
Abstract
Abstract
Background:
The effectiveness of home hospice care was helping patients to die at home, and reducing symptom burden.
Objective:
The study objective was to explore the impact of home hospice care on death at home, end-of-life (EOL) care, and health care costs among patients with advanced lung cancer in their last month of life.
Methods:
Using Taiwan's National Health Insurance Claims Database, we analyzed factors associated with home hospice care using logistic regression analysis.
Results:
We enrolled 568 patients with advanced lung cancer under hospice care who died during 1997–2011, of which 238 (41.9%) received home hospice care. Compared with the inpatient hospice (IH) group, the home hospice (HH) group had a larger portion die at home (55.5% versus 22.1%, p < 0.001), but a smaller portion stayed in hospital more than 14 days in their last month of life (67.3% versus 40.8%, p < 0.001). The mean health care cost was less in the HH group than in the IH group (US $1,385.00 ± $1,370.00 and US $2,155.00 ± $1,739.00 [p < 0.001], respectively). Female patients' (p = 0.001) decreased hospital stay in the last month of life (p < 0.001) and longer hospice care duration (p = 0.003) were predictors of receiving home hospice care in advanced lung patients.
Conclusion:
Home hospice care enables patients with advanced lung cancer to increase the 33.4% chance of dying at home, to spend an average of eight-days less in hospital stay, and to save 35.7% health care costs in the last month of life, compared with their counterparts with only inpatient hospice care. Female patients' decreased hospital stay and longer hospice care duration were the predictors of receiving home hospice care.
Introduction
D
Despite advances in early diagnosis, treatment, and survival, cancer remains a leading cause of death in most developed countries. 1 With the increasing number of deaths from cancer, the inevitable need for high-quality EOL care has become increasingly important. A number of measures of high-quality EOL care have been developed and reported previously;10–11 these assess outcomes, such as receiving chemotherapy during the last two weeks of life, having more than one emergency room (ER) visit in the last month of life (LML), being admitted to a hospital more than once in the LML, receiving care in an intensive care unit (ICU) in the LML, receiving CPR in the LML, and dying in an acute care hospital. 12 These EOL care quality indicators have been adopted in the United States,11–12 Canada, 13 and Taiwan; 6 and these six indicators are considered to indicate aggressive EOL cancer care. More aggressive EOL care is considered inappropriate for the dying. Therefore, measuring these indicators is crucial for evaluating the quality of hospice care programs, including home hospice.
Over the past two decades the treatment of cancer patients near death has become increasingly aggressive with the hope of extending survival.6,10,14 Some people who believe that hospice care is performed to relieve pain and suffering but not extend life are concerned that hospice care may in fact hasten death. 15 However, previous studies have reported no reduced survival in patients with advanced cancer.16–17
EOL care imposes a heavy economic burden on patients, their families, and the health insurers. The impact of EOL care-related costs on patients with cancer has been frequently discussed, and numerous studies on health administrative data have been published since 2000. 18 Cancer care related costs are the highest in the initial period after diagnosis and in the last year of life, and decreases in the continuing phase follow a U-shaped curve. 19 Chastek et al. reported that health care costs are the highest in the last month of life in patients with cancer. 20 A review study reported that palliative care was most frequently found to be less expensive than nonpalliative care. 21 Previous studies have reported that home hospice care is a cost-saving alternative to inpatient hospital care worldwide, including the United States, 22 Canada, 23 and other countries.24,25
Lung cancer has been the most common cancer in the world for several decades. In addition, it is the most common cause of cancer-related death, with a share of 18.2% among other cancers. 26 Moreover, lung cancer was the leading cause of cancer death in Taiwan, constituting 19.7% of overall cancer deaths in 2012. 27 Therefore we explored home hospice use in patients with advanced lung cancer.
The aim of this study was to examine the impact of home hospice care on place of death, quality of EOL care, health care costs, and survival in patients with advanced lung cancer during the last month of life and to determine the predictors of receiving home hospice care.
Methods
Data source
In this nationwide population-based retrospective cohort study, we analyzed data obtained from the Taiwanese National Health Insurance Research Database (NHIRD). The National Health Insurance (NHI) program, implemented in March 1995, is a single-payer health insurance system in Taiwan covering approximately 99.9% of the total population in 2012. 28 The NHIRD, a nationwide representative database containing all original claims data for one million NHI beneficiaries from 1996 to 2012, is a randomized, systemic sample of the 23.32 million NHI enrollees. According to the Registry of Catastrophic Illness Database, a subpart of the NHIRD, patients with cancer are designated as those having a catastrophic illness and issued a Catastrophic Illness Certificate. We used the NHIRD to identify patients with lung cancer; the catastrophic illness database to identify patients receiving hospice care; and the insurance system exit date, which is our proxy for death. We followed patients up to December 2012 by using the Longitudinal Health Insurance Database 2000 (LHID2000), a subset of the NHIRD containing all the original claims data from the one million individuals randomly sampled from the NHIRD in 2000.
