
Abstract
Abstract
Background:
Early conversations between clinicians and patients about goals of care may improve patients’ quality of life and prevent nonbeneficial care near the end of life, but these conversations are limited in frequency and scope. To address this issue, clinicians are increasingly asked to use standardized medical order forms, like the Medical Orders for Life-Sustaining Treatment (MOLST), to document end-of-life conversations and to help ensure that patients’ wishes are realized. In kind, the Centers for Medicare and Medicaid Services recently decided to reimburse physicians as well as nurse practitioners and physician assistants for these conversations.
Objective:
To explore physicians’ and advanced practitioners’ (APs’) attitudes and behaviors around initiating and documenting goals of care conversations and to identify targets for improvement.
Design:
Online survey administered between October 1, 2014 and February 20, 2015.
Setting/Subjects:
Physicians (n = 2492) and APs (n = 336) at an urban academic medical center.
Measurements:
Clinicians’ perceptions and self-reported behaviors regarding goals of care conversations and the Massachusetts MOLST form.
Results:
We found that 44.0% of physicians and 33.0% of APs reported that they discussed goals of care with all patients with serious, life-limiting illness (p < 0.001). APs were more likely than physicians to report awareness of MOLST forms (55.1% vs. 45.1%, p < 0.001) but less likely to feel comfortable making recommendations on end-of-life care (25.3% vs. 41.0% recommending against resuscitation, p < 0.001; 35.1% vs. 55.7% recommending for resuscitation, p < 0.001).
Conclusions:
These findings suggest the need to educate physicians and empower APs to facilitate goals of care conversations and use standardized forms, as well as an opportunity for interdisciplinary collaboration.
Introduction
E
Although a small survey in heart failure clinicians suggested that physicians are more likely than nurse practitioners and physician assistants to discuss goals of care, 7 little is known about how different types of clinicians generally approach these conversations. Therefore, we assessed self-reported practices and perceptions of physicians and advanced practitioners (APs, including nurse practitioners, physician assistants, certified registered nurse anesthetists, and nurse midwives) regarding goals of care conversations and the Massachusetts MOLST forms to understand any differences between these groups and to identify potential targets for intervention.
Methods
We created a nine-item survey instrument to assess how and how often clinicians engage in end-of-life conversations; comfort level with making recommendations regarding resuscitation; and use and perception of the MOLST form. We administered the web-based instrument as the first part of a mandatory training module on the MOLST form to all clinical affiliates at Massachusetts General Hospital, comprising 336 APs and 2492 physicians (including 622 trainees and 43 psychologists with clinical PhDs), between October 1, 2014 and February 20, 2015.
Since the survey was anonymous, aggregated demographic data were gathered separately for all Massachusetts General Hospital Physicians (n = 2566) and APs (n = 311), which led to some discrepancies in total counts. We used the chi-square test to compare groups. 8 Two-tailed p < 0.05 indicated statistical significance. The study was exempt from institutional board review based on 45CFR46.102.
Results
All physicians (n = 2492) and APs (n = 336) eligible for the survey responded (Table 1). Forty-four percent of physicians and 33.0% of APs reported they discussed goals of care with all patients with serious, life-limiting illness (p < 0.001). Fifty-one percent (50.6%) of physicians and 32.1% of APs reported that they offered prognostic information “all of the time” to patients/families who wanted to hear it (p < 0.001). Physicians and APs were more likely to feel comfortable recommending resuscitation if they felt resuscitation would be helpful to the patient (55.7% of physicians and 35.1% of APs strongly agreed; p < 0.001) than recommending against it if they felt it would not be (41.0% of physicians and 25.3% of APs strongly agreed; p < 0.001; among physicians: p < 0.001, among APs: p = 0.006; Fig. 1). Forty-five percent (45.1%) of physicians and 55.1% of APs reported that they were aware of the MOLST form (p < 0.001); 22.9% of physicians and 24.7% of APs reported that they or their team filled out such a form at least once in the previous 12 months (p = 0.46).
