
Abstract
Abstract
Background:
Communication among doctors, nurses, and families contributes to high-quality end-of-life care, but is difficult to improve.
Objective:
Our objective was to identify aspects of communication appropriate for interventions to improve quality of dying in the intensive care unit (ICU).
Methods:
This observational study used data from a cluster-randomized trial of an interdisciplinary intervention to improve end-of-life care at 15 Seattle/Tacoma area hospitals (2003–2008). Nurses completed surveys for patients dying in the ICU. We examined associations between nurse-assessed predictors (physician-nurse communication, physician-family communication) and nurse ratings of patients' quality of dying (nurse-QODD-1).
Results:
Based on 1173 nurse surveys, four of six physician-nurse communication topics were positively associated with nurse-QODD-1: family questions, family dynamics, spiritual/religious issues, and cultural issues. Discussions between nurses and physicians about nurses' concerns for patients or families were negatively associated. All physician-family communication ratings, as assessed by nurses, were positively associated with nurse-QODD-1: answering family's questions, listening to family, asking about treatments patient would want, helping family decide patient's treatment wishes, and overall communication. Path analysis suggested overall physician-family communication and helping family incorporate patient's wishes were directly associated with nurse-QODD-1.
Conclusions:
Several topics of physician-nurse communication, as rated by nurses, were associated with higher nurse-rated quality of dying, whereas one topic, nurses' concerns for patient or family, was associated with poorer ratings. Higher nurse ratings of physician-family communication were uniformly associated with higher quality of dying, highlighting the importance of this communication. Physician support of family decision making was particularly important, suggesting a potential target for interventions to improve end-of-life care.
Introduction
W
Two aspects of communication in the ICU that might be used to improve end-of-life care are physician-nurse communication and physician-family communication. Improved physician-nurse communication has been associated with enhanced provider satisfaction and improved patient outcomes, such as reduced ICU lengths of stay and costs of care.12–17 However, there is a lack of consensus among nurses and physicians about which components of physician-nurse communication are clinically useful 18 and about whether this communication is actually occurring.19–21 When nurses and physicians are surveyed, nurses perceive less physician-nurse communication and less involvement in decision making than physicians.19,22–24 With regards to communication with family members, families of critically ill patients consistently rate improved communication as an important need25,26 and report that inconsistency in communication between physicians and nurses is a source of distress.27,28 Furthermore, physician-family communication has been shown to have an important effect on family psychological outcomes, such as depression, anxiety, and posttraumatic distress.6,28–30 Despite this consensus on the important role of communication, some recent studies designed to improve general and broad aspects of communication about palliative care in the ICU have been unsuccessful.31,32 These negative trials suggest a need for more information about the specific aspects of communication in the ICU that should be targeted for intervention.
Our study objective was to use ICU nurse assessments of quality of communication and quality of dying to identify specific targets for communication interventions to improve patients' dying experiences. To accomplish this goal, we examined nurse assessments of quality of dying for patients in the ICU and their association with nurses' reports of ICU physician communication (with nurses and with families) using data from a previously completed trial of an intervention to improve end-of-life care in the ICU. 31
Methods
Design and setting
This study used data from a cluster-randomized trial of an interdisciplinary, multifaceted intervention to improve end-of-life care for critically ill adult patients and their families. 33 Hospitals in Seattle or Tacoma, Washington, were eligible if they had enough ICU deaths to meet sample size requirements for the randomized trial. Fifteen of the 16 eligible hospitals agreed to participate, including 3 university-affiliated hospitals, 3 nonuniversity-affiliated teaching hospitals, and 9 nonteaching hospitals. All procedures were approved by institutional review boards at all institutions. Subjects in the randomized trial were enrolled under a waiver of documentation of consent; they received information sheets containing all elements of consent, but signatures were not required.
Subjects
Eligible patients were those who died in an ICU or within 30 hours of transfer to another hospital location. Patients with ICU stays shorter than 6 hours were excluded. The time restrictions allowed ICU clinicians sufficient opportunity to impact end-of-life care. Patient deaths occurred between 2003 and 2008.