Definition of variables
Home hospice care group (HH group) and only inpatient hospice group (IH group)
We searched the claim data for the charge codes of inpatients' hospice care and home hospice care. Among the claim data, patients with the codes for inpatient hospice care and without the codes for home hospice care were classified as the IH group. If patients were with the codes for home hospice care, they were classified as the HH group. Accordingly, these inpatient hospice units also served as the back-up system for patients receiving home hospice care when they experienced exacerbating symptoms that required further readmission to the hospice unit or whose families needed respite care from caregiving.
Quality indicators of EOL cancer care
The clinical impact of hospice care services for adult patients with terminal illnesses and their family caregivers is defined according to symptom control, quality of life, caregiver distress, and satisfaction with care. Previous studies have reported that quality indicators for hospice care included symptoms related to cancer, such as pain, dyspnea, and depression; treatment-associated toxicities (e.g., diarrhea, delirium, skin rash); information and care planning (e.g., advance directive or a surrogate decision maker); communication about chemotherapy; and psychosocial care.29–32 In this study, information on symptom control, communication about chemotherapy, and psychosocial care was unavailable in the NHIRD data; therefore, we used the following indicators to appraise the quality of EOL cancer care. These quality indicators are outlined as followed: (1) receiving chemotherapy during the final two weeks of life, (2) having more than one ER visit, (3) being admitted to a hospital more than once, (4) receiving care in an ICU during the final month of life, (5) receiving cardiopulmonary resuscitation (CPR) during the final month of life, and (6) dying in an acute care hospital.10–11
Death in a hospice ward
If the date of discharge for the last admission was the same as the date of death, 33 then the patient was considered to have died in the hospice ward. In Taiwan, hospice wards belonged to acute care hospitals. Patients who died in hospice wards received care and bereavement service for their families, unlike those who died in other acute wards.
The socioeconomic status (SES) of an individual
On the basis of previous studies,34–35 we classified SES into three groups: low, moderate, and high. Those earning less than U.S. $571.00 per month, between U.S. $571.00 and U.S. $1,141.00, and more than U.S. $1,141.00 per month were included in the low group, moderate group, and high group, respectively.
Charlson comorbidity index (CCI)
CCI was calculated by examining the ICD-9-CM diagnosis and procedure codes recorded in the year prior to diagnosis, according to the Deyo method, and applying them to inpatient and outpatient claims as described by Klabundle et al.36–38
Survival probability after diagnosis
Survival was defined as the time from cancer diagnosis to death. The Kaplan-Meier estimate is used to measure the probabilities of subjects living for a certain amount of time after diagnosis. 39
Health care costs
The health care cost of each patient was categorized into inpatient and outpatient services. We converted costs on the basis of the U.S./N.T. exchange rate in 2006 (U.S. $1.00 = N.T. $32.53).
The study protocol was reviewed and approved by the Research Ethics Committee of the Buddhist Dalin Tzu Chi Hospital, Taiwan (No. B10301001). Because the NHIRD files only contained deidentified secondary data, the review board waived the requirement for informed consent.
Statistical analysis
Statistical analysis was performed using R 3.0.2 software (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p value ≤0.05 was considered significant. The survival (years) was defined as the duration from the day of diagnosis to the day of death (in years). The survival probabilities were analyzed by the Kaplain-Meier method and tested by log rank test. The distributional properties of continuous variables were expressed in mean ± standard deviation (SD), and categorical variables were presented in frequency and percentage. Univariate analysis, two-sample t test, Wilcoxon rank-sum test, chi-square test, and Fisher's exact test were employed to examine the differences in the distributions of continuous variables and categorical variables between the two groups.
Multivariate analysis was performed by fitting multiple logistic regression models with a stepwise variable selection procedure to identify the crucial predictors of home hospice care during the last month of life. Generalized additive models (GAMs) were fitted for detecting potential nonlinear effects of continuous covariates and identifying appropriate cutoff points for discretizing continuous covariates, if necessary, during the stepwise variable selection procedure. 40
The goodness-of-fit (GOF) of the final logistic regression model was assessed and the Hosmer–Lemeshow GOF test was checked. Finally, the statistical tools of regression diagnostics for residual analysis were applied, influential cases were detected, and the multicollinearity was assessed to identify problems with the model or data.
