
Abstract
Abstract
Background:
Emergency departments (EDs) are seeing more patients with palliative care (PC) needs, but evidence on best practice is scarce.
Objectives:
To examine the effectiveness of ED-based PC interventions on hospital admissions (primary outcome), length of stay (LOS), symptoms, quality of life, use of other health care services, and PC referrals for adults with advanced disease.
Methods:
We searched five databases until August 2014, checked reference lists/conference abstracts, and contacted experts. Eligible studies were controlled trials, pre-post studies, cohort studies, and case series reporting outcomes of ED-based PC.
Results:
Five studies with 4374 participants were included: three case series and two cohort studies. Interventions included a screening tool, traditional ED-PC, and integrated ED-PC. Two studies reported on hospital admissions: in one study there was no statistically significant difference in 90-day readmission rates between patients who initiated integrated PC at the ED (11/50 patients, 22%) compared to those who initiated PC after hospital admission (179/1385, 13%); another study showed a high admission rate (90%) in 14 months following ED-PC, but without comparison. One study showed an LOS reduction (mean 4.32 days in ED-initiated PC group versus 8.29 days in postadmission-initiated group; p < 0.01). There was scarce evidence on other outcomes except for conflicting findings on survival: in one study, ED-PC patients were more likely to experience an interval between ED presentation and death >9 hours (OR 2.75, 95% CI 2.21–3.41); another study showed increased mortality risk in the intervention group; and a case series described a higher in-hospital death rate when PC was ED-initiated (62%), compared to ward (16%) or ICU (50%) (unknown p-value).
Conclusions:
There is yet no evidence that ED-based PC affects patient outcomes except for indication from one study of no association with 90-day hospital readmission but a possible reduction in LOS if integrated PC is introduced early at ED rather than after hospital admission. There is an urgent need for trials to confirm these findings alongside other potential benefits and survival effects.
Introduction
S
Emergency departments (EDs) are highly vulnerable to this demographic transition. They are not only seen as an available option to seek relief from pain and other burdensome symptoms, 5 but as an accessible entry point to a high-technology health care system. 2 While not originally considered an ideal environment to deliver PC, EDs face the challenge of receiving growing numbers of patients at the EOL. 2 Many patients with serious and life-threatening illness present to EDs, because symptoms cannot be controlled in the community setting.2,5,6 Emergency medicine (EM) providers may have limited training and resources to manage and respond well to patients in the ED who have PC needs, nor to fully respect these patients' preferences and expectations.7–10 There is scarce evidence about how ED services can best manage patients that are both clinically and socially complex, promoting continuity of care and preventing unnecessary admissions. 2
Interest in the interface between EM and PC is recent but has been growing—supported by preliminary data 11 that suggest these interventions might help to identify PC needs and reduce acute hospital admissions by promoting admission to a PC unit instead, reduce length of stay (LOS), and reduce costs. 5 Reducing hospital admissions is key to ensure that patients stay for as long as possible at home in their last months of life. There is extensive evidence showing that this preference is shared by the majority of patients with advanced illness. 12 Therefore, in this systematic review we aim to examine and compare the effectiveness of ED-based PC interventions on hospital admissions (primary outcome), LOS, symptoms, quality of life (QoL), use of other health care services, and PC referrals for adults with advanced disease.
Methods
The review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement 13 and followed a predesigned protocol.
Identification of studies
Search strategy
We searched five databases (MEDLINE, EMBASE, CENTRAL, PsycINFO, and NHSEED) up to August 2014 using search terms “Palliative” and “Emergency” or their equivalents combined with the operator AND. In addition, we hand searched recent issues of relevant journals that were not fully indexed in databases, screened the references of relevant reviews and all included studies, screened proceedings of conferences in the field, and contacted 29 experts to identify further eligible studies.
Study selection
Studies were first screened by one reviewer (DS) who read titles and abstracts and then by two reviewers (DS and CN) who independently read the full text. Studies were included if they provided original data evaluating any type of PC intervention or service at the ED for adult patients (18 years or older) with advanced disease. This was aligned with Beynon et al.'s broad criteria for PC needs in an ED setting: 14 diagnosis of cancer, or chronic obstructive pulmonary disease (COPD), or heart failure (HF), or renal failure, or liver failure, or neurological disease (multiple sclerosis, Parkinson's, dementia, or motor neuron disease), or >2 comorbidities on the Charlson Index.
We included interventional controlled studies (experimental and quasi-experimental studies), pre-post studies, cohort studies, and case series. We considered any type of PC intervention that was described as such by the authors and that was provided at the ED, with the requirement of being provided by at least one member of a PC team (e.g., social worker, nurse, or physician). Studies not written in English, Spanish, Portuguese, French, or Italian were excluded due to translation limits. Studies were also excluded if full publications were not available.