Data collection
Within 72 hours of patient death, nurse questionnaires were distributed to the hospital mailbox of the ICU nurse caring for the patient at the time of death (or transfer from the ICU) and the ICU nurse from the prior shift. Questionnaire materials included a coffee card, postage-paid return envelope, and questionnaire booklet. (See online Supplementary questionnaire booklet at www.liebertpub.com/jpm and at www.liebertonline.com.) To enhance response rates, follow-up mailings were distributed, including reminder/thank-you postcards, three weeks after initial distribution, followed by a second set of materials to nonrespondents after five weeks.
We abstracted patient characteristics from medical records and death certificates. We identified comorbidities and diagnoses from medical records. Cause of death (cancer, trauma, other) was obtained from death certificates.
Outcome measure: Nurse rating of the overall quality of dying and death
The nurse-QODD-1 is a single-item question assessing the patient's experience from the nurse's perspective: “Overall, how would you rate the quality of the patient's dying?” It is scored on a 0–10 scale; 0 is “terrible experience” and 10 is “almost perfect experience.” It is based on the single-item rating from the family-completed quality of death and dying (QODD) and is associated with markers of quality of palliative care in the ICU, including documentation of a living will, absence of cardiopulmonary resuscitation performed in the last hour of life, discussion of the patient's wish to withdraw life support during a family conference, use of standardized comfort care orders, and occurrence of a family conference.34,35 The family-completed QODD-1 score has been shown to differentiate higher quality of dying and death for decedents receiving lower intensity of care at the end of life and for families participating in patient- and family-centered decision making; significant differences of one point on the QODD-1 scale have been associated with the presence of comfort care orders as compared to patients who died without comfort care orders in place. 34
Predictors from nurse surveys
Physician-nurse communication topic
Physician-nurse communication topics were scored dichotomously (yes/no) and included two items: (1) Did the nurse and physician discuss the patient's care? (2) If yes, which of these topics were discussed (patient/family perceptions of diagnosis or prognosis, specific family questions, family dynamics, spiritual considerations, cultural considerations, and nurses' concerns related to the patient or family)?
Physician-family communication topics
Nurses assessed physician-family communication with four items from the Quality of Communication questionnaire (QOC) 36 : (1) answered family's questions about illness/treatment, (2) listened to what the family had to say, (3) asked about treatments patient would want, and (4) helped family decide treatments the patient would want. A single-item rating of the overall quality of physician-family communication was also included. Ratings ranged from 0 to 10, with 0 = “the very worst I could imagine” and 10 = “the very best I could imagine.” Nurses also had two additional options, “Doctor didn't do” and “I don't know.” “Doctor didn't do” responses were recoded as “0,” as reported previously. 36 “I don't know” responses were coded as missing values.
Confounders
Potential confounders included nurse characteristics (gender and years in critical care); patient characteristics (gender, minority racial/ethnic status, age, and cause of death as cancer, trauma, other); hospital site; and intervention group.
Statistical analyses
Nurse data produced a crossclassified design: Each patient could be evaluated by two nurses, and each nurse could evaluate multiple patients. To simplify this design, we selected one nurse evaluation per patient, with the selection favoring the evaluation that included the most complete responses on the QODD (likely signifying the nurse with more knowledge of the patient's dying experience). In the event of two QODD instruments with an equal number of complete responses, we selected one randomly. This procedure resulted in a simple clustered design, appropriate for analysis with clustered linear regression models (patients clustered under nurses) to test the association of physician-nurse and physician-family communication with the nurse-QODD-1. Parameters were estimated with restricted maximum likelihood. When a predictor of interest was associated with the outcome at a P-value of 0.20 or below in an unadjusted model, we tested each variable in the confounder pool in an adjusted model; if addition of the confounder changed the coefficient for the predictor of interest by 10% or more, we included it in the final model for the predictor of interest.
