
Abstract
Abstract
Many people in our communities live with symptoms for years or decades, something of relevance to hospice/palliative care clinicians and researchers. The proportion of people in the community at large who have a chronic symptom is likely to approximate the proportion of people referred to hospice/palliative care services with that same chronic symptom that pre-dates their life-limiting illness. Such patients may have different responsiveness to, and expectations from, symptomatic therapies, thus requiring more advanced approaches to symptom control.
For researchers evaluating the impact of hospice/palliative care services, failing to account for people with long-term refractory symptoms pre-dating their life-limiting illness may systematically underestimate services' benefits. Observational symptom prevalence studies reported in hospice/palliative care to date have not accounted for people with long-term refractory symptoms, potentially systematically overestimating symptoms attributed to life-limiting illnesses.
Cross-sectional community prevalence rates of key chronic refractory symptoms largely unrelated to their life-limiting illness reflect the likely prevalence on referral to hospice/palliative care: fatigue (up to 35%); pain (12%–31%); pain with neuropathic characteristics (9%); constipation (2%–29%); dyspnea (4%–9%); cognitive impairment (>10% of people >65 years old; >30% of people >85 years old); anxiety (4%); and depression (lifetime incidence 2%–15%; one year prevalence 3%).
Prospective research is needed to establish (1) the prevalence and severity of chronic symptoms that pre-date the diagnosis of a life-limiting illness in people referred to hospice/palliative care services, comparing this to whole-of-population estimates; and (2) whether this group is disproportionately represented in people with refractory symptoms.
The Prevalent Chronic Symptom Burden in the Community
A
The group of people who are of interest in this paper are those people with chronic symptoms that pre-date by years a recently superimposed life-limiting illness and who have ongoing problems because of the long-term, refractory symptom(s) (see Figs. 1a and 1b).

The whole populations, the proportion with a chronic symptom, and the proportion with a life-limiting illness.
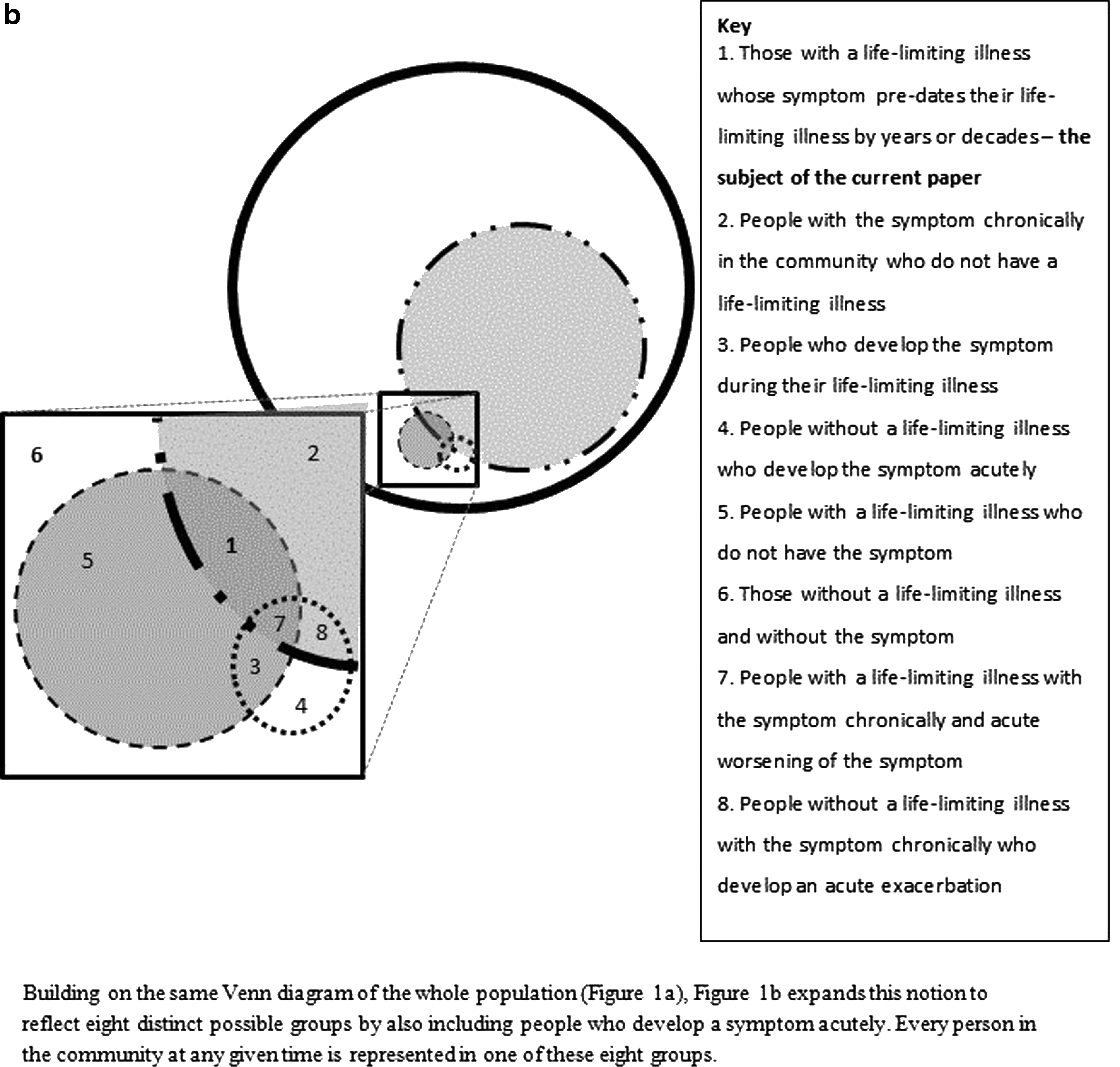
The whole population with and without the symptom, chronically and acutely. (The additional circle is for people with the symptom acutely.)
Current Community Prevalence of Chronic Symptoms Relevant to Hospice/Palliative Care Services
