
Abstract
Abstract
Background:
Several trials have shown that integrated palliative and oncology care improves quality of life and mood in patients with advanced cancers. However, the degree to which early involvement of palliative care (PC) in the outpatient setting impacts the cost of care remains unknown.
Methods:
Data for this secondary analysis came from a trial of 151 patients with metastatic nonsmall-cell lung cancer (NSCLC) who were randomized to early PC integrated with standard oncology care (SC) or SC alone. We abstracted costs for hospital and outpatient care, including intravenous chemotherapy, from the hospital accounting system. Oral chemotherapy costs were estimated based on actual drug costs. To estimate hospice costs, we used Medicare reimbursement rates. We examined between-group differences in costs of care throughout the entire study period and during the last 30 days before death using the bootstrap-t method.
Results:
The analytic sample includes the 138/151 patients who died by July 15, 2013. Early PC was associated with a lower mean total cost per day of $117 (p = 0.13) compared to SC. In the final 30 days of life, patients in the early PC group incurred higher hospice care costs (mean difference = $1,053; p = 0.07), while expenses for chemotherapy were less (mean difference = $757; p = 0.03). Costs for emergency department visits and hospitalizations did not differ significantly between groups over the course of the study or at the end of life.
Conclusions:
The delivery of early PC does not appear to increase overall medical care expenses for patients with metastatic NSCLC. Larger, sufficiently powered cost studies of early PC are needed.
Introduction
E
Yet, significant barriers limit the widespread adoption of early PC for patients with metastatic cancer. 5 First, PC is a relatively new medical subspecialty, with an insufficient workforce to provide care for each patient with metastatic cancer. Second, costs of care for patients with advanced cancer are exceptionally high, with a mean cumulative total healthcare cost of over $125,000 for patients with metastatic lung cancer. 6 The additional clinical services required by early involvement of PC physicians and nurses may thus increase the already substantial costs of care. Although improving patient outcomes, such as quality of life and symptom burden, is a national priority, early PC in the ambulatory setting will be difficult to disseminate throughout the healthcare system, unless the additional costs of outpatient care are offset by savings in other domains of oncology and end-of-life care.
Within the inpatient setting, PC as a consultative service is associated with reduced costs through lower utilization of healthcare services, such as decreased rates of admissions to the intensive care unit and shorter lengths of stay in the hospital.7,8 Similarly, a study of in-home PC for homebound patients with severe, poor prognosis illnesses showed lower utilization of emergency department and hospital services for patients assigned to the intervention, with resultant cost savings. 9 While PC delivered in the hospital or home setting is associated with decreased service utilization and lower medical care costs, the degree to which early outpatient PC achieves such cost savings for patients with newly diagnosed advanced cancer remains unknown. Compared to hospital or home-based PC, ambulatory care models involve more frequent and long-term involvement of PC clinicians, which may add to the cost of caring for patients with advanced cancer.
We conducted a randomized controlled trial of early PC versus standard oncology care (SC) in patients with metastatic nonsmall-cell lung cancer (NSCLC), observing differences in utilization of medical care services near the end of life for patients assigned to the intervention.1,10 Specifically, patients in the early PC group were less likely to receive intravenous chemotherapy and more likely to have earlier referral to hospice within the final months of life compared to those in the standard oncology care group. 10 These findings suggest that early PC integrated throughout the course of outpatient care has the potential to decrease healthcare utilization and costs at the end of life.
For this secondary analysis, we examined the costs of care for patients who participated in our randomized trial. Based on our previous findings of lower rates of healthcare utilization at the end of life, we hypothesized that costs in the last 30 days of life would be lower for patients assigned to early PC compared to those assigned to SC. Given that the early PC intervention began soon after diagnosis of metastatic lung cancer for participants, we also sought to explore differences in medical care costs between study groups throughout the entire course of illness.
