
Abstract
Abstract
Background:
Honoring the wishes of cancer patients is a responsibility of oncologists; however, end-of-life care (EOLC) discussions are frequently delayed past the point of usefulness.
Objective:
To develop a patient-reported outcome (PRO) screening tool that facilitates timing of EOLC discussions.
Design:
A seven-item PRO instrument covering four clinical and personhood domains [performance status, pain, burden (financial and family), and depression] was administered to patients with advanced malignancies undergoing noncurative therapy. The PRO instrument included the patient's assessment of the importance of each domain. Results were correlated with the oncologist's assessment of appropriateness of continuing aggressive therapy.
Setting/Subjects:
Four hundred thirty-three patients fully completed the PRO instrument between February and March 2015 at a single outpatient cancer center.
Results:
There was a difference (p < 0.0001) in median scores among cohorts deemed by their oncologists appropriate to continue noncurative treatments versus patients whose physicians were contemplating or actively engaged in EOLC discussions. The scores for the four individual domains also differed among cohorts. An upper threshold score comprising 46% of patients deemed appropriate to curtail treatment (but inclusive of only 26% of patients deemed appropriate to continue) was determined, facilitating identification of patients for EOLC discussions.
Conclusions:
A seven-item patient-centric PRO instrument was able to separate advanced malignancy patients into cohorts who their physicians deemed were at differing stages in their cancer journey with increasing needs for advance care planning. A study to determine if the threshold scores identified in this pilot correlate with palliative/EOL consultation frequency and patient survival is underway.
Introduction
C
Prior attempts to encourage advance care planning among cancer patients have focused on improving the accuracy of identifying patients at risk of imminent death. Cancer patients with poor performance status, weight loss, anorexia, breathlessness, confusion, and abnormalities on laboratory parameters have limited survival. 11 The PaP score, which aggregates these features, when combined with oncologist's estimates of survival, has been found to categorize patients into groups with differing survivals. 12 There are also decision aids that have been developed to assist patients facing health treatment choices, several of which account for personal preferences and values; however, few address the need to make EOLC decisions. 13 The recently developed Criteria for Screening and Triaging to Appropriate aLternative care (CriSTAL) tool utilizes objective criteria, including age, frailty, comorbidities, nursing home/hospitalization utilization, and laboratory criteria to identify patients likely to die within three months but does not account for patient input. 14
A patient-reported outcome (PRO) screening tool that uses patient input to trigger advance care planning discussions would be beneficial as a clinical decision tool. Patients may have difficulty starting the conversation but may be able to describe physical and emotional symptoms. A PRO screening tool that does not mention EOLC but rather focuses on domains of burden and suffering might correlate with appropriateness to reassess EOLC decisions. The screening tool needs to be patient centric, allowing the patient to express his or her assessment of the importance of each domain. Combining the patient-reported physical and emotional symptoms with an individual's weighting of importance of the domains generates a global score. The hypothesis is that a patient with higher intensity, multidomain burdens might be willing to engage in advance care planning. As an initial step in developing a clinical decision tool, we sought to correlate scores from a new patient-centric instrument with their physician's assessment of appropriateness to continue aggressive therapy. The goal of this pilot is to establish “threshold scores” in which physician assessment of the value of continuing therapy is linked to patient self-reported distress. These threshold scores can subsequently be utilized to encourage physicians to initiate more timely palliative care consultations and/or EOLC discussion.
Methods
PRO instrument
A seven-item PRO study instrument, known as “Living with Cancer” (LWC), was developed in February 2015 by Cancer Outcomes Tracking and Analysis (COTA, Inc.; Fig. 1). The instrument covers the following four personhood and clinical domains: (1) physical performance status,15–18 (2) pain, 19 (3) burden (financial and family),19,20 and (4) depression.21–23 A second, but critical, element of the instrument is to determine a weighting based on the patient's perception of the importance of the item. Each question was given a weighting of 1, 2, or 4 depending if the patient considered the question “not at all,” “moderately,” or “significantly” important.
