
Abstract
Abstract
Background:
Community-based palliative care can improve outcomes and avoid unnecessary spending, but the effects of its widespread adoption on health care spending in California is unknown.
Objective:
To estimate the spending avoided if, by 2022, more than 100,000 Californians received community-based palliative care (CBPC) per year.
Design:
We estimated the 6-month per-patient spending avoided through three mature CBPC programs in California and extrapolated data to predict the total avoided spending statewide over 8 years if enrollment in the three programs proceeded according to our model.
Results:
If Californians participated in CBPC in the numbers envisioned, in 2014 there would have been a $72 million reduction in intensive hospital based care, while still respecting patients' wishes, and nearly $1.1 billion in spending could be avoided in 2022. Overall hospital spending would be reduced by more than $5.5 billion through 2022.
Conclusions:
Existing CBPC programs have the potential to provide care that is both in alignment with patients' wishes and avoids substantial amounts of unnecessary hospital-based spending.
Introduction
A
Palliative-based care
Generally, palliative care combines pain and symptom management, goal setting, family caregiver support, and practical and social support. 2 It operates on a continuum of care in which the proportion of curative to palliative services varies over the course of illness (Fig. 1) Palliative care cannot be delivered solely in the hospital setting but needs to be available in the community; having care delivered in the home or a clinic can also help dispel the misperceptions of palliative care, for example, the conflation of palliative care with hospice care.

Intensity of type of care over the course of illness.
For providers and plans to offer palliative care interventions that produce high-value, high-quality care, they must accurately target the patients who will benefit most. For example, early palliative care provided to patients with non-small–cell lung cancer has been shown to improve quality of life, reduce depressive symptoms, reduce provision of aggressive end-of-life care, and has been associated with longer survival time. 3
Additionally, spending on seriously ill patients—often for low-value services or care that does not align with patient wishes—comprises a large proportion of health care expenditures. Medicare spends approximately 25% of its budget on the 5% of U.S. beneficiaries who die each year. Failing to provide care concordant with patient preferences reduces quality of care while unnecessarily generating high costs. Fortunately, opportunities for better end-of-life care exist both in the hospital and in community settings, such as the patient home and outpatient clinics.
In-home palliative care can improve patient satisfaction, increase likelihood of dying at home, and reduce emergency department visits and hospital admissions. 4 However, although hospital-based palliative consultation services have increased recently, 5 few hospitals in California operate outpatient palliative care services. 6 Meanwhile, ambulatory Community-Based Palliative Care (CBPC) programs have extended their outreach into the homes, where providers can identify risks that might not otherwise be uncovered in an ambulatory setting or through telephone calls.
In 2013, The Berkeley Forum for Improving California's Healthcare Delivery System shared its vision for the state's delivery and payment system. 7 The Berkeley Forum's vision called for an increase in the use of concurrent curative-intent and CBPC for seriously ill patients, to include a focus on advance care planning and physical, emotional, and social support. It would provide access to interdisciplinary patient-centered CBPC to patients who have a prognosis of approximately 1 year or less as a result of certain conditions.
The Forum modeled the number of potentially eligible patients from estimates of deaths from the considered medical conditions and the increased provision of palliative care over time. By 2022, half of all Californians with the disease conditions would receive CBPC (Fig. 2). This number of potential patients with varying preferences gives providers the opportunity to design systems that increase the range of CBPC choices.