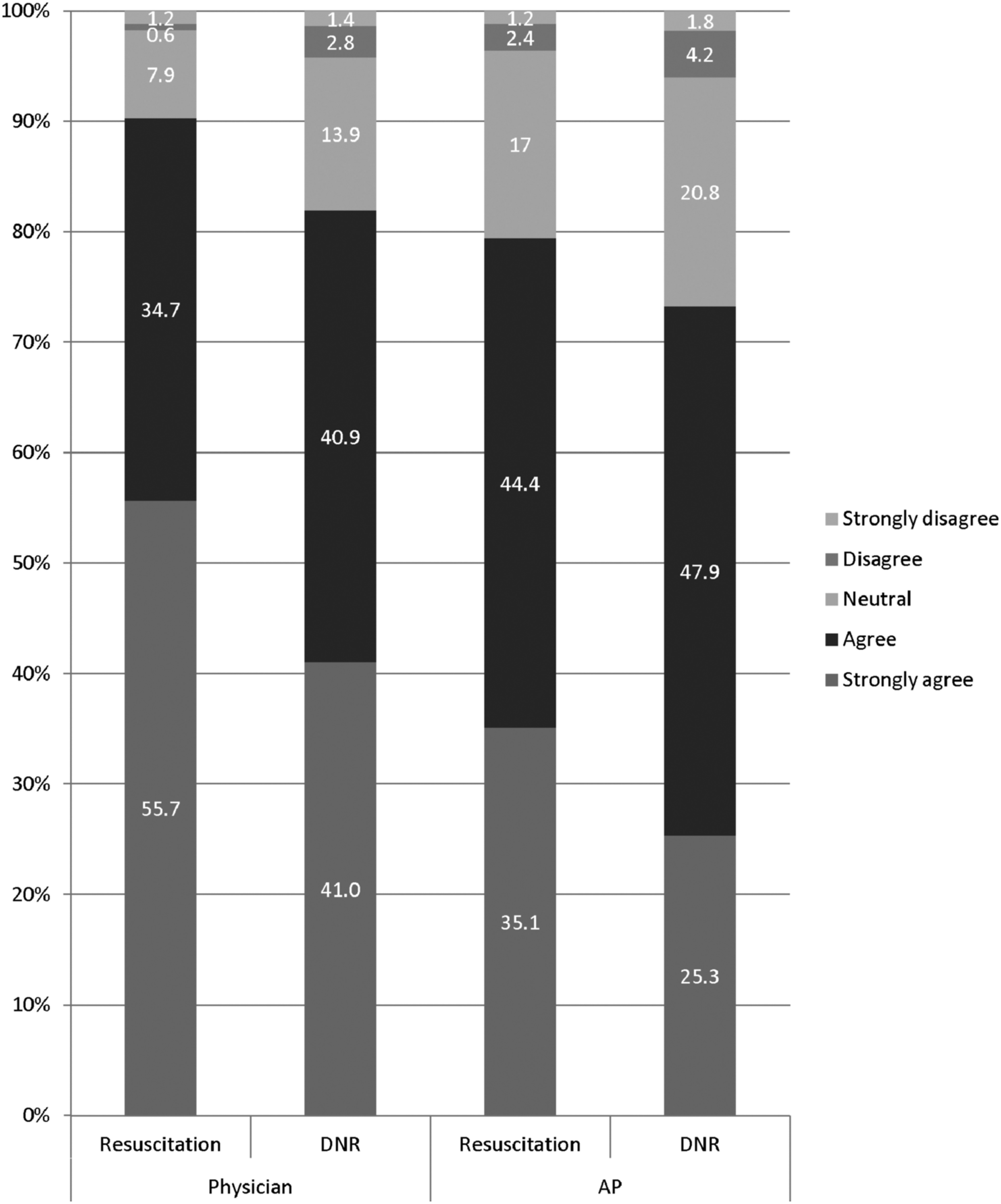
This graph shows the percentage of physicians and APs who reported various levels of comfort with recommending resuscitation when they felt it was most appropriate or recommending against resuscitation when they felt that this was the most appropriate. APs, advanced practitioners; DNR, do-not-resuscitate order.
Averaged among 2478 subjects with available data.
Averaged among 259 subjects with available data.
Sex was missing for one subject in each group.
The most commonly reported barriers to using the form among physicians and APs included nonapplicability to their patients (55.3% and 50.0% respectively), lack of awareness (25.4% and 25.9%), lack of time (13.0% and 6.0%), and patient/family unwillingness to discuss the topic (12.6% and 16.7%). APs also reported that it was challenging for them to raise the issue (9.2%).
Discussion
Although encouraging overall, our findings show some room for improvement in how often clinicians discuss prognosis and goals of care. More respondents felt comfortable conveying their recommendation when they felt resuscitation would be helpful than when they felt it would not—a finding that supports reports of clinicians’ discomfort with confronting the limits of medical intervention. These findings align with the recently published Institute of Medicine report “Dying in America,” which noted the importance as well as the inconsistent use of high-quality clinician–patient conversations about end-of-life care. 1
Although there was general lack of awareness about MOLST forms, APs were more likely to be aware of the MOLST forms than physicians but less likely to be comfortable recommending for or against resuscitation. The difference in MOLST form awareness may reflect increasing administrative burden on physicians and resulting challenges in teaching them about new initiatives, as well as efforts to displace some of this burden through task sharing by APs. To educate both APs and physicians about the presence and utility of standardized forms, clinicians might designate MOLST champions at clinical sites and use educational forums such as ongoing web-based modules and “in-services” across hospital and outpatient facilities. These forums would offer opportunities to discuss the importance of advance care planning and goals of care conversations more generally and to link education about the forms to education about best practices in having these discussions. Making forms more accessible at point of care would supplement training and help to address structural barriers to their use.
The difference in comfort level with making recommendations on resuscitation status, in turn, may reflect that APs might defer (appropriately or not) to physician colleagues to have these high-stakes discussions. Our results also point to the need to empower APs to facilitate goals of care conversations when appropriate, perhaps through formally assigned roles or training. MDs and APs may need to clarify roles and discuss who should take the lead on goals of care conversations when collaborating in patient care. Our results also point to an opportunity for an interdisciplinary approach, in which some team members might focus on leading end-of-life conversations, whereas others ensure that they are documented.1,4
Our study should be interpreted in the context of its limitations. The study was conducted at a single site with a cross-sectional design and it relies on self-report of clinician behavior that may not accurately represent true behavior. The study does not allow insight into which physicians or APs (e.g., inpatient versus outpatient and from which specialties) are having these conversations, nor does it shed light on the quality of discussions. However, we did obtain responses from 100% of a large population representing a spectrum of clinicians involved in advance care planning. Further research is needed on the impact of educational initiatives on MOLST usage and to determine whether the culture around advance care planning is evolving to better serve the needs of patients and families.
Footnotes
Acknowledgments
I.G. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. There was no financial or material support for the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the article.
Author Disclosure Statement
No competing financial interests exist.