramuscular injection. Valdecoxib is then extensively metabolized and most of its metabolites are excreted in the urine; this metabolism includes cytochrome P450 iso-enzymes 3A4 and 2C9.
We observed no deterioration in renal function after parecoxib 40 mg daily despite two patients having moderately severe renal failure. One of our patients died from pulmonary embolism less than 24 hours after treatment with parecoxib and 72 hours after cessation of concurrent prophylactic heparin prior to staging liver biopsy. Although it is unlikely that parecoxib contributed, we cannot exclude this possibility. Schug 27 reported no increased risk of vascular adverse events in noncardiac postoperative surgical patients given parecoxib, although after cardiac surgery an increased incidence of thrombotic events has been reported when therapy is extended to 10 days or more.28–30 The increased cardiovascular risk of ongoing selective COX-2 inhibitor administration is well described, and the therapeutic benefit-to-risk ratio needs to be individually assessed in patients with a longer cancer prognosis and known comorbid nonmalignant disease.
Conclusions
Short-term single daily dose ‘off-label’ subcutaneous injection of parecoxib sodium was effective in selected patients with severe bone cancer pain when added to existing analgesic therapy. The apparent longer duration of drug action compared with single injection of the comparable nonselective agent, ketorolac tromethamine, may obviate the need for continuous subcutaneous drug infusion. It may have a role as a ‘circuit-breaking’ agent for rapid pain reduction in selected patients with intractable bone pain as part of a comprehensive pain strategy and also particularly in the terminal period where potential longer-term risks are irrelevant. It is not known whether other cancer pain syndromes may be similarly amenable to parecoxib.
The limitations of this pilot study include the relatively low treatment numbers, the open label design and patient selection, and the lack of a control treatment arm. Nevertheless our findings indicate the efficacy and tolerability of short-term daily subcutaneous parecoxib sodium for malignant bone pain, and further research into the use of this agent in patients with advanced cancer would be worthwhile.
Footnotes
Acknowledgments
The authors acknowledge the assistance of Maryann Street and Luis Vitetta with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.