Data extraction
A data extraction form was developed specifically for the review. This included items recording study identification, methods, participants, intervention, outcome measurement, and results.
Quality assessment
Studies were independently assessed for methodological quality by two reviewers (DS and CN), using tools according to the study design. Three of the included studies were case series, for which we used the National Institute for Health and Care Excellence (NICE) quality assessment tool for case series. 15 Two studies were cohort studies; for these, we used the Scottish Intercollegiate Guidelines Network (SIGN) checklist for cohort studies. 16
Analysis
The characteristics and results of the studies were narratively reported in synthesis tables. For the primary outcome (hospital admissions), we have reported quantitative data when available from the papers or through the authors. For secondary outcomes (LOS, symptoms, QoL, use of other health care services, PC referrals), we reported the results according to the measure used. A meta-analysis was not performed due to limited results.
Results
Search results
Electronic searches identified 5301 hits, resulting in 4015 references after duplicate removal. Through screening of title and abstract, 3986 references were excluded. We then examined the full text of the 29 remaining references. Five studies were included. Reasons for exclusion are presented in Figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart.
Design and setting
Three studies are case series and two are cohort studies with intervention and control groups (see Table 1). Four studies originated from the United States (conducted between 2005 and 2010), all from major academic inner city tertiary medical centers. One study was European, including 174 EDs across France and Belgium, conducted in 2004 and 2005. 17
ED, emergency department; HQoL, health quality of life; LOS, length of stay; NICE, National Institute for Health and Care Excellence; MVQoL, Missoula Vitas Quality of Life; NP, nurse practitioner; OR, odds ratio; PC, palliative care; QOL, quality of life; SE, standard error; SIGN, Scottish Intercollegiate Guidelines Network; SOB, shortness of breath.
Participants
In total, 4374 participants were included, with a mean of 875 participants per study (ranging from 89 to 2420 participants). Four studies included patients with cancer—16.5% 17 to 51% 18 —and noncancer conditions—44.6% 19 to 83.5%. 17 The latter predominantly included advanced dementia, HF, COPD, 18 renal and liver diseases.19–21 Median/mean age ranged from 66 to 90 years. Gender distribution ranged from 36% 21 to 58% 22 for males and 42% 22 to 64% 21 for females.
Types of interventions
We found three main types of ED-based PC interventions, described according to the level of cooperation between ED and PC services:
• ED screening tool used by PC members: Glajchen et al.;
19
this is a rapid two-stage screening protocol (BriefPal) that was developed to improve referral of frail older people in ED to PC or hospice care • Traditional PC consultations in the ED: Van Tricht et al.,
