
Abstract
Abstract
Background:
The high prevalence of complementary and alternative medicine (CAM) use among patients with cancer can be explained by reasons such as growing scientific evidence and improved regulation. However, subjective considerations are also relevant for practicing CAM and perceiving its effectiveness. The current study aimed at qualitatively estimating patients' prior beliefs and expectations, as well as their level of satisfaction after the treatment.
Patients and methods:
Patients with cancer who received six weekly sessions of CAM during their oncologic treatments participated in the study. They detailed their prior expectations and their level of posttreatment satisfaction. The open-ended answers were analyzed using interpretative phenomenological analysis. In addition, the contents before and after the intervention were compared.
Results:
Over a 2-year period, 163 patients entered the study, 135 of whom completed all six CAM sessions. The content analysis of the pretreatment expectations revealed four main categories: emotional, physical, external, and aspects related to the practice of CAM. After the intervention, patients referred to the therapeutic encounter as a significant aspect, in addition to the emotional and physical ones.
Conclusion:
CAM sessions encouraged emotional and relational aspects in patients' perspectives, which may be highly relevant for their coping process. Encouraging personal motives may increase treatment efficacy and ensure optimal use of health care resources.
Introduction
C
Approximately half of the patients with cancer worldwide use CAM as part of their oncologic care. 3 This high prevalence of CAM use can be explained by the growing scientific evidence regarding its efficacy in improving various physiologic and psychologic parameters among patients with cancer, such as distress and depression, 4 pain, 5 reduction of treatment side effects, 6 and enhanced immune regulation. 7 In addition, the integration of CAM services into health care systems and the improved regulation of practitioners and practices encourage patients with cancer to participate in such services as part of their cancer care.3,8
However, the willingness of patients with cancer to practice CAM therapies can also be related to more personal and subjective reasons, such as their health beliefs,9–12 their beliefs regarding the risks and benefits of CAM use8,11,13–17 as well as the conventional treatment,3,8,14,18 and their past experiences.3,8
Personal and subjective parameters may also influence patients' posttreatment satisfaction and perceived effectiveness, and these are unnecessarily related to objective scales and outcomes.19,20 For example, patients with cancer reported the importance of the humanistic attitude and the sense of “togetherness” as part of the therapy effect. Another study demonstrated that patients with cancer perceived CAM effectiveness as an increased sense of control over the disease. 21 In addition, aspects of personal empowerment and increased hope were found to be highly significant. 22
In Israel, the use of CAM by patients with cancer has grown steadily in the recent decades.23–25 It was found that various personal–emotional aspects were involved in the experience of CAM care by Israeli patients with cancer and their attitudes toward it. For example, Paltiel et al. 23 found that CAM use was related to patients' unmet needs by health care, lack of trust, or sense of hopelessness, in addition to common demographic ones, which were found in studies worldwide (e.g., female, higher level of education). Another study found that patients' perspectives regarding CAM included emotional factors, such as a sense of confidence, emotional resilience, and empowerment. 26
Similar to other Western countries, the oncology field in Israel is progressing toward personalized medicine, which tailors treatment strategies according to each patient's medical and genetic information. This trend should be implemented in other aspects of oncologic care, including palliative services and CAM, in order to ensure whole-person care, tailored to the patient's needs and perspectives.
