
Abstract
Abstract
Background:
The American Academy of Pediatrics (AAP) and the American Academy of Hospice and Palliative Medicine (AAHPM) have recommended minimal standards for palliative care (PC) team composition and availability. It is unknown whether team composition affects utilization of PC.
Objective:
The study objective was to describe pediatric PC team composition, evaluate whether composition and availability are associated with utilization, and examine PC referral patterns.
Methods:
The study was a descriptive survey. Subjects were pediatric PC team directors or hospital administrators at Pediatric Health Information System (PHIS) hospitals (N = 44).
Results:
The overall response rate was 86%. Teams varied in size from <1 to 9 full-time members. Average referrals per hospital bed were 0.46, range 0.05–2.13. Among individual PC team roles, referral rates were 34% greater in teams with an advanced nurse practitioner (ANP) (p = 0.07). Likewise, teams with acute pain, chronic pain, or hospice palliative medicine specialists tended to have greater referral rates (39%, 36%, and 25%), though reported differences were not statistically significant. Teams adherent to the original AAP recommendations had a 31% greater referral rate (p = 0.22). Teams available 24 hours daily had similar referral rates to those with less availability (0.47 versus 0.46 [p = 0.94]).
Conclusions:
Team composition and availability are not crucial to PC utilization. Hospitals with some personnel but not all recommended team members should create formal teams and modify them over time. The addition of team members that tend to increase referrals, namely ANPs and acute pain, chronic pain, or hospice palliative medicine specialists, should be considered.
Introduction
P
PC teams may consist of many different types and numbers of members depending on the program age, resources available, and population base served. Little is known about the ideal size and team composition for adults or children. Hockley et al. hypothesized that in order to meet patient needs for an adult hospital with 800 beds, the PC team would need at least five members. 5 Both Ceronsky et al. 6 and Schrader et al. 7 discussed different team member types included on adult PC teams, but neither addressed what the ideal composition was for team function or service delivery. Currently there is a paucity of research outlining the appropriate size and ideal PC team composition for pediatrics. The AAP statement on PC recommended that teams be interdisciplinary and include a minimum of “a physician, nurse, social worker, spiritual advisor, and child life therapist.” 1 In 2010, the American Academy of Hospice and Palliative Medicine (AAHPM) outlined similar team composition for successful pediatric PC program development (excluding a child life specialist). 8 The AAP and the AAHPM also recommend that PC services be provided 24 hours a day, seven days a week.1,8 However, whether compliance with these recommendations leads to greater use of PC services is not known.
In addition to team member recommendations, the AAP suggested that PC team consultation occur early in a child's life-threatening illness rather than after curative treatment failure. 1 The goal of this is to enhance communication and support for families and children regardless of whether the child's illness is fatal. In order for this to happen, referrals should be made by primary care providers (PCP) or subspecialty physicians soon after initial diagnosis. It is unknown who makes most referrals to the PC team and when in the course of illness the referrals occur.
Our main objectives are to describe pediatric PC team composition at Pediatric Health Information System (PHIS) hospitals and evaluate the number of reported referrals to assess if team composition and availability are associated with referrals. Our secondary objective was to determine when in the course of a child's illness PC referrals are being made and which providers refer most often.
Methods
Study design
We designed and distributed a survey to 44 pediatric hospitals currently contributing to the PHIS, developed by the Children's Hospital Association, 9 (states represented include Alabama, Arizona, Arkansas, California, Colorado, Connecticut, Florida, Georgia, Illinois, Indiana, Louisiana, Massachusetts, Michigan, Minnesota, Missouri, New York, Ohio, Pennsylvania, Tennessee, Texas, Virginia, Washington, Wisconsin, and in Washington, DC). PHIS hospitals were a convenience sample, but they represent large children's hospitals across the United States. The survey questions were developed to address the study objectives. The survey was pretested by a small group (n = 5) from a survey methods course at the University of Utah and a group of 10 physicians from Primary Children's Hospital. After refinement, the survey underwent pilot testing at 10 U.S. pediatric hospitals not participating in PHIS. Pilot testing revealed no need for further adjustments, so the survey was converted into an electronic format. Study data were collected and managed using Research Electronic Data Capture (REDCap), a secure, web-based electronic data capture tool hosted at the University of Utah.10,11
The survey and a cover letter explaining the study objectives and assuring confidentiality were sent to the directors of pediatric PC teams for all 44 hospitals; if a hospital did not have a pediatric PC team, it was sent to a hospital administrator. To protect confidentiality, responses were not linked to the respondents' e-mail addresses. The survey was open for responses over an eight-week period from May to July 2013. Reminders were sent at two and four weeks, with a final reminder sent approximately one month later. Consent was indicated by participation. The University of Utah institutional review board reviewed and approved this research.