Materials and Methods
Study design and sample
This study represents a secondary analysis of a randomized controlled trial of early PC integrated with SC (n = 77) versus SC alone (n = 74) in patients with newly diagnosed metastatic NSCLCs. We enrolled study participants between June 2006 and July 2009. Patients were eligible for the original trial if they had a diagnosis of metastatic NSCLC within the previous eight weeks, an Eastern Cooperative Oncology Group performance status score = 0–2, and the ability to read and respond to questions in English. Participants assigned to the early PC group met with a board-certified PC physician or advanced practice nurse within three weeks after enrollment and monthly thereafter throughout the course of disease until death. Those assigned to standard care were able to access PC services upon request or at the discretion of the treating oncology clinician. The study was approved by the Dana-Farber/Harvard Cancer Center IRB before enrolling any patients in the initial trial. For the present analysis, the sample included the 138 patients who died by July 15, 2013, but not the remaining seven patients (4.6%) who were still alive or the six patients (4%) who had transferred their medical care to another hospital system during the course of the study. We excluded the living participants as they were still accruing costs at the time of analysis and potentially represent outliers in the sample.
Data collection
We had previously collected data on the number of PC visits, hospital admissions and days, emergency department visits, chemotherapy cycles, and days in hospice from the hospital electronic health record (EHR). In the original publication of this trial, we reported the service utilization figures of the 105 participants who had died by December 1, 2009. For the present analysis, we expanded the EHR data collection on these aspects of care and now report on the utilization and associated cost findings from the larger sample of the 138 patients who died by July 15, 2013.
Costs for study participants were abstracted from the hospital cost accounting system used by Massachusetts General Hospital, Eclipsys Sunrise (EPSi™). Eclipsys (now AllScripts) has embedded reporting and transition costing analysis using data sources, including budgeting and planning, cost accounting, patient financial and clinical analysis, and productivity. Hospital costs (for inpatient and outpatient clinic visits) reported in this study include both direct costs, such as supplies, labor, laboratories, and procedures, as well as indirect costs, such as overhead and building management. The data abstracted from Eclipsys represent the opportunity or resource use cost of care at the institution, rather than the amount charged to the patients' insurance or the amount the hospital is reimbursed for the patients' care.
Costs were calculated based on the visit type, including inpatient care, outpatient care, chemotherapy administration, or hospice care as shown in Table 1. We collected current procedural terminology (CPT) codes and dates of service for all services rendered during patients' visits throughout the trial period. Inpatient costs include all services indicated in Eclipsys as “inpatient,” except for those associated with chemotherapy. Emergency department visit costs included all costs identified by the appropriate CPT codes (99281-99285) plus costs for services (such as laboratory tests) during the same encounter. If patients were admitted to the hospital after an emergency department visit, all costs were captured in the inpatient cost category.
CMS, Centers for Medicare and Medicaid Services; CPT, current procedural terminology; Eclipsys, hospital cost accounting system; EHR, electronic health record; HCPCS, Healthcare Common Procedure Coding System; PC, palliative care.
Outpatient physician costs and all services indicated in Eclipsys as “outpatient,” except for those associated with chemotherapy administration, were included in the outpatient care costs. PC office visits were identified in Eclipsys using the physician code for the PC clinician. Costs for PC visits, including PC visits that took place while a patient was admitted to the hospital, were calculated for the entire study period.
Study participants received both intravenous and oral chemotherapy, including FDA-approved medications and nonapproved FDA drugs as part of clinical trial protocols. We abstracted the cost of intravenous chemotherapy, which includes all medication and administration costs, from Eclipsys. FDA-approved oral chemotherapies are not captured in Eclipsys, as these medications are provided by outpatient pharmacies. Study patients receiving the oral chemotherapy, erlotinib, were assigned a cost (based on the average wholesale price for the year of their death) for a one-month supply of 150 mg pills for each month they were prescribed the drug. Patients receiving the oral chemotherapy, gefitinib, were assigned a cost for a one-month supply that was 20% less expensive than the cost of erlotinib, given the approximate cost difference for these medications in countries where both are available commercially. 11 Patients who received FDA-approved chemotherapy medications as part of a clinical trial protocol that were not captured in Eclipsys were assigned the cost (both medication and administration costs) for each month they were prescribed the drug. Patients who received a non-FDA-approved intravenous chemotherapy as part of a clinical trial protocol were assigned a cost based on the average cost of pemetrexed in the same year the protocol drug was received (i.e., we estimated costs using pemetrexed, given that it was the most recently approved intravenous chemotherapy for lung cancer during the study period). Patients who received a non-FDA-approved oral chemotherapy as part of a clinical trial protocol were assigned a cost of a one-month supply of 150 mg pills of erlotinib for each month they were prescribed the drug (i.e., given that erlotinib was the only FDA-approved oral chemotherapy for lung cancer at the time). We used this approach to estimate costs for the clinical trial medications because no wholesale prices were available for non-FDA-approved chemotherapies.