Given the importance of the patient's subjective point of view regarding CAM, specifically in Israel, the current study aimed at qualitatively estimating patients' prior beliefs and expectations, as well as their perceived contribution and level of satisfaction after the treatment. It evaluated the main reasons that encourage patients to practice CAM, and the aspects that were achieved after the treatment as perceived by the patients. In addition, it examined possible differences between pre- and post-perspectives, to evaluate the degree of satisfaction and possible changes in patients' main preferences. This article presents a qualitative investigation as part of a large-scale study carried out in the Division of Oncology at Rambam Health Care Campus (RHCC) in Haifa, Israel. The quantitative study demonstrated that six weekly CAM sessions significantly improved levels of anxiety and depression, fatigue, and global quality of life, an effect that lasted 6 weeks at least after completion of sessions. 27
Methods
Setting and participants
The CAM unit was established in 2004 as an integral part of the Division of Oncology at Rambam Health Care Campus (RHCC) in Haifa, Israel. A senior oncologist and a nurse supervise the service that includes the following therapies: art therapy, music therapy, guided imagery, Reiki, shiatsu, healing, cranio-sacral therapy, and oil anointing. The treatments are provided as part of the service for oncology patients and are free of charge. Information regarding this service is displayed in the Division of Oncology and patients can self-refer to it. Some are referred by staff members. The patients meet with a nurse who evaluates their medical and emotional state and discusses their personal preferences regarding the treatments. They receive six weekly sessions of one type of treatment, according to a waiting list.
The sample included patients with cancer who approached the CAM unit. Inclusion criteria were more than 18 years of age, willing to sign an informed consent form, good performance status (2 or below on a scale of 0–4 with 0 denoting perfect health and 4 full disability), 28 willing to complete the questionnaires, and Hebrew literacy. Exclusion criteria were inability to commit to six sessions and brain or nervous system metastasis.
Measurements
Before the start of therapy, all patients answered a written open-ended questionnaire that included two questions: “Why did you choose to practice CAM?” and “What are your expectations regarding the treatment?” Six weeks after the end of the treatment, patients answered the following open-ended question: “Did the treatment fulfill your prior expectations?”
Data analysis
The patients' answers were analyzed according to the Interpretative Phenomenological Analysis (IPA) method, which aims to investigate people's subjective point of view and perceptions, while emphasizing the way they make sense of their personal and social world. 29
According to this method, patients' answers regarding their prior expectations were read closely more than once. The main topics of each answer were identified and any significant key words were marked. These topics were then conceptualized into themes, concise phrases that aim to capture the essence of the text and represent a slightly higher level of abstraction. In the next phase, the list of themes was observed to establish theoretical or analytical connections between them and to compose the superordinate themes. 29 In the current study, the superordinate themes represented the main dimensions of patients' expectations. The same procedure was carried out on the posttreatment answers, and it composed the main aspects of satisfaction as perceived by the patients.
After completing the IPA analysis, the pre- and post-answers of each patient were compared in order to reveal possible connections between the two time points or any difference in patient preferences and point of view regarding CAM.
Results
Demographic and medical characteristics
Over a 2-year period, 163 patients entered the study and 135 completed all six CAM sessions. Table 1 details the characteristics of the entire sample and the percentages of participants who completed the treatment sessions. Most of the patients were female, more than 60 years of age, and had more than 14 years of education. Participants with more than 11 years of education were more likely to complete the sessions than those with 10 or fewer years based on research data from Bar-Sela et al. 27 The distribution of CAM therapies among study participants is shown in Figure 1.

Complementary and alternative medicine (CAM) therapies distribution among participants.
Based on research data from Bar-Sela G, Danos S, Visel B, et al.: The effect of complementary and alternative medicine on quality of life, depression, anxiety, and fatigue levels among cancer patients during active oncology treatment: Phase II study. Support Care Cancer 2015;23:1979–1985.
Expectations regarding CAM
The content analysis of the pretreatment expectations revealed four main aspects reflecting the reasons for choosing to participate in CAM therapies and patients' expectations (Fig. 2):
4.