Finally, we tested a path model showing possible interrelationships among the components of physician-family communication and their associations with the nurse-QODD-1. Path analysis (also called structural equation modeling) involves specification of a hypothetical model that attempts to explain why observed correlations between variables exist: which variables might cause changes in other variables and which of the correlations are spurious.37,38
Because we lacked an overarching theory of ICU physician-family communication, we relied on available literature and our clinical experience to construct an ad-hoc theory (i.e., patterns that seemed to make the most sense, conceptually). 39 We began with three topics of communication that appeared to be mutually influential, with cause potentially flowing in both directions: listening, asking, and answering. We then defined these as intercorrelated exogenous variables in the model, with all three having direct effects on nurse's perceptions of physician skill in helping families decide on appropriate treatments. Downstream from this point were the nurse's perceptions of physician overall skill in communicating with the family, followed by the perception of the patient's quality of death. In an initial saturated model, we hypothesized direct effects of each upstream variable on all variables downstream. Then we sequentially removed paths that were statistically nonsignificant, in descending order of the P-values of their coefficients.
Evaluation of the final model included a test of how well that model accounted for the observed covariances. This test established that, in addition to being conceptually credible, the posited causal associations were empirically plausible; however, it is not always the case that good fit ensures that the causal hypotheses supported are correct. Statistical significance for all analyses was set at two-sided P < 0.05.
Results
Sample and response rate
Of 3400 patients who died, 2176 had at least one nurse who could be identified. Nurse surveys were completed for 1294 of the eligible patients (59.5% patient-based completion rate), and 1173 patients (53.9%) had usable questionnaires in which the necessary variables for analyses (nurse-QODD-1 rating and response to at least one of the 11 predictors of interest) were completed. Of 1341 nurses who were contacted for participation, 718 (53.5%) returned one or more questionnaires, with 638 (47.6%) included in the analysis dataset, and 604 (45.0%) providing sufficient data for inclusion in the results. Chart abstraction was completed for 1110 of the 1173 patients (94.6%). Patient and nurse characteristics are summarized in Table 1.
Based on a total sample of 1173 patients and 604 nurses for whom there was a valid response on the nurse's QODD-1 rating and on at least one of the 11 predictors of interest.
Based on each of the 597 nurses' mean age at the time of death of the patients evaluated.
Based on each of the 601 nurses' mean years of experience at the time(s) of patient evaluation.
AIDS, acquired immunodeficiency syndrome; HIV, human immunodeficiency virus; ICU, intensive care unit; QODD, quality of dying; SD, standard deviation.
Outcome measures
Nurse-QODD-1
The mean (standard deviation, SD) nurse-QODD-1 score was 7.16 (2.76) on a 0–10 scale (0 = “the very worst I could imagine” and 10 = “the very best I could imagine”).
Physician-nurse communication topics
Eighty-eight percent of nurse surveys reported communicating with a physician. Nurses' reports of any communication with a physician, without considering the topic of communication, was not associated with higher ratings on the nurse-QODD-1 (b = −0.42, P = 0.09). Of the surveys reporting physician-nurse communication, 95% of surveys indicated that at least one of the six topics of interest was discussed. Nurses and physicians discussed “patient and/or family perceptions of diagnosis and/or prognosis” more frequently than any other topic (see Table 2). For four of the physician-nurse communication topics, communication was associated with higher nurse-QODD-1 ratings: specific family questions, family dynamics, spiritual considerations, and cultural considerations. However, communication of nurses' concerns related to the patient or family was associated with lower nurse-QODD-1 ratings.
Results are for six separate regression models, each regressing the nurse's QODD-1 rating on the predictor shown on the row and any confounders of that association.
Number of questionnaires with valid responses to both the predictor and outcome.
Percentage based on responses included in the regression model.
Estimated coefficient (β) for the predictor on this row.
Adjusted for hospital site, which decreased the coefficient for family dynamics by 15%.
CI, confidence interval; QODD, quality of dying.
Statistically significant (p < 0.05) findings are in bold.