Results
We enrolled 568 patients with advanced lung cancer. Among them, 330 (58.1%) patients received only inpatient hospice care (IH group), and 238 (41.9%) patients received both inpatient and home hospice care (HH group). The mean (median) home hospice visits were 6.6 ± 7.9 (3.0). The study flowchart is shown in Figure 1. No significant difference for survival probability was observed following advanced lung cancer diagnosis between the HH group and IH group (log rank test, p = 0.467) (see Fig. 2). The median days after hospice enrollment were longer in the HH group than in the IH group (39.5 versus 17.0, p < 0.001). As shown in Table 1, the HH group had a higher portion of female patients (47% versus 32.4%, p < 0.001); a smaller portion of residents in the northern area in Taiwan (25.6% versus 36.4%, p = 0.008); and a higher portion of residents in the southern and eastern areas (49.2% versus 39.1%, p = 0.020) than the IH group. No other significantly different characteristics were observed in both groups (see Table 1).

The study flow chart. CIC, catastrophic illness certificate; ICD-9-CM, International Classification of Diseases, 9th rev., Clinical Modification.
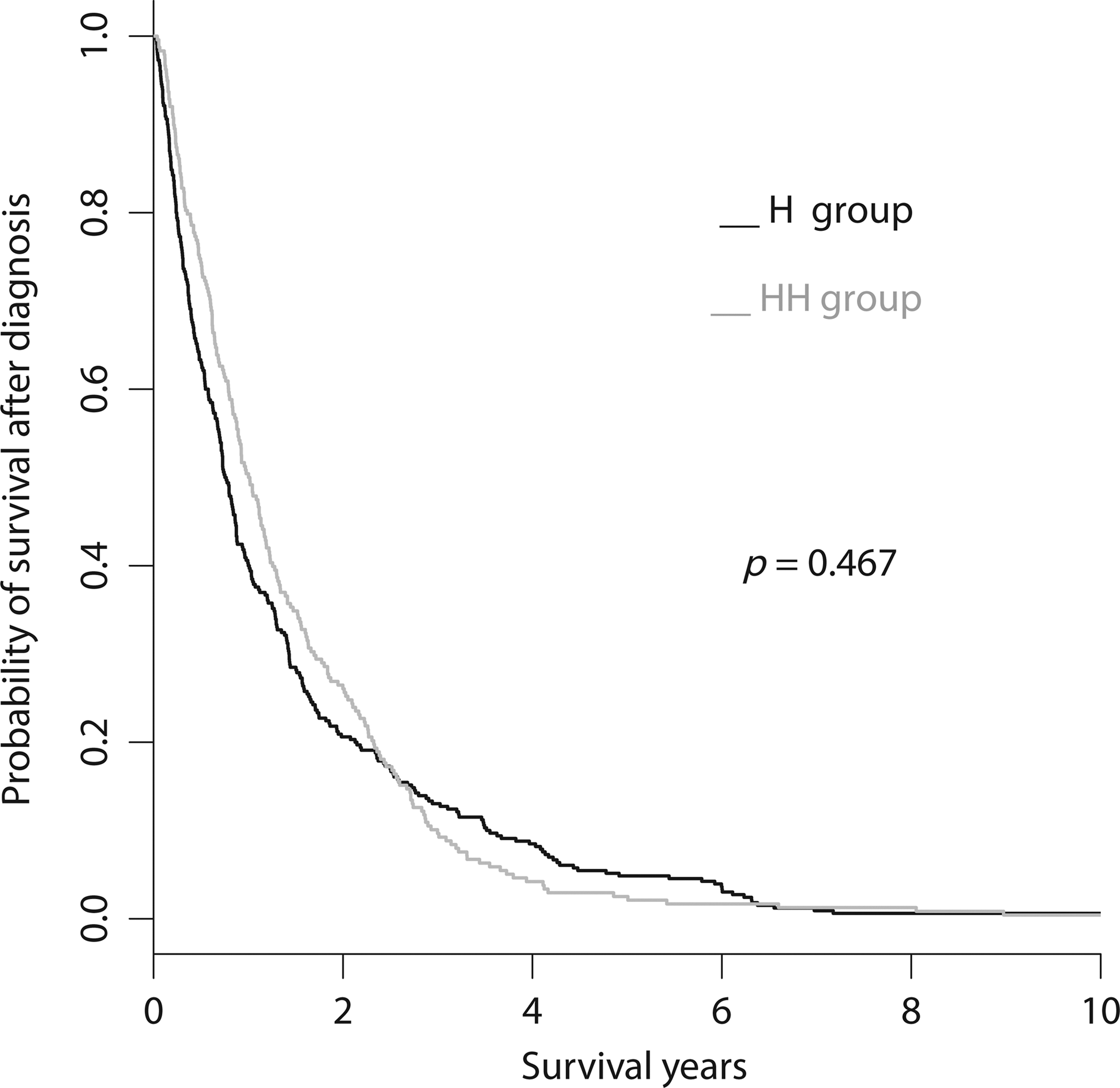
The survival curves following lung cancer diagnosis for patients in the home hospice group (HH group) and only inpatient hospice group (IH group).