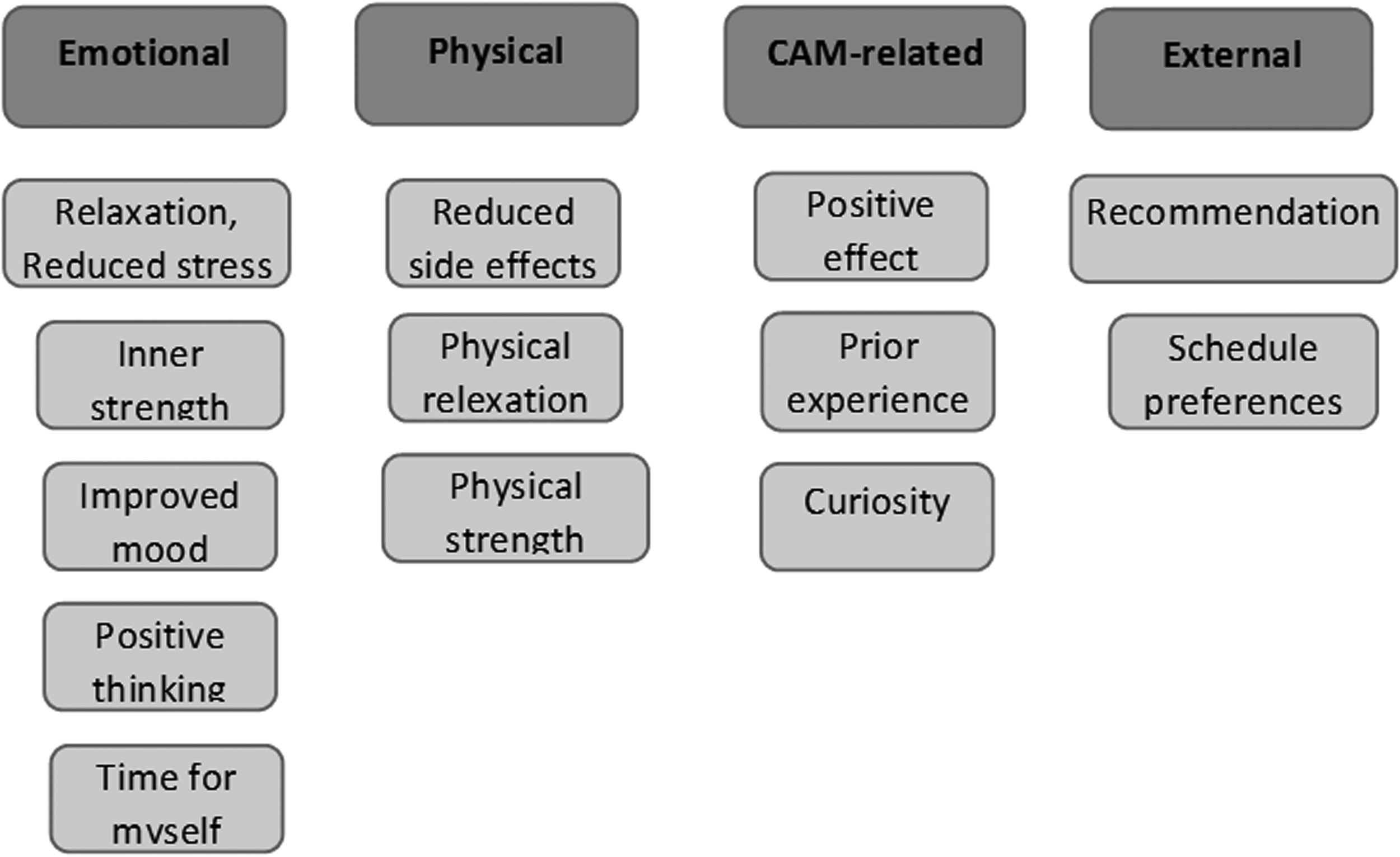
Patients' expectations prior to complementary and alternative medicine (CAM) treatment.