Physician-family communication
Higher ratings for each of the measured topics of physician-family communication, including four specific topics and one overall communication rating, were associated with higher ratings on the nurse-QODD-1 (see Table 3). In tests of a hypothesized path model, the nurse's rating of the physician's overall communication with the family and of the physician's role in helping the family decide treatments the patient would want were directly associated with the nurse-QODD-1 (see Fig. 1, Table 4). The ratings for the other three specific topics of communication (answering family's questions about illness/treatment, listening to what the family had to say, and asking about treatments the patient would want) had direct associations with the nurse rating of the physician's role in helping the family decide treatments the patient would want and the nurse rating of the physician's overall communication with the family, thus exerting indirect effects on the nurse-QODD-1. The χ2 test of fit for this model had P = 0.76, suggesting excellent fit to the data. Tests for multicollinearity indicated that the predictor sets for each of the three outcome variables in the model (helping the family decide, overall communication, and quality of death) included no redundant predictors. The maximum variance inflation factor (VIF), 5.72, exhibited by listening as a predictor of overall communication, was well below 10.00, and the tolerance level of that predictor (0.18) well above 0.10. VIF values above 10 and tolerance values below 0.1 are evidence of unacceptable item redundancy. 40
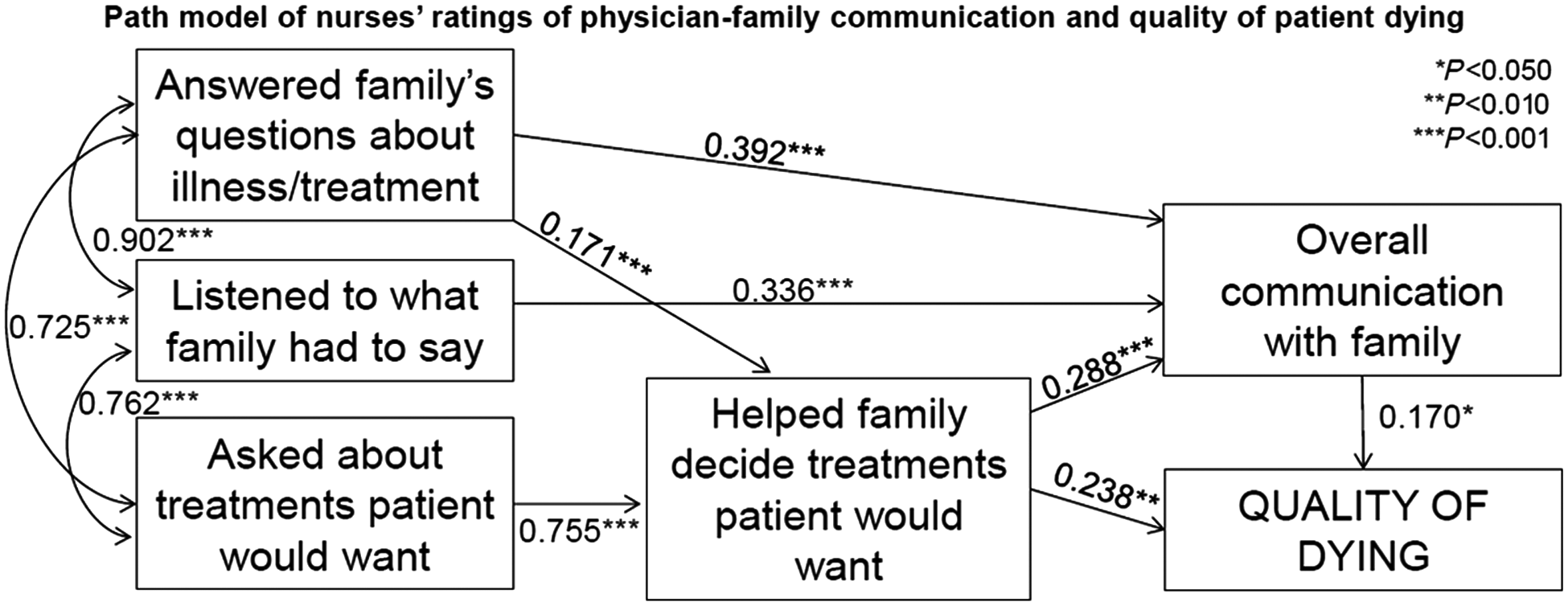
Path model of nurses' ratings of physician-family communication and quality of patient dying.