20
Mahony et al.,
21
and Lamba et al.
22
In these interventions, there is typically no specific collaborative relationship to help integrate PC principles into the fabric of ED care
23
• Integrated ED PC services: Wu et al.;
18
these programs are characterized by a more formal working relationship between the ED and PC program to define partnership goals and objectives
23
Results from quality assessment are discussed below and are shown in Figure 2 with dots to aid interpretation.
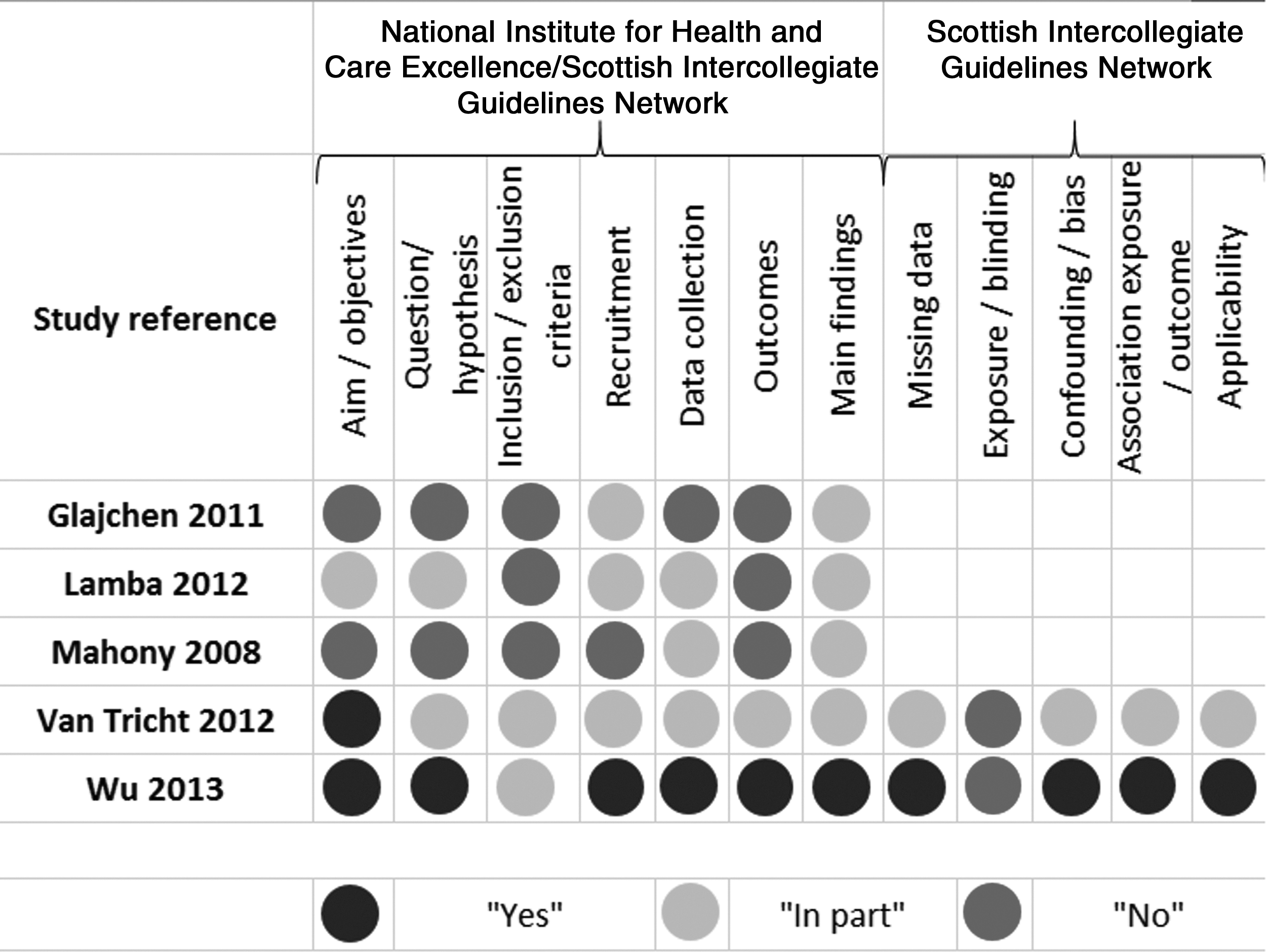
Quality assessment of the included studies.
Case series
Using the NICE quality assessment tool for case series, 13 the quality of the three case series was considered moderate (see Fig. 2). All case series were single-center and the data were collected retrospectively. Other methodological weaknesses were related to lack of clarity of the hypothesis, aim, and objectives,17,18 inclusion/exclusion criteria, 19 data collection, 18 and outcomes measured.17–19
Cohort studies
Using the SIGN methodology checklist for cohort studies, 14 the quality of the study by Van Tricht et al. 20 was considered low (0) while the quality of the study by Wu et al. 21 was considered acceptable (+). The two studies reported clear aims, and the intervention and control groups were selected from similar and comparable source populations. However, Van Tricht et al. 20 do not clearly state their hypothesis, there is a lack of information on missing data, and the outcomes are not clearly stated. Methodological strengths of the study by Wu et al. 21 include having a clear aim and hypothesis; and information on missing data, outcomes, limitations, and results. However, since both studies are retrospective cohort studies and the outcome assessment was not blinded to the exposure status (ED-based PC consultation or standard care), according to SIGN the rating of these two studies cannot be rated higher than “+” (acceptable quality). 14 Effects of the interventions are discussed below and summarized in Table 2.
APRDRG, All Patient Refined Diagnostic Related Group; ED, emergency department; IQR, interquartile range; LOS, length of stay; MMC, Montefiore Medical Centre; MVQoLI, Missoula Vitas Quality of Life Index; OR, odds ratio; PC, palliative care; QoL, quality of life; ROM, risk of mortality; SD, standard deviation; SE, standard error; SOI, severity of illness.
Hospital admissions
In two studies the authors reported information on hospital admissions (1726 patients). Wu et al. 18 found no statistically significant differences in 90-day readmission rates. The authors stated that 11/50 patients (22.0%) that initiated PC at the ED (integrated ED PC) were readmitted, compared to 179/1385 (12.9%) of those that initiated PC after hospital admission. Mahony et al. 21 reported on hospital admissions but without comparison with a control group: 90% of the 291 patients that were seen by the ED-based PC team (traditional PC consultations) were admitted to the medical center during the 14-month timeframe of the study.