We calculated the amount of time patients received hospice services as number of days between hospice referral and death. Given that we did not have access to participants' insurance claims data, costs were assigned according to whether the patient was receiving hospice care at home or in an inpatient setting based on the Centers for Medicare and Medicaid Services daily payment schedule. 12 For two patients in the PC group and four patients in the standard care group who received hospice services but had no identifiable date of referral documented in the EHR, we used the median hospice length of stay for the assigned study group. We calculated hospice costs as average Medicare reimbursement for hospice care per day multiplied by the number of hospice days, using the cost for the appropriate fiscal year and hospice location (home or inpatient) based on the year and location of death.
Cost analysis procedures
We performed our statistical analyses using SPSS version 17.0 (SPSS, Chicago, IL) and Stata 13.1. Descriptive statistics were initially calculated to determine the frequencies, ranges, means, and standard deviations of the medical care utilization and cost outcomes. Given that the data were not distributed normally, we used the nonparametric bootstrap-t method (with 1000 replications) to examine cost differences between groups. 13 Of note, participants in the early PC group received more care overall, given their longer median survival compared to those in the standard oncology care group. We therefore examined differences in the average healthcare costs per day throughout the course of disease as well as differences in the total cost of care in the final 30 days of life. The results represent differences in average cost between groups rather than total costs, as such direct costs figures are considered proprietary information as per the policy of our institution. Finally, we calculated the cost-effectiveness ratio of the intervention per life year saved by subtracting the total average cost of care between groups, dividing that number by the mean number of days of increased survival for the early PC group compared to the SC group and multiplying by 365 days for the year.
Results
The baseline characteristics of the sample are shown in Table 2, with no statistically significant differences between study groups. At the time of analysis, 138 participants (91%) had died, for whom we analyzed the medical care utilization and cost data. Of these, 70 were in the standard care group and 68 were in the early PC group. The median time of follow-up for the participants in the sample who had died was 8.1 months.