Key symptoms—from available adult population estimates of symptom burden independent of health service utilization and relevant to hospice/palliative care services—include fatigue, pain, constipation, dyspnea, cognitive impairment, anxiety, and depression. In the following section, the overall population estimates of symptoms are described to illustrate the potential burden of preexisting refractory symptoms in hospice/palliative care. Population estimates that do not rely on health service contact are still influenced by definitions of the symptom, sampling techniques, and the demographic characteristics of the study population. These estimates also include people diagnosed with a life-limiting illness, although those who have a life-limiting illness are likely to be a small percentage of the people with chronic symptoms in the community given that between 1.0% and 1.5% of the community die each year.
Fatigue
A Korean population prevalence study 2 using the Brief Fatigue Inventory found 16.5% of the study population rated fatigue as ‘severe’ and 37.8% rated fatigue as ‘moderate.’ A Danish study reports that 14.7% of the study population were fatigued in one or more of the six activity categories measured on the Mobility-Tiredness Scale. 3 A Dutch study of a random sample of residents of Nijmegen found no fatigue, 64.4%; short-term (<6 months) fatigue, 4.9%; chronic fatigue, 30.5%; and chronic fatigue syndrome (CFS, in accordance with U.S. CDC criteria, without clinical confirmation) of <1%. 4
Arguably, fatigue remains the most difficult symptom to treat. 5 Fatigue often overlaps with depression in both clinical and general populations. There is also a relationship between people with CFS and use of both analgesics for pain and antidepressants for depression. 6
Pain
The prevalence of chronic pain is reported to be between 12.0% in Spain and 30.7% in the United States,7–11 and prevalence of all types of pain was found to be 20.0% in five European countries. 12 Higher prevalence of chronic pain is seen in women (approximately 3% greater than men); older people; people from lower socioeconomic groups; lower levels of education; and some cultural groups.8,9,11 Chronic pain is also associated with higher levels of psychological distress; poorer self-rated health; greater likelihood of receiving income support; and comorbidities including heart disease (34%), emphysema (41%), or cancer (29%).1,13
Patients entering hospice/palliative care services who already experience chronic pain may be less responsive to attempts to palliate their pain due to anatomical and pathophysiological changes. 14 For example, chronic pain changes the physiological response to new pain due to sensitization. 13 People who are already using opioids for chronic pain are likely to be less responsive to opioids for new pain or worsening of existing pain.