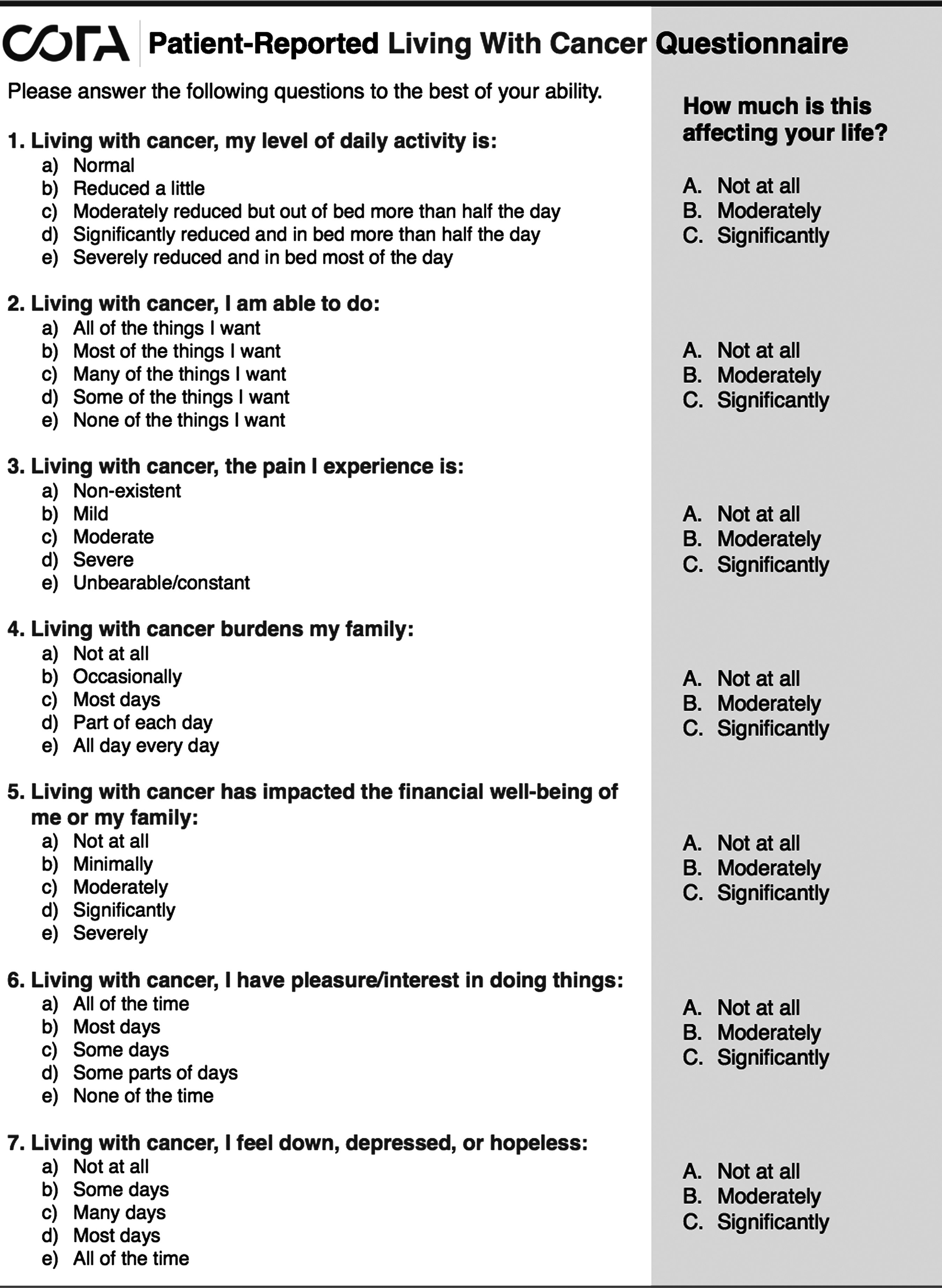
Patient-reported living with cancer questionnaire.
