
Abstract
Abstract
Background:
Methadone offers many advantages for treating cancer pain. However, its pharmacokinetic profile makes its use as a full-dose opioid challenging.
Objectives:
To evaluate the efficacy and safety of low-dose methadone as an adjunct to opioids in the treatment of cancer pain in palliative care patients.
Design:
A cohort was followed retrospectively for up to 60 days after the initiation of methadone as a coanalgesic.
Setting/Subjects:
Patients were eligible if they were prescribed methadone as a coanalgesic for cancer pain management and followed by the palliative care team.
Measurements:
The primary efficacy end point was reduction of pain intensity (11-point numerical rating scale). Variables associated with pain intensity reduction were explored using logistic regressions. Adverse events were collected throughout the follow-up.
Results:
Seventy-two of the 146 subjects (49%) qualified as significant responders (≥30% reduction in pain intensity). Median time to significant response was seven days, and pain intensity on the day of methadone initiation predicted the response to treatment. The most frequently reported adverse events were drowsiness, confusion, constipation, and nausea. As expected in a palliative care population, there was a substantial amount of missing data.
Conclusions:
A significant reduction in pain can be seen rapidly after the addition of methadone as a coanalgesic, particularly among patients with high pain intensity. More studies are needed to corroborate the efficacy of methadone as an adjunct to opioids.
Introduction
M
Pain relief remains suboptimal among cancer patients; thus, alternative treatment options need to be explored.17–22 The use of coanalgesics is a well-known approach to improve pain management.10,12,23,24 The coanalgesic use of methadone, defined as adding methadone at low doses to other opioids, is a potential strategy to benefit from its pharmacological properties while minimizing the risks. This novel strategy has been used by a number of palliative care and pain management teams in Quebec as a response to the growing need of cancer pain relief. Although clinical experience indicates the efficacy of methadone as a coanalgesic, little published evidence supports this practice.
To our knowledge, only two case reports25,26 and three case series27–29 have been published on the subject. However, none of these studies used response to treatment to describe the effectiveness of methadone, nor did they determine the subjects who were the most likely to benefit from this treatment strategy. Our study aims at addressing this gap in evidence and at determining whether methadone, used as a coanalgesic, is safe and effective for treating cancer pain. Our primary outcome was to evaluate the reduction of pain intensity using methadone as a coanalgesic. Secondary outcomes evaluated its impact on pain relief, quality of life, and global impression of change as reported by the patient and clinician prospectively. We also assessed variables associated with pain intensity reduction.
Due to recruitment difficulties in the prospective arm, the results of many secondary outcomes will not be included in this publication, as they are of little interest to the reader.
Methods
Study design and participants
This was a cohort study with parallel prospective and retrospective arms. Patients were eligible if they were prescribed methadone as a coanalgesic for the management of pain due to cancer and followed as either an outpatient or an inpatient by the palliative care team at our center. Exclusion criteria consisted of the prescription of methadone for opioid withdrawal, presence of hepatic insufficiency (Child-Pugh class C), or the availability of less than seven days of data. Additional exclusion criteria for the prospective arm were the inability to communicate or give informed consent, or a vital prognosis shorter than one week. Informed consent had to be obtained within seven days of addition of methadone.
Data sources
Computerized medical files of all patients who received methadone in our center were consecutively screened starting from February 3, 2014. Data were manually collected from computerized medical files by investigators using a standardized data collection sheet. Two data sources were used for documenting the primary outcome of pain intensity on the 11-point NRS. First, medical progress notes were screened. Nursing notes were used if data were missing within three days of each follow-up date. In the event that multiple NRS measures were made on the follow-up date, a mean was calculated.
The index date was defined as the date of the first prescription of methadone, and data were collected according to the same prespecified schedule. Cohort exit was defined as death, censoring for any reason, or end of scheduled follow-up.
An independent institutional ethics committee approved the protocol.