For the subgroup of people for whom their pain is predominantly neuropathic, recent population-based data have been published. A study of adults from general practices in 12 regions of the United Kingdom (n=10,000; response rate, 47%) asked respondents to self-administer the Leeds Assessment of Neuropathic Signs and Symptoms (S-LANSS). Of respondents, 8.9% had chronic pain with neuropathic characteristics in the cross-sectional sample. 15
Constipation
Functional (primary) constipation is estimated to affect up to 15% of the population and hence it is likely that at least 15% of people referred to hospice/palliative care services will have a history of functional constipation that pre-dates their life-limiting illness by years or decades. Of these, 23% are likely to be related to slow colonic transit, 37% related to pelvic floor disturbances, while 55% of constipated people have a degree of both. Likewise. the estimates of the prevalence of secondary constipation vary, with 40% of people taking opioids for chronic pain experiencing constipation, 16 and up to 75% of people in residential aged facilities likely to be taking laxatives. 17 Older people and females are more likely to self-report constipation. Population studies suggest that 2%–29% of adults in the United States suffer disturbed bowel function, with one in six people taking regular or intermittent laxatives.18,19 Given these rates, it will be important in future work to codify whether these are the people with constipation that is more difficult to control.
Breathlessness
Population estimates for dyspnea that has an impact on activities of daily living vary: a longitudinal Scandinavian study (12-year follow-up; n=3786) had a prevalence of persistent breathlessness of 6.9% for women and 4.3% for men. 20 Another study, with 19,998 people followed for 30 years, demonstrated higher rates of death with higher levels of breathlessness across the community. 21 In a cross-sectional study (n=8396), 8.9% of people had some breathlessness, while 1% had chronic disabling breathlessness and 1 in 300 were housebound because of breathlessness measured with the modified Medical Research Council Scale (mMRC). 22
Depression and anxiety
Depression is a major public health issue with lifetime incidence ranging from 2%–15%. 23 In the year 2000, depression was rated as the fourth leading cause of disease burden, accounting for 4.4% of total disability adjusted life years (DALYs). The largest known population-based survey (WHO World Health Survey), involving 60 countries and 245,404 participants, found the one-year prevalence for International Classification of Disease (ICD) version 10 depressive episodes was 3.2% (95% CI 3.0–3.5). 24 Women have a twofold greater risk of developing depression than men. 25 Global population-based studies estimate that anxiety is prevalent for 4.0% of the population. 26 Anxiety is twice as prevalent in women (5.2%) than men (2.8%). 26
Cognitive impairment
Approximately 36 million people globally have dementia. Although cognitive impairment is more likely to be reported by the caregiver, some patients will notice impaired cognition. This number will double by 2030 and more than treble to over 115 million by 2050. 27 In Western countries dementia is present in 5%–10% of adults 65 and older and by age 85, 30% will have dementia. 28 Alzheimer's disease is the most common cause of dementia; ischemic cerebrovascular disease and Lewy body dementia are other common causes that often co-occur with Alzheimer's disease. 29
Most symptoms in people who are cognitively impaired are likely to be underrecognized and underdiagnosed due to individuals' variable abilities to both understand and verbally respond to queries about their symptoms. In patients with severe dementia, pain is commonly shown to be present in individuals with behavioral disturbances such as agitation, repetitive behaviors, socially disruptive behaviors, and wandering. Anhedonia, social withdrawal, and decreases in appetite and activity may be indicators of pain or depression with any severity of dementia. 30 Delirium occurs more commonly in the setting of dementia and may be more persistent.31,32
The impact of cognitive impairment on symptom ascertainment and management in end-of-life care remains poorly elucidated due to the paucity of research in this area. Research is needed to understand the optimal assessment and management of all types of symptoms in individuals with preexisting cognitive impairment.
Why Are Community Rates of Symptoms Important in Hospice/Palliative Care?
At three levels, these preexisting symptoms potentially have importance in hospice/palliative care: clinically, in order to provide optimal palliation of symptoms; in evaluating service performance; and in future research.