During the instrument development phase, the seven-item PRO was administered to a random subset of patients with advanced malignancies in the John Theurer Cancer Center at the Hackensack University Medical Center (Hackensack, NJ) to determine readability (n = 10). Patients were asked to read the form (written at a sixth-grade level) and describe each question to the investigator. A Spanish translation of the form was developed and confirmed with patients by a Spanish-speaking licensed clinical social worker.
Correlation of PRO with physician assessment
All English- and Spanish-speaking patients (age >18 years old) with malignancies presenting for evaluation to the John Theurer Cancer Center from February to March 2015 were given the PRO instrument in the waiting room by the clinic greeter. No additional explanation or instructions were given to the patients. Upon rooming the patient, the cancer diagnosis was recorded on the form by the nursing assistant. No other identifying information was requested from the patient or recorded on the study instrument. The responses were anonymous, and no attempt to correlate with demographics was made.
Independently, the oncologist of each respondent was asked to state whether the therapy was “curative” or “palliative” and rate the patient's current status with regard to appropriateness of continuing therapy as (1) appropriate to continue therapy, (2) contemplating EOLC-focused advance care planning or curtailment of therapy, or (3) actively in EOLC planning discussions or in hospice referral. These responses were documented on the form by the nursing assistant. The oncologists were not aware of the results of the PRO study instrument. Surveys from patients receiving “curative” intent therapy were discarded.
Statistical assessment
Simple statistics, including two-sided chi-square tests, were evaluated. The statistical team also determined that additional weighting of individual questions did not significantly improve separation between the cohorts.
Consent
The study design was reviewed by the Human Institutional Review Board at the Hackensack University Medical Center and deemed to be exempt from the need for informed consent. The information gathered on the PRO instrument is part of routine medical care and required by CMS and ASCO QOPI compliance. The results were collected in an anonymous manner without any protected health information recorded.
Results
Four hundred thirty-three patients with advanced malignancies undergoing noncurative intent therapy at the John Theurer Cancer Center during February to March 2015 submitted completed LWC instruments. Incomplete surveys (missing two or more questions) were not counted (n = 47). Domain items with answers but no patient assignment of weight were arbitrarily weighted times one. Among patients completing the PRO instrument, 306 (71%) were deemed by their oncologists appropriate to continue noncurative therapy. However, the treating physicians felt that 103 (24%) patients were at a stage where discussions regarding EOLC and/or curtailment of therapy should be contemplated. Twenty-four (6%) patients who completed the survey were actively engaged in EOLC discussions. Malignancy types (by patient) included gastrointestinal cancer 92 (21% of patients), myeloma 87 (20%), breast cancer 58 (13%), leukemia 54 (12%), lung cancer 39 (9%), prostate cancer 33 (8%), and other tumor types each less than 5%.
The scores on each of the four domains differed among the EOLC discussion cohorts. The median scores for the performance status domain were 4, 8, and 14 among the three physician-determined EOLC appropriateness cohorts (p < 0.001 continue therapy vs. contemplating/engaged in EOLC discussions). The median scores for the pain domain were 1, 2, and 2 for the cohorts (p = 0.002). The median scores for the burden domain were 6, 9, and 9 for the cohorts (p = 0.011). The median scores for the depression domain were 4, 6, and 6 for the cohorts (p = 0.019).
The LWC total score was able to separate patients with advanced malignancies into cohorts at differing stages of EOLC discussion appropriateness (Fig. 2). The median total LWC score was 14 for the cohort physician deemed appropriate to continue therapy, 23 for the cohort physician deemed contemplating EOLC discussions, and 35 for the cohort physicians deemed actively engaged in EOLC (p = 0.003 continue vs. contemplating/engaged in EOLC discussions). A threshold score of 28 was exceeded by only 26% (78/306) patients in the physician deemed continue therapy cohort versus 46% (58/127) patients of the contemplating/engaged in EOLC discussion cohort (p < 0.0001). A lower bound of 12 was crossed by 27% (84/306) patients in the continue therapy cohort versus only 11% (14/127) patients in the EOLC cohorts (p < 0.0002).