Outcomes and measurement
The primary outcome of the study was measured using an 11-point NRS. 30 Subjects were qualified as significant responders if pain intensity was reduced by 30% or more, and as substantial responders if pain intensity was reduced by 50% or more from index date. Responders’ status was determined at each of six predefined assessment time points (day 3, 7, 15, 30, 45, and 60) and overall during cohort follow-up (Supplementary Data Table 4; Supplementary Data are available online at www.liebertpub.com/jpm). Modifications of analgesic treatments (methadone, opioids, and coanalgesics) and adverse events were also collected.
Sample size and statistical methods
Sample size was estimated according to feasibility. We estimated that we could recruit a minimum of 100 patients for the retrospective cohort. Frequency distribution was evaluated using the Kolmogorov-Smirnov tests for normality. Descriptive statistics presenting the median and range were used to summarize the data, since distribution was skewed. Wilcoxon Mann-Whitney rank-sum test was used to compare the methadone dose between responders and nonresponders. Prespecified variables were included in univariate logistic regression models to determine characteristics associated with a significant response to methadone. Statistically significant covariables identified in the univariate logistic regression models and clinically plausible predictors of response were included in the multivariate logistic regression model. Significance was tested at an α of 0.05. Analyses were performed using SPSS (ver. 21.0.0.0) and SAS (ver. 9.3).
Results
Study sample
The files of all 847 patients who received methadone between October 16, 2010 and May 19, 2014 were screened, and 146 subjects were selected (Fig. 1). The main reasons for exclusion were use of methadone for opioid withdrawal, prognosis of less than seven days, and absence of follow-up by the palliative care team (data not collected). Patients could be living or deceased at the time of screening. We excluded one subject for catastrophizing as described by an attending physician in the progress notes, since our measurement tools were not validated for this population. 31 The mean duration of follow-up was 36.4 ± 19.8 days, with a median of 32.0 (interquartile range: 17.8–60.0). Reasons for loss to follow-up were as follows: death (65%), cessation of methadone (17%), and sign-off of care by palliative care team (18%).
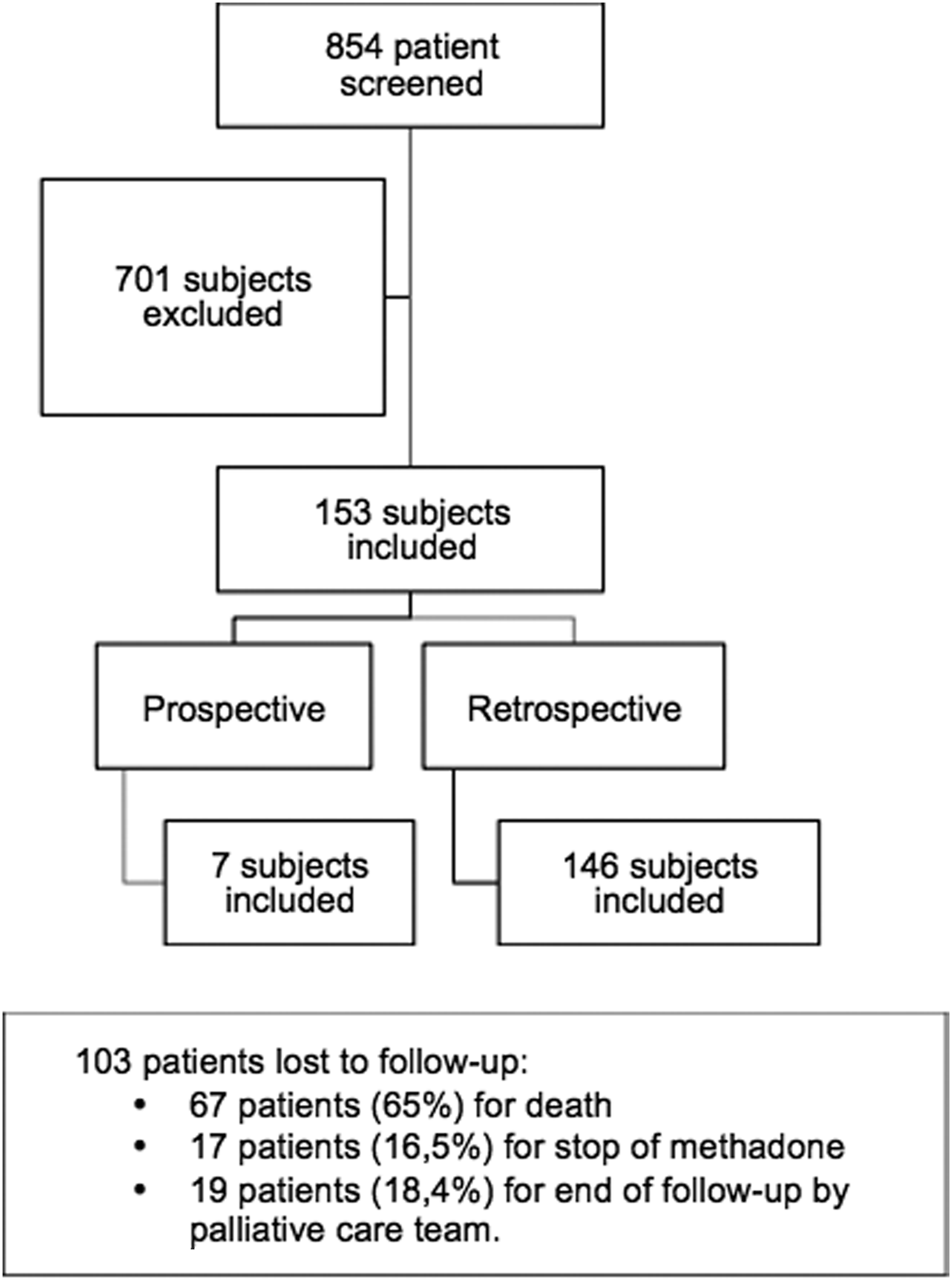
Subject selection.
Demographic and disease-related data