Optimal palliation of symptoms
While palliative care aims to alleviate symptoms and optimize function, not everyone with a life-limiting illness is able to have their symptoms controlled or in some cases even reduced. Despite reluctantly acknowledging this reality, at a population level, little attention has been given defining the characteristics of the populations for whom symptom control is more challenging. Yet, it is highly likely that people with chronic symptoms pre-dating their life-limiting illness are represented at least with the prevalence outlined above at the time of referral to hospice/palliative care services. They may, as a subgroup, be overrepresented as a portion of referrals and as a portion of people with difficult to control symptoms at the end of life. If this position is accepted as plausible, then conceptually different therapeutic approaches may be required in three subgroups of patients with preexisting symptoms when referred to hospice/palliative care services:
(1) Those with a chronic symptom that does not change as the result of the life-limiting illness. In this setting, a major improvement in symptom control may be unlikely. (2) Those with a chronic symptom unrelated to the life-limiting illness itself, that is exacerbated or becomes unstable due to the presence of the life-limiting illness. (3) Symptoms attributable to both a chronic component and a life-limiting illness.
Symptom management for these three subgroups is likely to be distinct from management of patients with new symptoms related only to the life-limiting illness. If a symptom has been chronic and has not responded to optimal treatment of the underlying condition nor to symptom control measures, the longer it has been present the more likely that it will be refractory to currently available therapies. The history of a preceding distressing symptom requires additional attention by the hospice/palliative care clinician to meet patient-centered goals while simultaneously ensuring that patients' expectations are aligned with achievable clinical outcomes.
Evaluating service performance
In evaluating hospice/palliative care services, the benefits in symptom control achieved by these services may be underestimated systematically when no account has been taken of the preexisting (most likely refractory, long-term) symptom burden unrelated to the life-limiting illness people have when referred to the service. When symptom burden is unrelated to the life-limiting illness and has not been amenable to previous attempts at symptomatic treatment nor treatment of the underlying cause(s), the diagnosis of a life-limiting illness is unlikely to suddenly offer opportunity to improve control of the long-term symptom. As suggested above, the degree of chronicity may reduce the effectiveness of interventions, which in turn may make it less likely that referral to a hospice/palliative care service is going to have as much of an impact on reducing this person's symptom burden, although for some people referral to hospice/palliative care may be the first adequate assessment of their symptom.
Other research
In hospice/palliative care research, large numbers of observational studies on symptom burden are published. 33 In these studies, people referred to specialist hospice/palliative care services demonstrate great heterogeneity in the overall percentage of people with a life-limiting illness referred; diagnostic mix of conditions of those referred; and time point in their illness at which they are referred given that there are no national nor international criteria for referral to specialist hospice/palliative care services.
The point in disease trajectories at which symptoms are measured and reported in hospice/palliative care populations varies widely across the developed world, resulting in widely varying estimates of the symptom burden in hospice/palliative care. This variation in estimates is further compounded by failing to account for a population's preexisting symptom burden unrelated to their life-limiting illnesses. There is likely to be a systematic overestimation of the symptom burden directly attributable to life-limiting illnesses or their treatment. By taking account of preexisting chronic symptoms, in future research there will be a more accurate estimate of the new symptoms generated just by a life-limiting illness.
Future research
It will be important to consider a specific prospective research agenda that allows quantification of the prevalence and intensity of long-term symptoms that pre-date and are not related to a life-limiting diagnosis in people referred to hospice/palliative care services. The most important research agenda to arise from this categorization is to determine whether or not people with long-term symptoms that pre-date their life-limiting illness are disproportionately represented in people referred to hospice/palliative care services or, within services, those with refractory symptoms.
Conclusion
Ultimately, there are implications for hospice/palliative care clinicians and researchers from the burden of preexisting chronic symptoms that people have when referred to specialist services. These need to be taken into account in order to tailor clinical assessment and therapies, and to incorporate these symptoms into the assessment of symptom prevalence and service outcomes. Research needs to identify this specific group of hospice/palliative care patients and ensure that we understand their symptom burden and the proportion of them for whom that symptom is ‘refractory.’ This also requires us to understand if there are systematic difference in the clinical management that is offered.
Footnotes
Author Disclosure Statement
No competing financial interests exist.