Statistical analysis
Statistical analysis was performed using SPSS 18.0 (IBM, Armonk, NY). Survey results were analyzed using descriptive statistics. In order to index PC referrals to hospital capacity, we divided reported PC referrals by hospital bed numbers at the responding institution for 2012 and compared this indexed mean to reported team composition as well as hours of PC team availability. Independent t-tests were used to compare teams with the recommended members to teams without these specific members. Statistical significance was based on a value of p ≤ 0.05.
Results
Respondents
The survey response rate was 89% (39/44); however, with one survey incomplete and excluded from the final analysis, the corrected response rate was 86% (38/44). Most of the responding 38 PHIS hospitals had PC teams (35/38, 92%); and the majority of respondents from these hospitals were PC team medical directors (26/35, 74%). Table 1 provides the demographics collected. The three hospitals without PC teams were similar in size to the hospitals with PC teams. Unfortunately, the hospitals without PC teams did not provide information regarding 2012 hospital deaths.
One missing value.
Three values missing, as the response was a percentage, instead of whole numbers.
IQR, interquartile range; PC, palliative care.
Team size and composition
Among responding hospitals, PC teams increased from 4, prior to 2000, to 35 in 2013. The reported number of current PC team members varied greatly by hospital, ranging from one part-time member to nine members (mean = 4.1). Most (83%) teams changed composition and number of members after initiation (see Table 2); for example, the number of advanced nurse practitioners (ANP) team members increased from 6 at time of PC team initiation to over 33 on current PC teams, while the number of hospitals with ANPs quadrupled (from 6 to 24). Less robust increases were found in the use of acute pain service (APS) members, child life specialists, physicians, and social workers. Currently, most PC teams include a physician member (33/35, 94%), totaling 80 physicians among all teams. The PC teams without changes were teams created within the last three years.
Fractions of team members as reported in survey (part-time equivalents were listed as fraction of full-time equivalent).
Others at initiation: Psychologist, bereavement specialist. Others currently: bereavement specialist, family partners group, mental health, music therapist, art therapist, pharmacist, physical therapist, occupational therapist.
ANP, advanced nurse practitioner; APS, acute pain service; CPS, chronic pain service; PC, palliative care.
Team composition/availability and palliative care referrals
The 2012 reported mean PC referrals was 135 (range 12–337) with an averaged indexed referral per hospital bed of 0.46 (range 0.05–2.13). We evaluated total number of team members with indexed referrals and found no consistent relationship (Pearson correlation = 0.184, p = 0.30). Figure 1 shows reported indexed referrals and team members. Specific team members appeared to influence referral numbers. For example, teams with a chronic pain service (CPS) member had 36% more referrals than teams without a CPS member (0.67 versus 0.43 [p = 0.45]); however, this difference was not statistically significant. Similar statistically insignificant increases were present among teams with APS staff (34%), ANPs (39%), and hospice and palliative medicine (HPM) physicians (25%) (APS: 0.65 versus 0.43 [p = 0.36]; ANP: 0.53 versus 0.32 [p = 0.07]; and HPM: 0.52 versus 0.39 [p = 0.34]).