Baseline characteristics at index date are provided in Table 1. The mean age of subjects was 60 ± 12.6 years; 57.5% of subjects were men. Patients were distributed almost equally between levels of medical intervention I, III, and IV. Methadone was started in 110 hospitalized patients (75.3%) and 36 outpatients (24.7%), primarily for the treatment of residual pain despite opioid therapy as perceived by the physician (93.8%). Neuropathic pain accounted for 46.6% of the cohort with somatic and mixed pain (somatic and neuropathic pain) constituting 10.3% and 43.2% of the cohort, respectively. The mean pain intensity at baseline was 5.8 ± 2.4.
All values are presented as absolute number and percentage except when indicated.
Level of medical intervention defined as: (1) maximal interventions; (2) maximal interventions with certain restrictions; (3) maximal interventions aimed at treating reversible conditions; and (4) palliative care.
Treatments
Table 2 provides information on pain treatment at index date. The mean starting daily dose of methadone was 3.5 ± 1.5 mg with a median of 3 mg. The mean dose of regular opioid(s) received in equivalence to oral morphine was 157.4 ± 149.6 mg with a median of 120 mg. Daily doses of as-needed opioid(s) were calculated as an average of as-needed opioids received in the previous 72 hours and converted to the equivalent oral morphine dose.32,33 At index date, the mean of as-needed opioids received was equivalent to 75.4 ± 91.9 mg of morphine with a median of 44.2 mg. Subjects had a median of three coanalgesics.
Primary outcomes
Table 3 provides information on primary and secondary outcome results. Throughout the entire duration of the study, 72 of 146 subjects (49.3% of the original sample) had a significant response (≥30% reduction in pain intensity). The median time to the first significant response was seven days. On days 7 and 15, significant responders had statistically significant lower doses of methadone than nonresponders (p = 0.039 and p = 0.007, respectively). Over the cohort follow-up duration, 44 of 146 subjects (30.1% of the original sample) achieved a substantial response (≥50% reduction in pain intensity). The median time to the first substantial response was three days. On day 30, substantial responders had a statistically significant lower dose of methadone than nonresponders (p = 0.030).
Statistically significant difference in methadone dose between responders and nonresponders.
Mean of as-needed doses received by the subject 72 hours before the time of follow-up.
IQR, interquartile range.