Satisfaction regarding CAM
Of a total of 135 patients who completed the sessions, 4 patients reported that the therapy did not fulfill their prior expectations; all of these patients approached CAM services due to a recommendation (an external reason). All other patients expressed their satisfaction in three main aspects (Fig. 3):
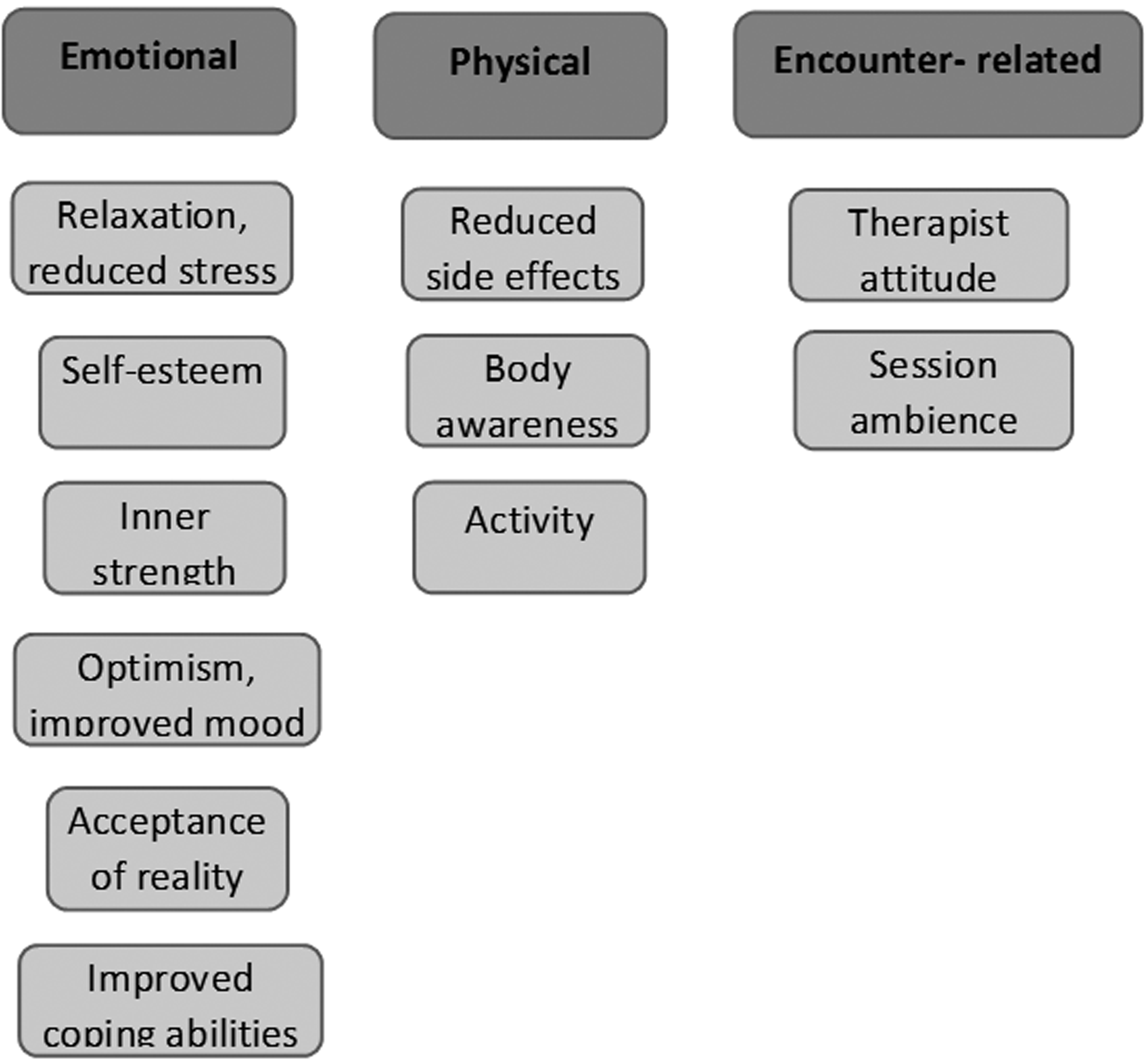
Patients' posttreatment satisfaction.
Comparing before and after treatments
Most of the patients referred to the same aspects before and after the therapy, for example referring to emotional reasons for practicing CAM and detailing the emotional dimensions of satisfaction after the treatment. However, 25 patients mentioned slightly different attitudes. Almost half of them (n = 11) expressed physical and/or external reasons for practicing CAM (5 mentioned external reasons only and 2 mentioned physical reasons only), and referred to emotional reasons after the therapy. In addition, 4 patients referred to external reasons before the therapy and mentioned encounter-related aspects after the therapy, mainly the therapist's human and personal attitude. The comparison did not reveal any change in the opposite direction, namely from emotional aspects to external and/or physical ones.