CCI, Charlson comorbidity index; CKD, chronic kidney disease; CVA, cerebral vascular accident; HES, high SES; HH group, home hospice care group; IH group, inpatient hospice care only group; LES, low SES; MES, moderate SES; SES, socioeconomic status.
Aggressiveness of EOL care was compared between the HH and IH groups (see Table 2). The median days of hospital stay in the last month of life were fewer in the HH group than in the IH group (10.5 versus 22.0, p < 0.001). The HH group spent an average of eight days less in hospital stay than the IH group. Compared with patients in the IH group, the HH group had a significantly larger proportion of death at home (55.5% versus 22.1%, p < 0.001); and a significantly smaller proportion of the patients in the HH group had more than 14 days of hospital stay in the last month of life (40.8% versus 67.3%, p < 0.001). The mean health care costs in the last month of life were significantly less for patients in the HH group than for those in the IH group (U.S. $1,385.00 ± $1,370.00 versus U.S. $2,155.00 ± $1,739.00, p < 0.001). No significant differences were observed for other EOL care quality indicators between the two groups.
Patients had no hemodialysis history before the last month of life.
ER, emergency room; HH group, home hospice care group; ICU, intensive care unit; IH group, inpatient hospice care only group.
From the multivariate logistic regression model, the significant predictors for home hospice care were females (female versus male odds ratio [OR]: 1.87, 95% confidence interval [CI]: 1.28–2.72, p = 0.001); decreased hospital stay in the last month of life (OR: 0.93, 95% CI: 0.91–0.95, p < 0.001); and longer hospice care duration (per five days, OR: 1.02, 95% CI: 1.01–1.03, p = 0.003) (see Table 3). The adjusted generalized R2 (Nagelkerke R2) was 0.224. This model was evaluated and approved according to the Hosmer–Lemeshow test (p = 0.289), and the AUC was 0.745.
Nagelkerke's R2 = 0.224. Hosmer-Lemeshow test was passed (p = 0.289). AUC = 0.745.
In the last month of life.
AUC, area under the curve; CI, confidence interval; OR, odds ratio.
Discussion
In this study we found home hospice care increased the 33.4% chance of dying at home, and enabled patients with advanced lung cancer to spend an average of eight days less in hospital stay, save 35.7% health care costs in the last month of life, and not compromise on survival, compared with their counterparts with only inpatient hospice care. Female patients, decreased hospital stay, and longer hospice care duration were the predictors of receiving home hospice care.
Globally, hospice and palliative care are now well established.41–42 We mainly focused on the quality indicators of EOL cancer care. Inpatient hospice patients with cancer were significantly less likely to be intubated and receive mechanical ventilator support during EOL care, as reported in a previous study. 43 In this study we observed that patients in the HH group were significantly less likely to have more than 14 days of hospital stay and die in a hospice ward than those in the IH group. However, no significant differences were observed for other EOL care quality indicators between these two groups.
Health policies around the world have viewed home as a panacea for a place to die, and attempts are made for shifting the stay from hospitals to homes, thereby enabling more people to be cared for and to die at home. 44 A prospective study reported that patients with cancer who died in a hospital experienced more physical and emotional distress and had a lower quality of life than those who received home hospice care. 45 A study in Taiwan reported that most advanced cancer patients and their family caregivers preferred that the patients died at home (61.0% and 56.9%, respectively). 46 However, another study reported that the percentage of hospital deaths in patients with terminally ill cancer was 65.4% in 2006. 6 A previous study discussed the reasons Taiwanese hospice patients want to stay in hospital from the perspective of health care professionals, and the resolutions for above situations included to arrange the hospice home care program and explain the goals of inpatient care. 47 In this study we found home hospice care enabled patients to die at home, similar to previous studies.3–4 It was one of the benefits of home hospice care services for patients with advanced cancer.