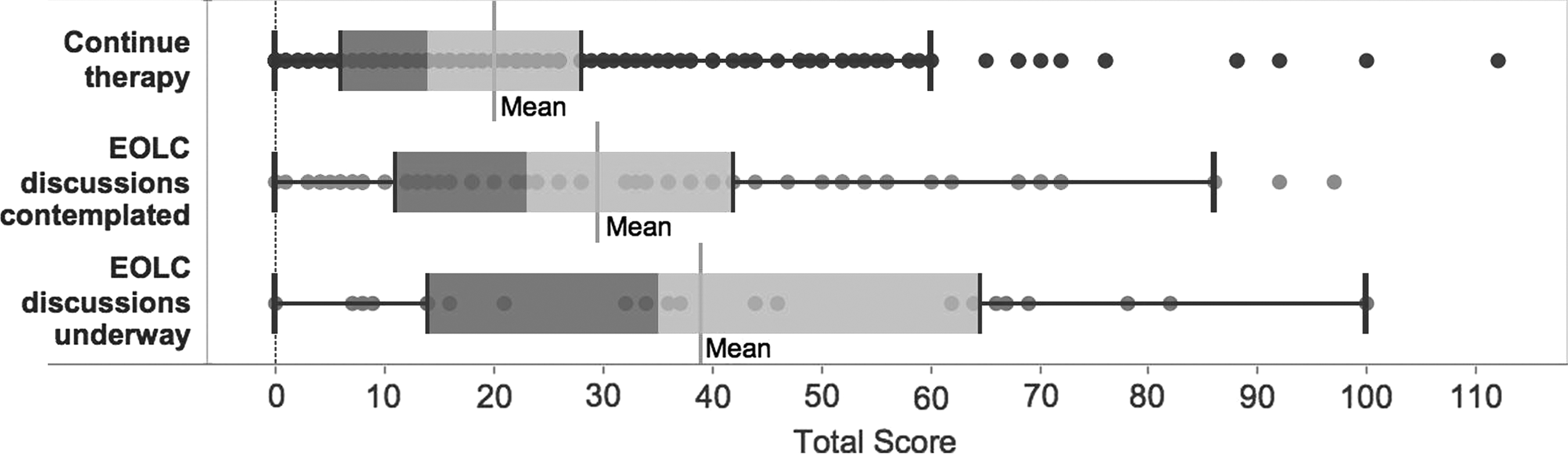
LWC scores by physician deemed EOL discussion appropriateness box–whiskers plot of the LWC total score in 433 advanced malignancy patients. The median total LWC score was 14 for the cohort physician deemed appropriate to continue therapy, 23 for the cohort physician deemed contemplating EOLC discussions, and 35 for the physician deemed actively engaged in EOLC (p = 0.003 continue vs. contemplating/engaged in EOLC discussions). Upper and lower bound scores of 28 and 12 are observed. EOLC, end-of-life care; LWC, living with cancer.
Results of the LWC instrument varied by tumor type. As shown in Figure 3, separation among cohorts was identified among patients with advanced breast and gastrointestinal cancers, but considerable overlap among the myeloma patients was noted.