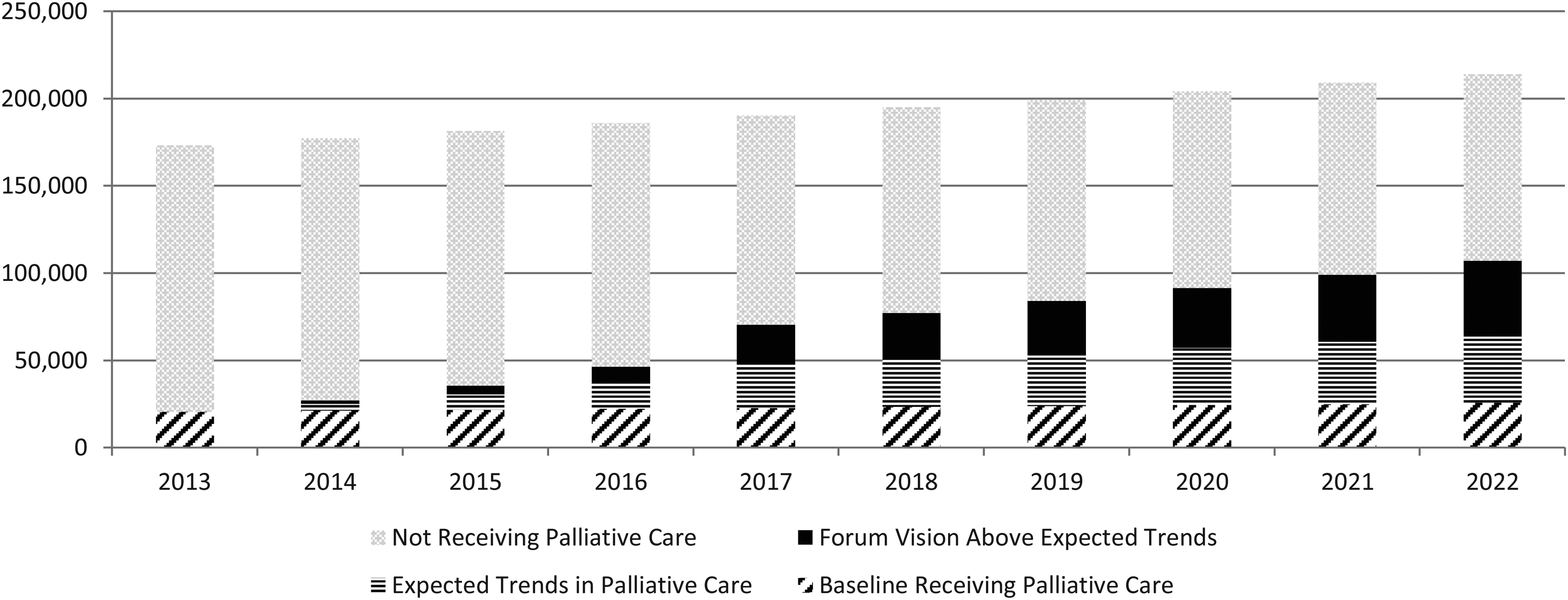
Projected provision of community-based palliative care in California, 2013–2022 Source: Berkeley Forum calculations using data from the California Department of Public Health.
In 2012, more than 19 million Californians were covered by one of seven insurance plans that either implemented or were planning programs to increase access to palliative care. 8 California SB1004 required Managed Medi-Cal plans to establish standards to ensure delivery of palliative care services, 9 potentially expanding access to a broad swath of the population. As would be expected in a developing field, the programs vary in location of care (e.g., ambulatory clinics, at home, via telephone), type of providers delivering care (physicians, nurses, nurse practitioners, social workers), and type of care provided (concurrent treatment for illness-directed care, enhanced case management, goal-setting, pain/symptom management, advance care planning).
The purpose of this article is to examine the value in reducing the expense of high-cost, undesired hospital spending, if CBPC were implemented on a scale consistent with the Forum Vision.
Methods
Eligible population and potential uptake
The Berkeley Forum estimated the number of new patients who would be diagnosed with one of several chronic conditions in each year through 2022a. 7 Conditions that would be covered include cancer, chronic obstructive pulmonary disease, congestive heart failure, dementia, amyotrophic lateral sclerosis (ALS), cirrhosis, and human immunodeficiency virus (HIV). Based on expert opinion, we added an additional 25% to the target population. We assumed that at baseline, 12% of the eligible population would receive outpatient palliative care. We also modeled current trends in uptake so that from 2013 to 2022 the proportion of eligible patients increased from 12% to 30%. Finally, we modeled uptake consistent with the Berkeley Forum Vision of 50% uptake by 2022. Details are shown in Figure 2. For example, we forecast that in 2022 there will be 214,135 patients potentially eligible for CBPC. A baseline of 25,696 would already have been receiving care, and current trends suggest that an additional 38,544 would receive care. A total of 81,131 would be treated under the Forum's vision in 2022.
Scope of reduced spending
To estimate savings from CBPC, we conducted a review from California and nationwide that had been established long enough to be described in peer-reviewed literature. We limited our review to studies that estimated net savings/cost-reductions, which already accounted for the direct costs of providing the intervention.
We selected three programs that covered a variety of approaches (described below) and projected their cost savings estimates over a 6-month period. Other well-established programs exist both in California and nationwide, but we selected models based on availability of peer-reviewed utilization and cost estimates. We modeled the Forum Vision's uptake of community-based palliative care from 2014 to 2022, estimating changes in health care utilization and their resulting effect on health care costs in the last year of life. Each of the three models described received 25% of the number of patients included in the Forum Vision for that year (for example 5,895 in 2014 and 81,371 in 2022). We assumed that 25% of eligible patients joined each of the three programs and experienced outcomes and savings at the average rate reported. We also assumed that 25% of patients enrolled in different CBPC models than the three more-established programs. To model improvements in efficiency in smaller programs over time, we increased the performance relative to the larger plans from 50% in 2014 to 82% in 2022. We then provided lower- and upper-bound forecasts by subtracting and adding 25% to our projections.