Length of stay
In two studies the authors reported information on LOS (1524 patients). Wu et al. 18 reported the mean LOS for the intervention group (patients who received ED-based PC; n = 50) was 4.32 days (SE 0.68) compared to 8.29 days (SE 0.36) in the control group (without ED-based PC; n = 1385). In multivariate analysis (controlling for covariates and propensity scores), the initiation of PC at the ED (versus after hospital admission) was still associated with shorter LOS, with a mean decrease of 3.63 days (p < 0.01). Lamba et al. 22 described the “average” hospital LOS of patients for whom an ED-based PC consultation was initiated was two days (without comparison with a control group).
Symptoms
In one study the authors reported information on symptoms (Glajchen et al. 19 ). Patients in the intervention group (patients screened by BriefPal) reported symptom reduction in pain, shortness of breath, nausea, and anxiety. These outcomes were assessed through follow-up of 112 patients via telephone contact. However, no information was given about time points; and no information was given about descriptive or analytic statistics comparing patients who were screened to those who were not.
Quality of life
In one study the authors reported information on QoL (Mahony et al. 24 ). The patient's QoL was self-reported using the Missoula Vitas Quality of Life Index (MVQoLI; scores range from −20 to +20; higher scores mean higher QoL). This assessment was done post-ED discharge, although no information was given on the specific point in time after the discharge. By then, very few patients completed the MVQoLI (20/291, 6.9% response rate). The authors reported that of those 20 patients, 14 expressed satisfaction with the control of their physical symptoms, and 13 expressed improved ability to communicate with people close to them. There was no information on total scores, results comparison pre-post the intervention (consultations by two PC nurse practitioners), or with a control group.
Use of other health care services
Two studies reported information on the use of other health care services. Lamba et al. 22 reported subsequent use of ED by patients who received ED-based PC, but without a comparison group. Twenty-four percent of patients (21/89) returned within one month and 59% (52/89) within six months of their initial contact with PC nurse practitioners. Four out of the 34 patients that received the ED-based PC and survived were discharged to skilled nursing facilities. Other destinations on discharge were home (18/34), home hospice (11/34), and unknown place (1/34). Mahony et al. 21 reported that of the 291 patients who received the ED-based PC service, 45% visited the ED in the 12 months subsequent to the index visit (compared to 59% in the 12 months before the index visit). Of those admitted to acute care (90.0%, n = 262), 41.9% were discharged to skilled nursing facilities, 24.2% to home with homecare, and 19.1% were discharged without homecare.
Referral to palliative care or hospice care services
In two studies the authors examined referrals to other PC or hospice care services, but neither provided analytical results. Glajchen et al. 19 reported that at the peak of implementation, the BriefPal screening project accounted for half of all referrals to the in-hospital PC service. Lamba et al. 22 described that 12% of patients who initiated PC at ED were discharged to home hospice (compared to 4% in ICU and 13% in ward-initiated PC). The statistical significance of these differences was not reported.
Survival
There were conflicting results on survival. Van Tricht et al. 20 reported that the provision of traditional ED-based PC was associated with greater odds of experiencing an interval between ED admission and death longer than nine hours (adjusted OR 2.75, 95% CI 2.21 to 3.41). Wu 201318 reported the risk of mortality for 1435 patients according to the All Patient Refined Diagnostic Related Group (APRDRG) risk of mortality (ROM) and severity of illness (SOI). 25 The APRDRG is a severity coding methodology that allows assignment of an SOI and ROM score in four categories (minor, moderate, major, and extreme risk). This system is used to evaluate resource utilization and predict inpatient mortality. The authors reported statistically significant differences between the intervention and control groups (p < 0.01). In the latter (standard care; n = 1385), the ROM was 2.3% for minor risk (32/1385), 22.5% for moderate risk (311/1385), 42.4% for major risk (587/1385), and 32.9% for extreme risk (455/1385). In the intervention group (n = 50), the ROM was 4.0% for minor risk (2/50), 24.0% for moderate risk (12/50), 62.0% for major risk (31/50), and 10.0% for extreme risk (5/50). The direction of these differences suggests higher mortality in the intervention group. Finally, Lamba et al. 22 reported in-hospital death rates. In the ED-initiated PC group (n = 89), the in-hospital death rate was 62% (n = 55), compared to 16% in the ward-initiated PC group (91/583) and 50% in the ICU-initiated PC group (288/578). However, the authors did not report the statistical significance of these differences. They viewed the in-hospital death rate in the ED-initiated PC group as “very high,” justified due to most patients dying early and at the ED, “signifying a trend for ED clinicians to request PC consults in those who are imminently dying.” 22
Discussion
We found no evidence that ED-based PC affects patient outcomes except for indication from one study of no association with 90-day hospital readmission but a possible reduction in LOS (by 3.53 days) if integrated PC is introduced early at the ED rather than after hospital admission. These findings must be interpreted with care, as they derive from a retrospective cohort study with a small intervention group (n = 50). However, if confirmed in future studies, this could suggest that ED-based PC may not avoid hospital readmission (possibly inevitable due to the complexity of patients with PC needs who present at the ED) but may help to plan and provide a faster discharge. It is important to discuss what a reduction in hospital LOS means at the EOL. Extensive evidence shows that well over 50% of people prefer to be cared for and to die at home.12,26 Most patients and caregivers facing advanced illness also prefer this.12,27,28 Therefore, if the result holds true in future trials, an early initiation of PC at the ED might contribute to decrease trends towards hospitalized dying, by helping patients who wish to remain at home spend less time in hospital and go home quicker.