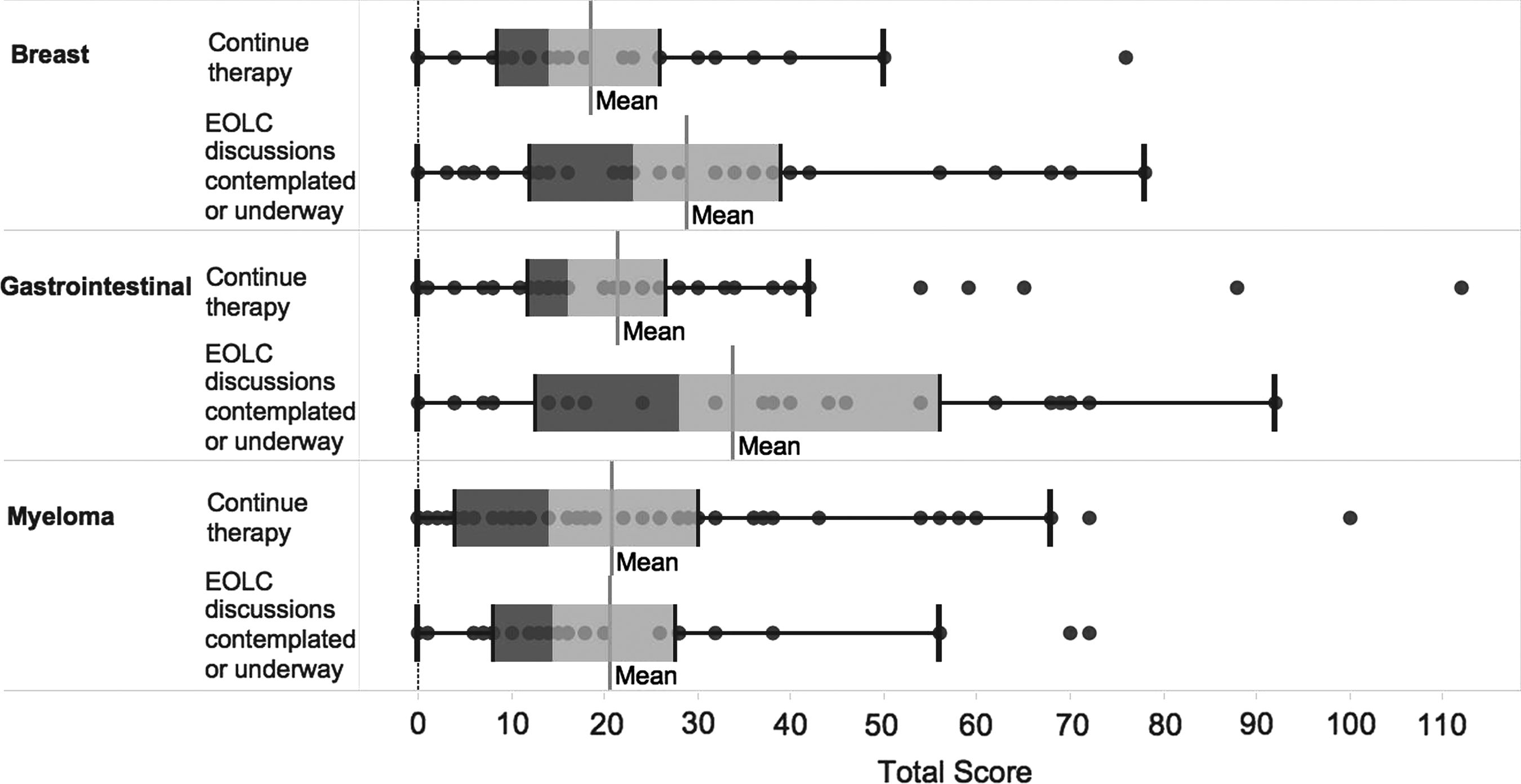
LWC scores by common disease types.
The instrument was reviewed for the existence of patterned relationships and absence of multicollinearity. The correlation matrix of survey responses per patient was analyzed with between-item correlation coefficients noted to be above ±0.30, indicating correlated item scores. The determinant score of the correlation matrix was 0.02, indicating an absence of multicollinearity. Bartlett's test of sphericity confirmed the existence of correlated responses (p < 0.0001). The Kaiser–Meyer–Olkin Measure of Sampling Adequacy was equal to 0.88, supporting the hypothesis that the seven items may measure certain underlying constructs. The results of principal components analysis demonstrated further that all seven items contributed in similar magnitude to driving the variance in scores. Cronbach's alpha coefficient of 0.88 demonstrated that the instrument can reliably measure a single unidimensional latent construct. To improve the statistical power in developing the threshold values, the upper two physician response categories were collapsed, and the upper/lower quartiles were defined as the thresholds.