We created six scenarios for avoided spending. For the first three, we projected current trends of numbers enrolled in CBPC multiplied by the low, middle, and high forecast of average savings. For the second three, we projected numbers of enrolled in CBPC by the numbers in the Berkeley Forum Vision.
Results
Sharp HealthCare Transitions Program
This model provided home-based, ambulatory, and telephone-based follow-up to those with advanced heart failure. 10 Patient and caregiver choice is enhanced through an evidence-based prognostication model, which provides practical information about the disease process in advance of milestones. This patient-centered approach encourages decision making away from the emergency room, intensive care unit (ICU), or hospital, where choices are more likely to be reactive. The intervention simultaneously offers curative and multidisciplinary palliative services, which increase over the course of illness. Services include in-home medical consultation, caregiver support, and advance health care planning.
The program reduces emergency department visits by 58% and expenditures of 36%. The total cost of care per patient decreased by over $26,000 per patient.
Sutter Advanced Illness Management (AIM) Program
This intervention combines hospital, home care, telephone, and clinic-based interventions to ease the transition between curative and comfort care for seriously ill patients. It provides evidence-based, patient-centered care and care management and has served more than 4,600 patients since July 2012. The program was developed in response to uncoordinated care and acute episodes that frequently led to end-of-life care that was unwanted and unsatisfactory to patients, caregivers and providers. The AIM model depends on patient/caregiver engagement, goal setting, and self-management. 11 Through this process, the focus of care is moved from the hospital to the home/community, where most choose to be. Patients are provided with hospital liaisons, care managers at physician offices, telephonic support (remotely or imbedded in physician group), and home-based services.
Early outcomes have shown a 53% reduction in hospitalizations postenrollment and a 75% reduction in ICU days. Total expenditure reductions in the AIM program are approximately $2,000/month per patient. 11
Aetna Case Management
This telephone-based management program identifies patients through review of admissions, physician referral, and proprietary modeling. 12 Few patients decline the option of specialized case management in lieu of traditional case management. The program employs a nurse case manager to provide patient education and care coordination with the patient's physician. The case manager addresses patient and caregiver needs for education on the disease process, offers assistance with advance care directives, and identifies patient preferences for care. Greater treatment options expand the length of time for inpatient hospice and dollar limits on outpatient hospice, and curative treatment is offered concurrently with hospice services. Forum staff estimated cost savings from the reported reduction in emergency department visits and acute inpatient days to be approximately $7,600 over 6 months.
Table 1 shows the forecasted mean per-patient reduced spending (in 2014 dollars) for patients participating in one of the four community-based palliative care programs; low and high amounts were established by adding and subtracting 25% of the projected cost reductions.
Source: Authors' calculations using data from Hoefer et al., 2013, Sutter Health Advanced Illness Management, Spettel et al. 2009, and Kaiser Family Foundation.
Scaling-up model and results
In our main projection, using the Forum Vision estimate of uptake and our middle estimate of reduced spending, we estimate that in 2014 there would have been a $72 million reduction in intensive hospital-based care, and nearly $1.1 billion in spending could be avoided in 2022 while still respecting patients' wishes. Overall hospital spending would be reduced by more than $5.5 billion through 2022 (Fig. 3). If current trends hold, the avoided spending would be more than $600 million by 2022, with more than $4.1 billion in total avoided spending (Fig. 4).