Results are for five single-predictor regression models, each regressing the nurse's QODD-1 rating on the predictor shown on the row. There were no confounders of associations between any of the five predictors and the outcome of interest.
Number of questionnaires with a valid response on the outcome, and with either a 0–10 rating, or a response of “doctor didn't do” on the predictor.
Mean and standard deviation are for the predictor with “doctor didn't do” recoded to 0, and are based on the responses included in the regression model (i.e., on questionnaires with valid data on both the predictor and outcome).
Estimated coefficient (β) for the predictor on this row.
CI, confidence interval; QODD, quality of dying; SD, standard deviation.
Statistically significant (p < 0.05) findings are in bold.
Regression coefficients shown in Figure 1 have been placed in table format. Direct effect: regression coefficient along the direct path from the aspect of communication to nurse-QODD-1.
Indirect effect:
Total effect: the sum of the direct and indirect effects.
QODD, quality of death.
Statistically significant (p < 0.05) findings are in bold.
Discussion
End-of-life care is an important component of ICU care, but evaluating the quality of that care is challenging, because we must generally rely on patients' surrogates to assess patients' experiences. Nurses are in the unique position of being able to evaluate a patient's experience of dying, situating it within the context of other patients' deaths that they have witnessed in the ICU. They also are able to observe and assess topics of physician-nurse and physician-family communication across diverse clinicians, patients, and families. By drawing on these nurse assessments, we have an opportunity to gain an understanding of those aspects of communication that are associated with an enhanced quality of dying and may be a focus for interventions to improve end-of-life care.
Physician-nurse communication in the ICU occurs regularly, but the specific content of this communication has not been well studied. This study found that simply participating in discussions with physicians did not result in improved nurse-QODD-1 ratings. Moreover, nurses and physicians discussed “patient and/or family perceptions of diagnosis and/or prognosis” more frequently than any other topic, and discussions of this type were not associated with nurses' ratings of quality of dying. In contrast, physician-nurse communication around the topics of family questions, family dynamics, spiritual considerations, and cultural considerations were significantly associated with higher nurse ratings of the quality of dying. These may be topics that, when discussed, can increase the quality of end-of-life care. For example, prior research has shown that patients and families value discussions of spiritual care in the ICU, 41 but that physicians in particular are reluctant to spontaneously raise this topic.42–44 Focusing end-of-life conversations on spiritual concerns could improve quality of dying. Potential interventions to improve the quality of end-of-life care could include teaching physicians and nurses to discuss these topics during end-of-life discussions.
Interestingly, communication of nurses' concerns related to the patient or family was associated with lower nurse-QODD-1 ratings. This finding suggests that the occurrence of communication in which nurses express concerns about patient and family issues to physicians might be an indicator of observed problems in providing patient- or family-centered care; it might be a “red flag” indicating disagreement among team members about the approach to the patient's care. Prior research suggests that improved overall physician-nurse communication and collaboration in the ICU is associated with better quality care, and our findings suggest that there are specific topics of physician-nurse communication that are associated with higher-quality end-of-life care.12,15 Encouraging physicians to be aware of the potential red flag of nursing concerns related to the patient or family could improve patient quality of dying.
The quality of physician-family communication, as assessed by nurses, was also associated with higher nurse-rated quality of dying. This was true for all topics of physician-family communication assessed in this study and is supported by observational studies and randomized trials that show that improved physician-family communication is associated with reduced prolongation of patient dying in the ICU and improved family outcomes.6,45–49 We used path modeling to test whether specific topics of physician-family communication played direct roles in ratings of quality of dying. We found that several types of physician-family communication were indirectly associated with quality of dying by contributing to the overall quality of communication with the family: listening to the family, answering their questions, and asking about treatments the patient would want. However, physician support for family decision making (defined as “helping the family decide treatments the patient would want”) occupied a central role, exerting both an indirect effect through its influence on overall communication and an independent direct effect on quality of dying. Support for family decision making might represent a particularly important target to improve quality of end-of-life care. A study of ICU family conferences also highlighted explicit support of family decision making as associated with higher family satisfaction with communication. 50 Encouraging physicians to focus on helping families make decisions in family conferences at the end of life could improve quality of dying.