Conclusions
The seven-item patient-centric “Living with Cancer” PRO screening tool was able to separate advanced malignancy patients into differing physician deemed stages in their cancer journey, with presumed increasing need for advance care planning and EOLC discussions. An upper threshold score was identified, which included almost half of the advanced cancer patients either already engaged in hospice discussions or in whom their physicians were contemplating EOLC discussions. In contrast, only one-quarter of patients deemed appropriate to continue therapy answered the PRO instrument with distress scores exceeding this bound. Knowledge of a patient's score above the upper threshold might prompt an oncologist to consider a palliative care consultation (if there are uncontrolled symptoms) or a hospice consultation. Conversely, a lower bound was identified, which might serve as a basis for postponing end-of-life and/or hospice discussions as these patients are, by their own admission, not under distress. Serial use of the LWC PRO instrument might be illustrative of changes among domains (performance status, pain, burden, and depression) that occur during the cancer treatment journey and may identify patients with particular needs in a single domain (e.g., referral for financial support due to emerging financial toxicity or referral to palliative care for uncontrolled symptoms). A larger study to determine if the threshold scores identified in this pilot correlate with palliative care and/or EOL consultation frequency and survival is underway.
As a potential quality metric, correlation of the LWC scores against the rates of referrals could be utilized to benchmark physician palliative care referral patterns rather than the current system of using days in hospice before death. Multiple reports find that timely EOLC discussions are frequently delayed, yet most oncologists feel that they are not the offenders. The ability to objectively quantify and benchmark physician practice patterns will assume increasing importance in emerging value-based care models.
A guiding principle of the LWC instrument is that patients who are experiencing extreme distress should have the opportunity to discuss advance care planning. A retrospective review of 100 consecutive patients who died from their primary gynecologic malignancies reported that although 49% of patients had a palliative medicine consultation, only 18% had timely consultations (occurring >30 days before death). 24 The use of aggressive medical care and overall cost of care were higher among the patients undergoing no or delayed consultations. 25
The economic impact of EOLC discussions cannot be ignored. A disproportionate share of the costs of healthcare is spent during the end of life, with 30% of Medicare expenditures attributed to the 5% of beneficiaries who die each year. 26 Furthermore, one-third of Medicare expenditures occurring during the last year are spent in the last month.27,28 A meta-analysis of 78 studies involving more than 3.7 million cancer patients found exponential increases in service use and costs as death approached, hospital services being the main cost driver. Palliative care services were underutilized and associated with lower expenditures than hospital-based care. In 15 studies using quality indicators, up to 38% of patients received chemotherapy or life-sustaining treatments in the last month of life, and up to 66% did not receive hospice/palliative services. 29 Timely discussions regarding EOLC might curtail unwanted expensive cancer care. 30 A longitudinal multi-institutional cohort study, Coping With Cancer, demonstrated that these discussions led to fewer life-sustaining procedures, lower rates of ICU admission, and substantially lower total costs.31,32
Our LWC seven-item PRO screening tool was designed to identify patients who could be approached based on their own assessment of distress. The instrument, which measured four domains and accounted for patient-rated importance of each domain, was able to segregate advanced malignancy patients into cohorts at different stages of their cancer journey as assessed by their physician and therefore potentially indicating increasing need for EOLC discussions. The goal of the LWC instrument is to facilitate appropriate timing of advance care planning, palliative care consultation, and hospice referrals by providing an objective metric to oncologists detailing the patient's views of important domains. In addition, the LWC screening tool can serve as the foundation for benchmarking physician practice patterns regarding the timeliness of EOLC discussions. A prospective validation study using serial use of the LWC PRO instrument across multiple sites and correlating the LWC scores against palliative care consultation rates and survival is ongoing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.