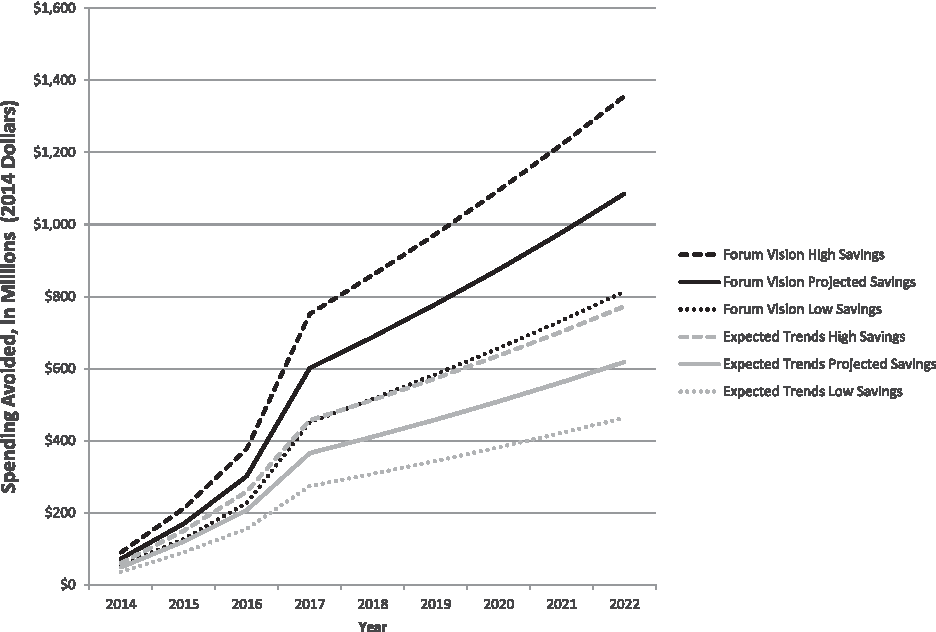
Estimated total spending avoided due to community based palliative care under different uptake and savings scenarios Source: Berkeley Forum calculations using data from Hoefer et al., 2013, Sutter Health Advanced Illness Management, Spettel et al., 2009, the California Department of Public Health and Kaiser Family Foundation.
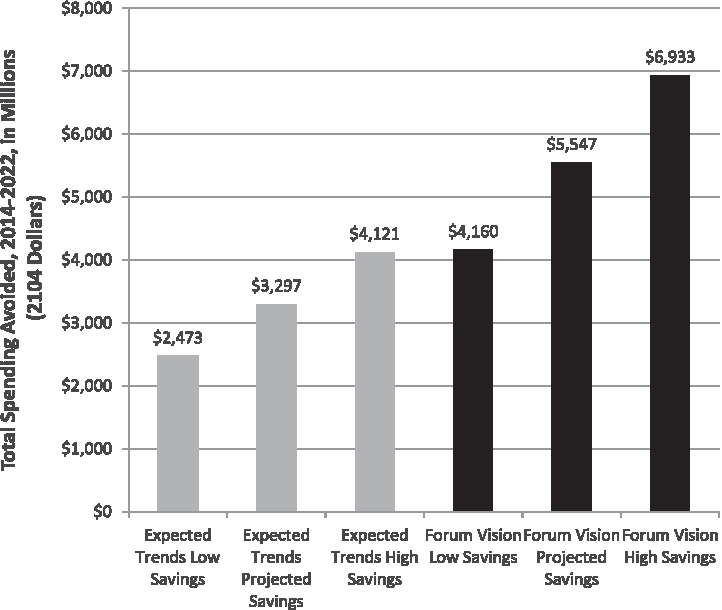
Total spending avoided, 2014–2022, as a result of community-based palliative care under different uptake and savings scenarios Source: Berkeley Forum calculations using data from Hoefer et al., 2013, Sutter Health Advanced Illness Management, Spettel et al., 2009, the California Department of Public Health and Kaiser Family Foundation.
Discussion
Palliative care and CBPC are being incorporated rapidly into standard care. Consensus statements from medical societies, the Joint Commission, national quality standards, and statewide plans to improve the health care delivery system all point toward improved patient choice and patient-centered care for chronic conditions and at the end of life.
Preventing unwanted care can improve patient and caregiver satisfaction while reducing expenditures, creating an alignment for insurers and providers to develop reimbursement models that integrate CBPC into the treatment of chronic illness. Patient-centered medical homes, which focus care management on patients with chronic illness, are natural settings to incorporate CBPC.
Palliative care programs can be resource intensive, and their net cost or savings to the provider and plan depends on a number of factors, including who is at risk for health care expenses, the target population, the care delivery model, baseline practice patterns, and payer mix. California's extensive managed care penetration provides many opportunities to explore payment mechanisms. 13 Medicare hospice benefit rules can limit providers who want to structure palliative care programs flexibly and to offer concurrent care. However, California's extensive managed care penetration provides many opportunities to explore payment mechanisms. 14 CHCF has called for developing and testing new reimbursement models, and in October 2014 issued 10 grants to “pair payers and providers to develop operational and financial plans for delivering palliative care projects in the community setting.”b Additionally, the California State Innovations Model (CalSIM) proposal calls for “new benefit and payment approaches to better meet patient preferences for palliative and hospice care.” 15 With properly devised incentives, plans and providers should be able to provide options to patients that increase satisfaction while avoiding unnecessary expenditures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.