As observed in Table 3, there was a high amount of missing data for the primary outcome. Although information on pain treatment was fully recorded over time for all patients who remained in the cohort, pain intensity was available from medical or nursing notes only for 88 patients at day 7, 60 patients at day 15, and eight patients at day 60.
Secondary outcomes
For the entire cohort and its significant responders’ subgroup, the daily dose of methadone increased gradually over time (Table 3).
The daily dose of regular opioids for the entire cohort remained stable on almost all days of follow-up. Similarly, there was relatively little fluctuation of opioid doses for significant and substantial responders. The median daily doses of as-needed opioids for the entire cohort and the significant responders’ subgroup decreased until day 30, at which there was a sharp increase. Among the substantial responders, the daily doses of as-needed opioids decreased as the study progressed. For the entire cohort, the significant and the substantial responders’ subgroups, the number of coanalgesics taken by the subjects remained relatively unchanged.
Adverse effects were reported in 132 of the 146 subjects (90.4%). Adverse effects in decreasing order of prevalence were as follows: drowsiness (51.4%), confusion (27.4%), constipation (24.7%), nausea (19.9%), and myoclonia (16.4%) (Supplementary Data Table 3). Methadone was held by one subject for several days due to overdose.
There was a high amount of missing data for the secondary outcomes (data not shown).
Predictors of response
Of the variables included in the univariate logistic regression, only the level of medical intervention (odds ratio [OR] 1.38, 95% confidence interval [CI]: 1.00–1.91) and the pain intensity at index date (OR 1.53, 95% CI: 1.22–1.91) yielded a statistically significant influence on the response (Supplementary Data Table 1). Due to a high loss to follow-up and missing data, only five covariables could be included in the multivariate analysis. Of these variables (level of medical intervention, intensity of pain at index, presence of invasive disease, head and neck cancer, and neuropathic pain), only intensity of pain at index date yielded a statistically significant influence on the response (OR 1.65, 95% CI: 1.29–2.12) (Supplementary Data Table 2).
Discussion
A significant response was observed at any given time during the follow-up in half of the subjects with the use of low-dose methadone as a coanalgesic to treat cancer pain. The results show that subjects were more likely to have a significant or substantial reduction in pain intensity during the first week after the start of adjuvant methadone. Not only did the response rate not increase after seven days, but also an increased dose did not translate into a further reduction in pain intensity. Although it is unclear why this happened, we hypothesize that patients who were unresponsive to methadone use as a coanalgesic within the first week were unlikely to respond despite prolonged treatment or increased doses. Therefore, the use of methadone should be re-evaluated after seven days in the absence of response in the clinical setting. A plateau was observed in response to an increasing methadone dose. This suggests that increasing the dose of methadone in patients who respond to a low dose might not further decrease the pain intensity compared with maintaining the same dose until loss of response.
The results of our multivariate analysis showed that subjects who had a higher pain intensity score at index date were more likely to respond to adjuvant methadone. Part of the explanation may be that patients with a higher pain score are more likely to appreciate a decrease in pain. Although the pharmacological properties of methadone would lead us to expect a better response in patients with neuropathic pain, our study was not able to demonstrate this association.
The literature on the use of methadone as a coanalgesic is very sparse. Our study is the first to adhere to the IMMPACT recommendations for clinical trials evaluating pain. 34 Since we used the 11-point NRS scale, a comparison to the available literature is problematic, because measurement of pain outcomes differed from study to study. However, the results are more translatable to the clinical setting, as this scale is practical and easy to use. Leppert and Kowalski 26 published a case report on one subject with lung cancer and observed a reduction of pain intensity from 8/10 to 4/10. Vorobeychik et al. 25 and Wallace et al. 27 used the Visual Analogue Scale (VAS) and the Edmonton Symptom Assessment Scale (ESAS), respectively. Pain score and symptomatology were reduced in both studies. Finally, McKenna and Nicholson 29 and Haughey et al. 28 presented their results descriptively, making direct comparisons impossible. In the existing literature, median starting doses were higher than in our cohorts, with the larger series having initiated methadone at 5–10 mg daily.27,29
Our observational study has a number of strengths. The sample size of our retrospective cohort is the largest pool of subjects studied to date, therefore providing a more global description of efficacy and safety of methadone used as a coanalgesic. The observational nature of this study is a potential strength, as there is no third-party intervention, allowing us to observe real-life effects in the clinical setting. This study is the first to explore factors that predict response to adjuvant methadone using multivariate analyses. Finally, as previously mentioned, this study is also the first to use the IMMPACT recommendations, allowing for easier comparability to future studies.