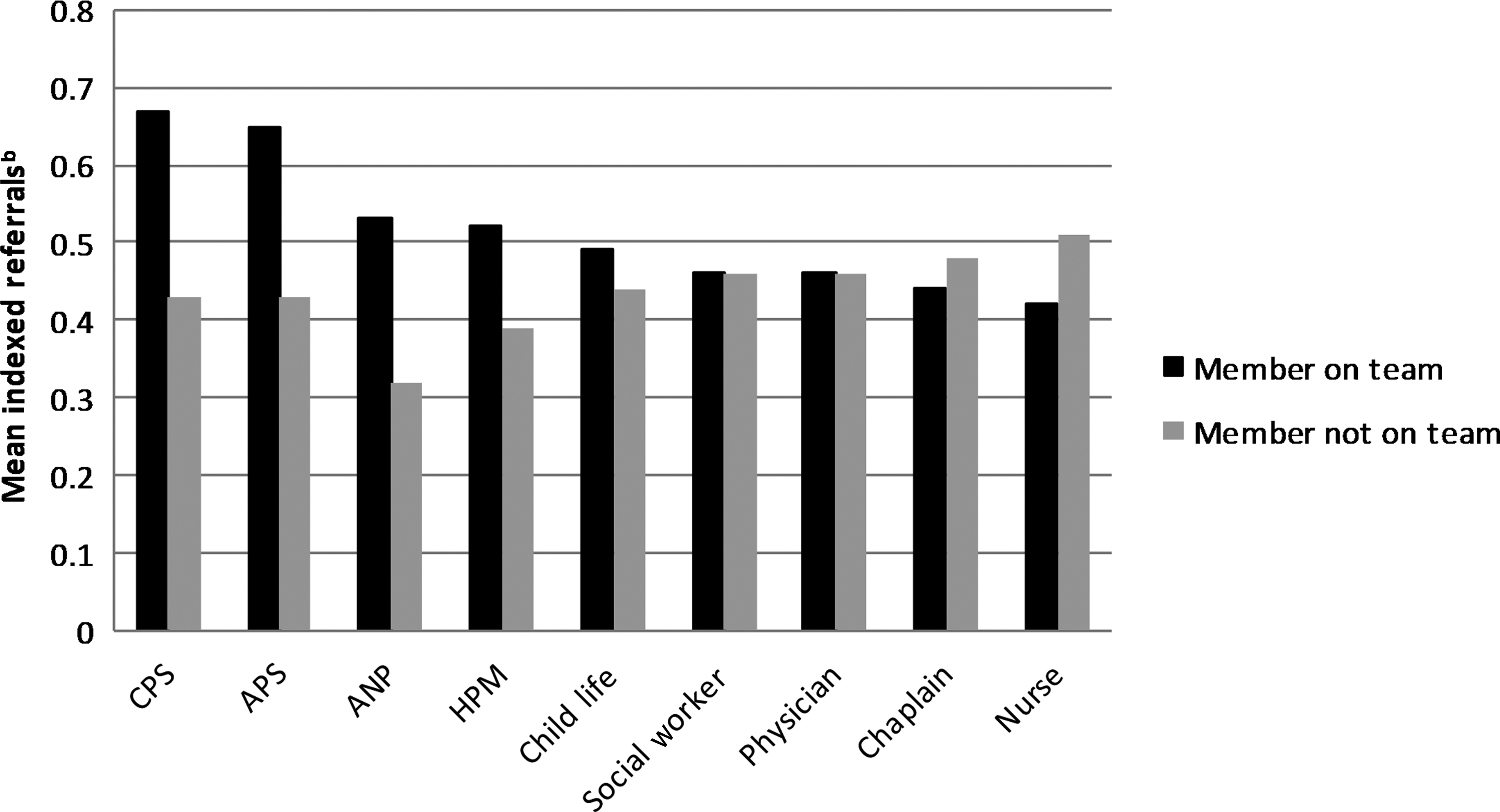
Mean referrals per hospital bed and team compositiona
Indexed referrals were examined as to whether the PC team included the members recommended by the AAP and the AAHPM. Ten teams (29%) currently include all members recommended by the AAP in 2000. As shown in Table 3, these teams had 31% more referrals than teams without these members; however, this increase was not statistically different (0.59 versus 0.41 [p = 0.22]). Fourteen teams (41%) include all members recommended by the AAHPM. There were no differences found with indexed referrals when comparing these teams to those without the AAHPM recommended members (0.41 versus 0.43 [p = 0.56]). Sixty-five percent of teams reported 24/7 availability. The amount of time teams were available was not associated with indexed referrals (0.47 versus 0.46 [p = 0.94]).