p-values were derived from two-sided chi-square and Fisher's exact tests for categorical variables and the independent-samples t test for continuous variables.
Fisher's exact test comparing rates of white versus member of a minority group (black and Asian) patients by condition.
An ECOG PS of 0 indicates that the patient is asymptomatic, 1 that the patient is symptomatic but fully ambulatory, and 2 that the patient is symptomatic and in bed less than 50% of the day.
Fisher's exact test comparing rates of platinum-based combination chemotherapy versus “other treatment” by condition.
ECOG, Eastern Cooperative Oncology Group; PS, performance status; SD, standard deviation.
Group differences in cost during entire study period
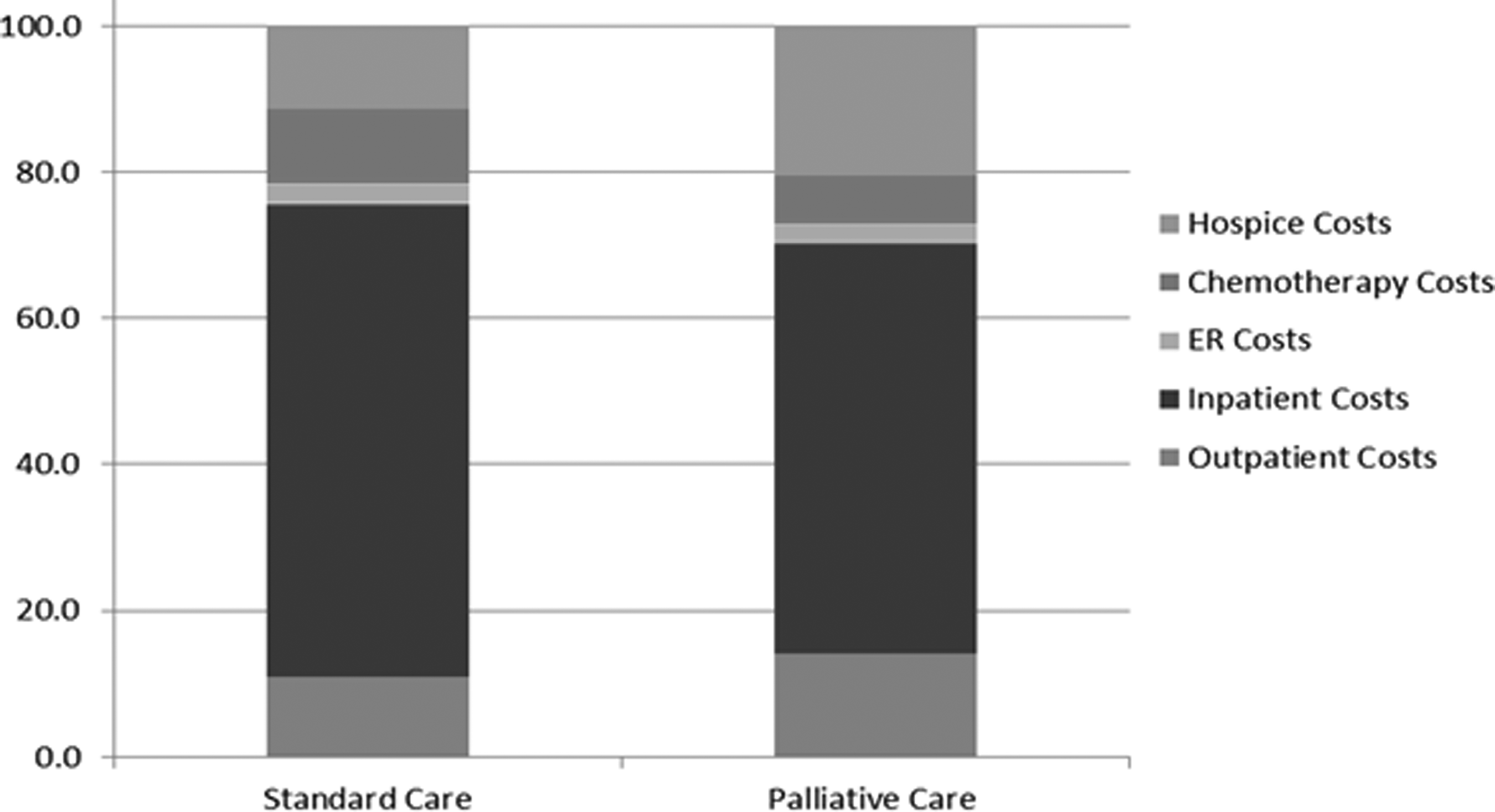
Patients in the standard care group had a total mean cost that was $11,260 less expensive than the early PC group (between-group median difference = $13,664). However, given that participants in the early PC group on average lived 98 days longer than patients in the standard care group, the mean total cost per day for the early PC group was $117 less expensive than the standard care group (p = 0.13). In Table 3, we show the differences between study groups in average total healthcare costs per day alive as well as by subcategory, including emergency department visits, hospitalizations, outpatient visits, chemotherapy administration, and hospice services. As expected, costs for outpatient PC visits were higher in the early PC group (p < 0.001). We also present the breakdown of the healthcare costs by category as a percentage of the total in Figure 1, which descriptively suggests that total healthcare costs in the entire sample were primarily driven by outpatient services. Hospitalizations accounted for a greater proportion of costs in the standard care versus early PC group.

Breakdown of medical care costs by treatment category for entire study period (as a percentage of the total).
p-Values derived from bootstrap-t method.
EPC, early palliative care; SC, ; SE, standard error.
Group differences in cost during final month of life
We also investigated differences between study groups in the total costs of care in the final 30 days before death. As shown in Table 4, patients in the early PC group had a mean cost that was $2,527 less expensive than the standard care group. However, costs at the end of life were quite variable within the study groups, and this difference was not statistically significant (p = 0.44). On closer examination of the subcategories of care (Fig. 2), costs appeared to be less expensive for chemotherapy (p = 0.03) and somewhat greater for hospice care (p = 0.07) at the end of life in the early PC group compared to the standard care group.