Our study also has limitations, namely, low recruitment in the prospective arm, short duration of recruitment, and high loss to follow-up. As previously mentioned, recruitment difficulties in the prospective arm constituted an important limitation of our study. Only seven subjects were recruited. The low rate of prescriptions during our four months of recruitment and the use of methadone in patients with a prognosis of less than seven days could explain the failure to achieve a significant sample size. As a result, very little information could be collected on quality of life. Furthermore, the important amount of missing data limited the detection of response beyond seven days of treatment. This problem cannot be avoided given the study population, even with the use of a larger database. However, a larger database would have given the study more power to assess factors associated with response to treatment. We also found that the 11-point NRS was not systematically recorded in patient file progress notes, which contributed to the amount of missing outcome data. As an alternative source, we used the 11-point NRS documented from nursing notes. Even though this was intended to reduce the amount of missing data, we believe that this could have falsely increased the reported pain intensity in these patients, since the nursing team tends to ask patients about their pain intensity when they require as-needed pain medication. In addition, the medical and nursing notes do not specify the formulation of the question for the NRS; therefore, the context of questioning is unknown (e.g., worst pain, least pain, 24-hour average pain, etc.). This bias was reduced in the prospective arm. In the end, despite having used two different sources for the 11-point NRS, there was still an important amount of missing data. Sensitivity analyses could have been done to minimize this bias.
As there is much interest in developing new strategies for the management of cancer pain and very little literature is available on the use of methadone as a coanalgesic, we hope that our study will provide a starting point for future studies on the subject. As we saw that most responses occurred early in the follow-up and that missing data are inevitable with this kind of population, we believe it is unnecessary to continue serial measurements beyond 15 days for the evaluation of the efficacy of methadone as a coanalgesic. A phase 2, double-blind, randomized, controlled trial was recently terminated (January 2015) due to low accrual. 35
Overall, our findings suggest that, in the absence of contraindications, an add-on trial of methadone should not be reserved as a last-line treatment, but might be worth considering earlier for patients presenting with cancer pain of high intensity seeing, as safety and tolerability were good.
Footnotes
Acknowledgments
The authors thank Marc Dorais, MSc, for his assistance with the statistical analyses as well as the palliative care team at the CHUM: A. Côté, F. Monteanu, S. Therrien, L. Laplante, C. Laurendeau, M. Lemonde, F. Collet, G. Dequoy, M. Deneault, J. Ayoub, R. Roberge, M. Lessard, L. Gagnon, M.-F. Thibault, S. Deneault, and P. Vinay.
Author Disclosure Statement
This study is the result of the pharmacy residency research project of D.D., F.C., and F.G. as part of their studies at the Faculté de Pharmacie of the University of Montréal in collaboration with the Centre Hospitalier de l'Université de Montréal (CHUM). Research funds for statistical analyses were provided by the Faculté de Pharmacie of the University of Montréal. D.D., F.C., and F.G. have no conflict of interest to declare. A.N. is an author and the editor in chief of Care Beyond Cure: Management of Pain and Other Symptoms—a complete guide for in-depth understanding of pharmacological approach of palliative care (4th edition 2008; 5th in instance). She received financial sponsorship to develop a methadone drug-interaction pocket-guide (2007; 2010; last update 2012). She is also a guest speaker on palliative care topics at provincial and national congresses. L.T. received fees from Abbvie and Shire companies for giving two lectures in the past five years. A.N. and L.T. have no other relationships or activities that could appear to have influenced the submitted work. All authors participated in the work described in this article, including conception, data interpretation, and the drafting and/or revision of the article. All authors approved the final version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.