Interestingly, we found conflicting findings about the association of ED-based PC interventions with patient's survival. Lamba et al. reported different in-hospital death rates, depending on where PC interventions commenced; and although the statistical significance of these differences was not reported and the ED-PC group was relatively small (n = 89), the findings indicated there could be more (in-hospital) death in this group (62%) compared to patients who initiated PC at a ward (16%). The difference is not so large when compared to patients who initiated PC at the ICU (50%), which suggests that the high rates may reflect the acute state of patients at the ED and ICU, which makes PC interventions more time restricted and closer to death.
On the contrary, Wu et al. found a lower proportion of people in extreme mortality risk in the group who initiated PC at the ED (10.0%) compared to those who initiated after admission (32.9%). But the overall direction of differences taking into account the other categories (major, moderate, and minor risk) indicates higher mortality risk in the intervention group—the main difference being in a major risk group, which represents 62.0% of all intervention patients and 42.4% of controls. Contrarily, Van Tricht et al. reported that ED-based PC was associated with two times greater odds of an interval between ED admission and death longer than nine hours. The latter results suggest that ED-based PC interventions might prolong survival, similar to what has been found in other recent interventional studies of PC.29,30
Limitations
Only one review author (DS) conducted the initial screening. Only 27 potentially eligible studies were found through hand searches. The studies included were all conducted in high-income countries. Only one example of ED screening tools used by PC members 31 and only one example of integrated ED PC services 18 were found.
Since we conducted the review searches (August 2014), a systematic review of PC screening/referral projects at the ED was published. 32 This did not exclude studies that used non-PC personnel to screen patients. From the seven studies identified, one is relevant to our review but does not change our findings. This was a randomized control trial with 134 patients, comparing early ED-based PC referral to usual care (where PC was provided only if requested by the admitting physician). 33 The authors found that early referral increased the likelihood of receiving a PC consultation, which was low as part of usual care within the ED (18% in the usual care group). Finally, the body of evidence we reviewed has strong methodological limitations, mainly related to the retrospective nature of studies.
Conclusions
In this systematic review we found that there is yet insufficient evidence of the effect of ED-based PC interventions, except for indication from one study of no association with 90-day hospital readmission but a possible reduction in LOS if integrated PC is introduced early at the ED rather than after hospital admission. Evidence is very scarce of impact on symptom control, QoL, and referrals to specialist PC services and use of other health care services. Finally, we found conflicting data on survival that require investigation. There is an urgent need for powered and well-conducted randomized controlled trials to examine any potential benefits of these interventions.
Footnotes
Acknowledgments
This study would not have been possible without the important contribution of the Calouste Gulbenkian Foundation, Dr. Jacinta Fernandes and the Unidade Domiciliária de Cuidados Paliativos—Planalto Mirandês, who generously funded and supported it. The study was conducted as Duarte Soares' research project for the MSc in Palliative Care at King's College London, integrated in the DINAMO Project, which aims at enhancing advanced training and research to optimize home palliative care in Portugal (Principal Investigator – Barbara Gomes, Scientific Director – Irene J. Higginson, other members – Pedro L. Ferreira, Hélder Aguiar, Ana F. Lacerda, Vera P. Sarmento, Duarte Soares, Rita Canário, Maja de Brito, Catarina Ribeiro, Diogo M. Branco).
The authors also wish to thank the library services from King's College London; the authors of the included studies, who provided the information asked for; colleagues in the Cicely Saunders Institute and the MSc course, mainly Rita Canário, Vera Sarmento, Ana Lacerda, and Bárbara Antunes, for supporting this project since its inception.
Author Disclosure Statement
No competing financial interests exist.