This study has several important limitations. First, although these data are from a randomized trial, these analyses combined the data from both the intervention and control groups and therefore provide observational findings that cannot be assumed to be causal. Although we found associations between nurse ratings of the quality of dying and nurse-assessed physician communication with both nurses and family members, unmeasured confounding or intervening variables might play a role in these associations. It addition, nurses might have had personal experiences caring for these patients that could result in moral distress potentially confound nurse ratings. 24 Nonetheless, these findings generate hypotheses that could be tested in future studies designed to improve communication.
Second, our nurse response rate was less than 60%, which might allow introduction of a response bias. Third, nurses were asked for their perceptions of physician-family communication. Although we included a “do not know” response so that nurses could choose to not rate a topic of communication about which they did not have enough experience to provide an assessment, the ratings that were provided may have been based on variable exposure to physician-family communication. Evaluation of these findings in a study design in which the exposure to physician-family communication is directly measured would provide an important test of our findings. Fourth, we did not assess for the presence of moral distress among participating nurses and were therefore unable to evaluate the effect that moral distress may have had on their ratings. 24 Fifth, study deaths occurred between 2003 and 2008 and ICU care might have improved since then; however, a prior analysis from this study suggests no improvement in the quality of palliative care during this time period. 36 Finally, this study took place in one region of the United States and may not generalize to other regions.
Conclusions
By examining the associations between nurse assessments of quality of dying for patients in the ICU and nurse evaluations of physician-family and physician-nurse communication, we identified several components of communication that were associated with higher nurse ratings of the quality of dying. When nurses report sharing information with their physician colleagues about family questions, family dynamics, spiritual considerations, and cultural considerations, nurses rate patients' quality of dying higher. When nurses perceive ICU physicians as helping families decide about treatments a patient would want, nurses also rate the patient's quality of dying higher. By contrast, when ICU nurses raise concerns about patient and family issues, these discussions are associated with lower ratings of the quality of dying, and might suggest the presence of obstacles to good-quality end-of-life care. Communication interventions targeted to create opportunities for physician-nurse exchange of patient- and family-specific information and physician-family communication that supports family decision making might be important targets for improving the quality of dying in the ICU.
Footnotes
Acknowledgments
Funding was provided by the National Institute of Nursing Research (R01 NR005226) and a grant from the Robert Wood Johnson Foundation. The funding agencies were not involved in the design, data collection, data analysis, data interpretation, writing of the manuscript, or in the decision to submit the manuscript for publication. The randomized trial is registered at ![]() : NCT00685893. The study was approved by the institutional review board or research oversight committee of all 15 institutions participating in the study: Swedish Medical Center/Ballard Stevens Hospital; Evergreen Medical Center; Highline Hospital/Highline Medical Center; Northwest Hospital & Medical Center; Overlake Hospital Medical Center; VA Puget Sound Health Care System; St. Joseph Medical Center; Swedish Medical Center Providence/Cherry Hill; Virginia Mason Medical Center; Valley Medical Center; Swedish Medical Center/First Hill.
: NCT00685893. The study was approved by the institutional review board or research oversight committee of all 15 institutions participating in the study: Swedish Medical Center/Ballard Stevens Hospital; Evergreen Medical Center; Highline Hospital/Highline Medical Center; Northwest Hospital & Medical Center; Overlake Hospital Medical Center; VA Puget Sound Health Care System; St. Joseph Medical Center; Swedish Medical Center Providence/Cherry Hill; Virginia Mason Medical Center; Valley Medical Center; Swedish Medical Center/First Hill.
Author Disclosure Statement
No competing financial interests exist for any of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.