In the current study we also found that the IH group had a higher portion of residents in the northern area in Taiwan, and the HH group had a higher portion of residents in the southern and eastern areas than the compared group. The explanation might be that most resources are allocated in North Taiwan, resulting in a geographic disparity due to unbalanced health care resource allocation. 48 This reminds policy-makers that the equality of medical resources and necessary medical services should be guaranteed in health care policy in order to achieve the goal of health, for human rights has always been the health system's mission.
High diversity exists in palliative care provision models and health insurance systems in different countries. The reimbursement of home hospice and inpatient hospice care in Taiwan differs from those in other countries. Home hospice care is paid at a fixed rate per visit (from U.S. $42 to U.S. $48 based on the time spent on the visit), and inpatient hospice care is paid at a per day rate of U.S. $142.00. A previous study reported that patients under home hospice care incurred less costs and had more savings than those under only inpatient hospice care in their last week of life. 49 In this study the mean savings in health care costs of patients in their last month of life in the HH group was 35.7% when compared with the IH group. The costs savings may be caused by the decrease in the length of the hospital stay.
Some practitioners and patients argue that hospice may hasten death. 15 A previous study reported that the use of hospice and the length of hospice stay for patients with advanced lung cancer did not compromise their survival.14,50 In this study no significant differences were observed in the survival probability between the two groups. Following hospice enrollment, patients in the HH group had 22 more median days after hospice enrollment compared with those in the IH group (39.5 days versus 17.0 days, p < 0.001). It's possible that the sicker population of patients and insufficient caregiver support were in the IH group than the HH group.The mean home hospice visits were 6.6 times and the mean rehospitalization was 1.1 ± 1.7 times following hospice enrollment.
The decision regarding place of EOL care is complex, with multiple competing factors being considered. In this study we identified the three predictors of receiving home hospice care for patients with advanced lung cancer. Female patients were more likely to receive home hospice care; this finding was similar to the result of a previous study. 51 The greater use of home health care among women was possibly explained by their greater health care needs; they were less likely to have a hospital stay and had fewer physician visits than men. 52 On the other hand, the Carlsson et al. study reported that women to a lesser degree died at home than men. 53 This different results might be due to different contexural and cultural factors. The second predictor was that the shorter duration of hospital stay of patients during the last month of life was associated with home care. A similar finding was reported by a meta-analysis study showing a small to moderate beneficial effect of home care on reduction in hospital days. 54 The reason might be home hospice services support families to sustain patient care at home. 55 The last predictor was that longer hospice care duration was associated with higher probabilities of home hospice care. In this study the median enrollment days in the HH group were longer than in the IH group (39.5 versus 17.0 days). The possible reasons might be the patients' surviving long enough to get this service, being familiar to the home hospice care team during inpatient hospice service, and home being the patients' preferred place of death.
Prognostication of life expectancy is one of the core skills in practice of medicine for clinicians involved in oncology and palliative care.56–57 However, clinicians receive little information during their clinical training on how to evaluate the accuracy of survival estimates. 58 A systemic review study reported that some significantly prognostic factors, such as performance status; symptoms associated with cancer anorexia-cachexia syndrome (weight loss, anorexia, dysphagia, and xerostomia); dyspnea; delirium; and some biologic factors (leukocytosis, lymphocytopenia, and C-reactive protein). 57 In this study we found that the female patient was a negative predictor of survival after hospice enrollment, with a similar finding also reported in a previous study.58–60
This study has some limitations. First, we did not include patients under the age of 20 years; therefore the current results cannot be generalized to younger patients. Second, the study was a retrospective design. Third, some misclassification bias might exist because of the accuracy of some of the variables used, including the calculation of the comorbidity score. Fourth, possible selection bias might be present because the study was not randomized. Lastly, reasons for referral to home hospice care and readmission to the hospice ward were not obtained from the claims database.
Conclusion
Home hospice care increase the 33.4% chance of dying at home, and enabled patients with advanced lung cancer to spend an average of eight days less in hospital stay, save 35.7% health care costs in the last month of life, and not compromise on survival, compared with their counterparts with only inpatient hospice care. Female patients, decreased hospital stay, and longer hospice care duration were the predictors of receiving home hospice care. Accordingly, policy for promotion of a home hospice program might optimize EOL cancer care.
Footnotes
Acknowledgments
This study is based partly on data from the NHIRD provided by the NHI bureau, Department of Health, which is managed by the National Health Research Institutes (NHRI). The interpretation and conclusions contained herein do not represent those of the NHI, Department of Health, or NHRI. J. K. Chiang received research grants from Buddhist Dalin Tzu Chi Hospital (DTCRD 102(2)-E-01, 103(2)-E-03).
Author Disclosure Statement
The authors declare that they have no competing interests.