Breakdown of medical care costs by treatment category for the last 30 days of life (as a percentage of the total).
p-Values derived from bootstrap-t method.
Cost-effectiveness ratio of intervention
Finally, we calculated the cost-effectiveness of the intervention per life year saved. Using hospital costs, rather than insurance reimbursements, as a measure of resource use, we found that randomization to early PC was associated with a cost-effectiveness ratio of $41,938/life year saved, compared to standard care.
Discussion
In this secondary analysis of a randomized controlled trial of early PC for patients with metastatic NSCLC, we observed a mean savings of $117 (median = $46) per day in the early PC group compared to the standard care group, although this difference was not statistically significant. At the end of life, those in the early PC group had higher costs for hospice services compared to the standard care group, which was offset by lower expenses for chemotherapy administration. Moreover, the intervention cost-effectiveness ratio is below a willingness-to-pay threshold of $50,000/life year saved, 14 representing a good value that third-party insurers typically cover.
Although the present findings are preliminary, it appears that early PC delivered longitudinally during the course of illness may help patients utilize medical resources in a cost-effective manner by shifting care from the inpatient to the outpatient setting and avoiding intensive chemotherapy administration at the very end of life. The collaborative role that PC clinicians play in helping patients and their caregivers to make informed treatment decisions throughout the course of care and at the end of life may partially explain this shift. The present findings expand upon our initial trial results1,10 by confirming the corresponding cost savings associated with patients receiving less chemotherapy near death. However, in this larger analytic sample at a four-year follow-up, the subcategory costs for patients who had at least one emergency department visit or hospitalization did not differ significantly between groups over the course of study or at the end of life. These results should be interpreted with caution, as the study is a secondary analysis that lacks power to detect statistically significant differences in (often skewed) cost outcomes across groups.
Given the increasingly high costs of caring for patients with metastatic cancer, PC represents one method for improving the value and quality of comprehensive cancer care without adding significant medical expenses for treatment. 15 Nonetheless, even with payment reform initiatives, most cancer centers will not be able to employ a sufficient workforce to meet the needs of all patients with metastatic cancer by providing at least monthly consultations from the time of diagnosis. Further work is needed to identify innovative models that clarify the optimal dose and timing of outpatient PC services to achieve such gains for these patients. 16
To our knowledge, the present study is the first to show findings from a cost analysis of early PC for patients with metastatic cancer. The strengths of our approach are the randomized design and inclusion of data from the entire course of care across inpatient, outpatient, and homecare treatment domains. Prior cost analyses of PC services have generally focused within the inpatient setting using observational or case-matched control designs.7,8 Yet, several limitations of our study are worth noting. For example, the results may lack generalizability given the cancer care setting (i.e., within an academic medical center), cancer type (i.e., exclusively metastatic NSCLC), and patient race (i.e., primarily white). In addition, although the original trial was not powered for cost outcomes, the descriptive data are meaningful in suggesting that, at a minimum, the early PC model did not increase the average cost of medical care per day. Furthermore, we examined actual hospital costs rather than insurance reimbursements, although the latter approach may have yielded greater cost savings with early PC. Using the hospital accounting system to abstract most of the cost data, we were unable to capture costs for any services patients received at outside clinics or hospitals, and we had to estimate costs for non-FDA-approved chemotherapies and hospice care. Finally, costs related to patient time and out of pocket expenses were not collected as part of the trial design or included in this analysis. However, the influence of this omission on the conclusion of the study is reduced because PC visits were almost always provided during outpatient or inpatient visits for other treatments, rather than requiring additional travel or time costs for patients in the PC group.
As previously reported,1,10 early PC for patients with metastatic NSCLC leads to a number of beneficial outcomes with respect to quality of life, mood, and resource utilization. In addition, this model of care, delivered in the outpatient setting throughout the entire course of disease, does not appear to increase medical care costs. Rather, early PC helps to ensure the delivery of high-quality, comprehensive cancer care in a cost-efficient manner from the time of diagnosis through the very end of life for those with metastatic lung cancer.
Footnotes
Acknowledgments
This study was supported by the ASCO Career Development Award (PI: Dr. Temel) and gifts from the Joanne Hill Monahan Cancer Fund and Golf Fights Cancer.
Author Disclosure Statement
No competing financial interests exist.