Of the patients who did not complete the CAM sessions (n = 28), 11 patients mentioned external reasons for practicing it, mostly a recommendation from a nurse. Four patients had prior experience with CAM and three decided to try out of curiosity.
Discussion
The aim of the current study was to qualitatively investigate the attitudes of patients with cancer regarding CAM by examining their prior expectations as well as the perceived contribution after the treatment.
The study found that patients referred to emotional aspects as reasons to practice CAM, for example the need to reduce stress levels or gain inner strength. This finding is supported by previous studies, which demonstrated the significant emotional needs and difficulties of patients with cancer.30,31 In addition, the comparison between pretreatment and posttreatment contents suggested that the CAM therapy encouraged patients to express emotional aspects of their coping, which were not detailed in their prior expectations. Given the importance and prevalence of these aspects among patients with cancer, it is positive to refer to these issues and enable emotional disclosure as part of the therapeutic session.
The physical aspects expressed by the patients are highly common and familiar, given the significant physical implications of coping with cancer and its treatment. 32 However, the current findings suggest an additional value of the CAM therapy to the physical aspects of coping, a more active and self-sufficient position, as expressed by the patients' awareness and increased activity. Adopting this type of attitude may have important implications on the patient's coping, including emotional benefits, such as an increased sense of capability and inner strength.
An important aspect, which did not appear in patients' prior expectations, is the therapeutic encounter, mainly the therapist's considerate and personal attitudes. Patients were highly satisfied with this aspect, even though they did not detail any need for emotional bond or supportive relations before the therapy. This may suggest that the CAM encounter encouraged patients to express their relational and supportive needs. These needs may be highly significant, given previous findings regarding the profound implications of coping with cancer on patient's relationships. Marital relations can be impaired due to increased distress, changes in responsibilities, and communication difficulties,33,34 along with impairment in social relationships.34,35 The supportive role was traditionally fulfilled by nurses; however, in the current health care system, the nurse's workload makes it difficult for them to refer to the relational aspects of their interactions with patients, but rather to practical and directive ones.36,37 Previous studies have demonstrated that this function is also fulfilled by the practice of spiritual care, which addressed patients' needs for an attentive and caring attitude, 38 as well as support and comfort. 39
Most of the patients who did not complete the six sessions referred to CAM, due to external reasons, mainly a nurse's recommendation. This finding may further strengthen the assumption, which was discussed in the Introduction, that inner and personal reasons are important motives to practicing CAM and to benefit from the therapeutic encounter. Given the limited resources in the health care system, it might be more efficient to conduct a short intake with patients before referring them to palliative services, in order to evaluate their motivation for treatment, personal needs and resources. This may help tailor the appropriate intervention for them (e.g., CAM, spiritual care, psychological services), and may improve treatment efficacy, as part of the personalized care trend.
Our findings should be evaluated in light of the limitations of the study. First, the current study was carried out as a qualitative study with only two written open-ended questionnaires, rather than semi-constructed interviews that could have enabled a conversation and a deeper understanding of patients' perspectives and attitudes. It included a sample of patients with cancer from a single medical center in Israel, not chosen randomly. It evaluated only the short-term effects of a single CAM therapy for each patient. In addition, it evaluated patients who practiced various modalities of CAM, with no consideration given to possible differences between them (e.g., therapeutic attitude, caregivers). In addition, most of the patients practiced shiatzu and music therapy, thus creating a possible bias.
Conclusion
The expectations of patients with cancer regarding CAM therapies included common and central emotional and physical aspects. It seems that the therapeutic encounter evoked emotional and relational aspects, as well as a more active position, which may have significant implications on patients' coping abilities. Encouraging personal motives for CAM may increase treatment efficacy and ensure the optimal use of limited health care resources.
Footnotes
Author Disclosure Statement
No competing financial interests exist.