Recommended members include nurse and/or ANP.
AAHPM, American Academy of Hospice and Palliative Medicine; AAP, American Academy of Pediatrics; ANP, advanced nurse practitioner; SD, standard deviation.
Other services offered outside the PC team (bereavement services, spiritual support, hospice, music therapy, psychosocial support, sibling support, etc.) varied across hospitals. We found wide variation in hospital size and PC team member number in relation to the total services provided outside of PC team services.
Timing of palliative care referrals and providers who refer
In order to evaluate when in the course of a child's chronic illness the PC teams received referrals, we provided three specific time periods during which a PC referral could be made. These were (1) at the time of chronic illness diagnosis, (2) later in the course of the chronic illness but when curative treatments were ongoing (concurrent care), and (3) once all curative options were exhausted. Most (>60%) reported that currently <25% of referrals were made at the time of diagnosis, with only one hospital reporting these as the majority of their referrals. Sixty-three percent of respondents reported more than half of referrals were for children receiving concurrent care. Very few referrals were reportedly made after curative treatments were exhausted. Many (86% and 71%, respectively) reported increases over time in the number of referrals made at the time of diagnosis and for children receiving concurrent care.
We also examined which care providers tend to refer children for PC services and which do not. We found that the most common reported referrers to PC were subspecialists, followed by social workers, PCPs, ANPs, and nurses. Table 4 reviews the subspecialties that reportedly refer to PC most often, as well as those who tend to not refer. Most responders report physicians from pediatric intensive care (PICU) as one of the top referrers, followed by hematology/oncology (H/O). Endocrinologists, nephrologists, and gastroenterologists were reported as the least likely subspecialists to make referrals.
Other = geneticist (1), maternal fetal medicine (1), complex care/special needs physician (3).
Discussion
In this survey of more than 40 U.S. children's hospitals, we found that PC team composition varied greatly and that most teams changed, in regards to member types and total team members, after program initiation. We could not demonstrate significant differences in reported referrals by team composition or 24/7 availability, suggesting that hospitals should not delay initiation of PC teams. We also found that referrals made at the time of diagnosis although still low are increasing, while referrals made after curative treatments are exhausted are decreasing. Finally, respondents reported that most referrals come from subspecialists, specifically pediatric intensivists.
Most of the children's hospitals we surveyed reported having PC teams (35/44 respondents, 80%). These data confirm our previous work 12 using the PHIS database, where we found that 76% of PHIS hospitals used a PC code (V66.7) 13 in the year 2011. Other research also confirms increased PC team availability over time in both adult and pediatric hospitals.2,3 Slowly, access to PC services for pediatric patients with complex chronic conditions is becoming the standard for most children's hospitals.
To evaluate PC team utilization we chose to use indexed annual referrals per bed, as it was an easily ascertained measure. Using this measure we found that developing a PC team consisting of all AAP recommended members or members recommended by AAHPM may not be necessary in order to increase PC utilization. While we did find a trend in increased referrals with teams consisting of AAP recommended members, a similar trend was not found for teams consisting of the AAHPM recommended members. We were unable to identify any prior work evaluating PC team composition and utilization. Our findings suggest that hospitals should not delay the development of a PC team until they are able to fully staff a PC team with the recommended members. Hospitals should be encouraged to start PC programs with the resources they have available and then add necessary members over time. In support of this, our findings show that once teams were established, they usually added members over time. This indirectly supports the updated 2013 AAP recommendation recognizing the initial development of PC teams that have only a few members and stressing that team composition should change over time to include the recommended members. 14 Once able to grow an established PC team, our findings suggest that the addition of certain team members, notably ANPs, pain team physicians, and HPM physicians, may increase the number of referrals made to the PC team.
Although prior research on PC team composition is limited, Feudtner et al. conducted a national survey of children's hospitals evaluating PC team composition. 15 Similar to our findings, they reported a broad range in the number of consultations per year, mean consultations per hospital bed, and total number of consultations per hospital bed. Unlike our study, they found an increase in consultations with an increased number of full-time equivalent PC team clinicians. Also similar to Feudtner et al. 15 we found that two-thirds of our respondents had PC programs that provided 24/7 availability. Our study showed that PC referral rates were similar whether ’round the clock coverage was available or not. Previous work has identified the recommendation of 24/7 availability as a barrier to PC team development. 16 Although 24/7 coverage is considered ideal, based on this new data, it should not be viewed as a deterrent to PC team development.
In our study, respondents reported that <25% of their referrals are made at the time of diagnosis. The AAP recommends that children with a life-threatening condition be offered PC at the time of diagnosis. 1 Offering PC early in the illness provides time for development of relationships, enhances transitions of care, and likely increases trust when the family faces end-of-life decisions. There have been several studies documenting barriers to PC referral for children, one of which is uncertain prognosis.17–19 Unfortunately the trajectory of illness in pediatrics is very difficult to predict. In a review of pediatric deaths it was shown that only 22% of the deaths were anticipated, even though many of the children had chronic illnesses. 20 Fortunately we found that although early referrals were low, these referral types tended to increase over time after the development of a PC team. Another barrier to early referral is the belief that PC is only beneficial after all curative options are exhausted.17–19 A promising finding of our study was that these referral types made up a small percentage of referrals, and referrals made while patients were receiving curative care increased after PC team development. This indicates a possible change in belief around curative versus PC. Several studies have highlighted the importance of integrating PC with curative care.21,22 These findings are encouraging and highlight the need for PC team development, so that services can be provided early, while curative therapies are ongoing.
We found that hospital-based subspecialists were much more likely to refer a patient to PC than PCPs were. We believe this is the first study to report physician specialty and PC referral. These findings are consistent with a previous study showing that children with neonatal and cardiac diseases were the least likely to have a PC code billed prior to their death. 12 It is not surprising that PICU and H/O physicians refer often to PC, as they care for many patients with chronic illness. As most children who die in the hospital are <1 year old, 12 the number of referrals from neonatologists could be much higher, as could referrals by other subspecialists, given the AAP recommendation that all children with life-threatening illnesses be offered PC. Contrary to this, we found very few reported referrals come from subspecialists in endocrinology, nephrology, gastroenterology, and cardiology. This may be related to the amount of time subspecialists spend in the hospital setting versus the outpatient setting—but overall, highlights the need for educational efforts to detail the model of concurrent curative and PC for children with life-threatening chronic illness.
Our study has limitations to consider. First, the study design is a survey that asked for respondents' opinions and data, which may not be accurate. However, the requested information was likely readily available information for the PC team. The majority of our respondents were PC team medical directors (74%), which may increase data accuracy; however, our analysis to determine referrals per bed was predicated on the number of referrals reported, and if these were inaccurate it would decrease precision. Second, in regards to reported referrals, it is unknown if they represent total referrals made to the PC team or if they represent only referrals that resulted in the addition of new patients to their PC service. Additionally, we do not have information on the reason the referrals were made or what limitations underlie referrals to the team (i.e., whether referrals are limited to symptom management). Third, although we had a remarkably high response rate, it is still a small sample size, which likely led to our lack of statistically significant findings. Fourth, while the PHIS hospitals represent a variety of children's hospitals across the United States, they are mostly large children's hospitals, with only two respondents from hospitals with <150 beds; this limits the generalizability of this information to smaller hospitals. Fifth, it is unknown whether the nonrespondents were from hospitals with or without PC teams. This may represent a respondent bias. Finally, the AAP revised their recommendations for team composition after development and administration of our survey. The updated recommendation for “mature teams” includes a bereavement specialist, 16 which we did not specifically ask about in our survey.
In conclusion, we found that team composition and availability may not be critical to PC team utilization and should not be viewed as deterrents to initial PC team development. Hospitals with some of the needed personnel but not all team members recommended by the AAP and AAHPM should consider creating formal teams. As these teams grow, they will need increasing support in order to meet patient and family needs as well as mitigate provider burnout. The addition of specific members to the team, such as an ANP, HPM physicians, and pain management physicians, may increase referrals. It is encouraging that PC referrals are occurring closer to the time of initial diagnosis; however, there is still room for improvement if we are to provide optimal care to children with life-threatening illnesses.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or disclosures to make. No competing financial interests exist.