
Abstract
Abstract
Background:
There is often little information on long-term prognosis available for Emergency Medicine physicians when decisions on admission, treatment, or consultations are being made for patients. There is a new focus to understand if palliative support should be offered in the emergency department (ED) and the Palliative Performance Scale (PPS), a screening tool used in other settings in palliative care, has been little used in the ED.
Objective:
The goal of this study was to assess the prognostic value of the PPS in predicting three- and six-month survival in patients admitted through the ED.
Design:
A prospective cohort study.
Setting/Subjects:
We evaluated 123 patients over the age of 55 years admitted through the ED of a tertiary care hospital in New England in November and December of 2013.
Measurements:
Each patient's PPS score was evaluated initially in the ED, with follow-up assessments of PPS and survival at three and six months.
Results:
Baseline PPS for the 123 patients was 72 ± 22. Information on 72 subjects (58.5%) at three months was 60 assessed and 12 deaths. Information on 47 subjects (38.2%) at six months was 26 assessed and 21 deaths (nine further deaths from three months). There were no significant differences in the demographics or PPS score in those evaluated and those lost to follow-up at three or six months. Patients with an initial PPS score of 30 or less had 14% survival at six months.
Conclusion:
In this small preliminary study, The PPS score may predict survival in patients admitted to the hospital through the ED. The ease of use holds promise that use of the PPS in the ED may help ED physicians predict survival and plan for better disposition, advocate for patient wishes, and initiate palliative care consultation.
Introduction
E
With an aging population and a gradual increase in the number of ED visits each year, 7 it would be ideal to have a brief, objective, and accurate way to predict prognosis in those patients with severe or disabling illnesses who present to the ED. While it has been shown that measures of physical and cognitive function carry strong prognostic value in hospital outcomes for elders, 8 the feasibility of assessing these variables in the ED has not been well studied. 9 The Palliative Performance Scale (PPS) has been validated as an accurate predictor of survival in multiple settings,10–15 but has limited use in the ED. 16 The PPS incorporates five parameters that are scored by an observer: ambulation, activity and/or evidence of disease, self-care, dietary intake, and level of consciousness. We conducted our study with the purpose of assessing the prognostic value of the PPS for patients in the ED at a tertiary care facility. We hypothesize that the PPS will be an accurate predictor of survival when used in the ED setting.
Methods
Overview
This was a prospective cohort study involving a convenience sample of patients admitted through the ED to XX (removed name to remain blinded), an academic tertiary care facility in XX (removed to remain blinded). The Institutional Review Board at XX approved the study.
Participants
The study was conducted on patients admitted to John Dempsey Hospital (JDH) through the ED between November and December of 2013. Those patients over 55 years were considered for inclusion; excluded from participation were prisoners, patients with a primary psychiatric or obstetric/gynecologic diagnosis, patients not admitted through the ED, transfers to the ED, and those whose hospital stay was less than 24 hours. A list of patients fitting inclusion criteria was obtained by our research staff either while in the ED or from a daily census list. The potential subject was then seen in the ED or hospital for possible enrollment within 24 hours of their admission. Not all patients fitting enrollment criteria were approached given time constraints, as one member of the research team did all recruitment in two days per week during the study period. The days of the week varied so that bias was not introduced into the study. Eligible patients were identified in chronological order by which they were admitted. Our study team member approached the nurse for each patient (either in the ED or hospital floor), discussed our study, and asked the nurse to give each patient a brief Study Introduction Sheet. If the patient then verbally agreed to be approached by our research team, we entered the room and began the official enrollment process.
Data collection
Of the 124 patients approached, 123 provided consent to participate. Only one patient who was approached during the enrollment period declined participation, citing pain as her reason. The study included an in-person interview assessing the following variables: PPS score, age, gender, race, marital status, place of residence, primary diagnosis, and whether or not the patient was currently receiving hospice or palliative care. All patients were initially evaluated by the same research team member (M.B.). PPS scores were determined as outlined by the Victoria Hospice Society, 17 with the exception regarding evidence of disease as described above. The PPS incorporates five parameters that are scored by an observer: ambulation, activity and/or evidence of disease, self-care, dietary intake, and level of consciousness. For the purposes of our study of the second parameter—activity level and/or evidence of disease, we only assessed activity level due to the subjective nature of assessing evidence of disease. The scale is rated from 0 to 100 in increments of 10 (Supplementary Appendix S1; Supplementary Data are available online at www.liebertpub.com/jpm). The initial PPS score reflected the baseline performance status as reported by the patients or their surrogate before the acute event that led to their ED visit and subsequent hospitalization.
Follow-up data collection
The goal was to collect follow-up data at three and six months after the initial enrollment. Each patient was contacted by phone 12 weeks after the initial visit. Three additional research team members performed these phone calls. If the research staff was unable to reach the patient, repeat phone calls were made over the following seven days in an attempt to reach the patient. If after one week or 10 phone calls the patient was still unable to be contacted, the patient was considered lost to follow-up. If the patient declined to continue participating, this was noted.
Data obtained on follow-up phone calls using a scripted interview included the following: assessment of PPS score, place of residence, ED visits since initial enrollment, and whether or not the patient was receiving hospice or palliative care. Deaths were identified through family, Social Security Death Index, local obituaries, or hospital medical records. The date, cause of death, and any other obtainable data were collected and the PPS score was recorded as 0.
Outcomes
The primary outcome was survival. The secondary outcome was a change in PPS score over time.
Analysis
We used Kaplan–Meier survival curves to display survival analysis. Pearson chi-squared and analysis of variance (ANOVA) tests were also incorporated for PPS score change analysis. Cox proportional regression analysis with death at six months as the dependent variable was used to control for age on the association between death and PPS score. All calculations were made utilizing SPSS software, version 19.0.
Results
We reviewed the data from the enrollment period of November 2013 through December 2013. The baseline characteristics of the 123 patients enrolled are shown in Table 1. There were more women than men and most of the patients were Caucasian and arrived from home. The most common admission diagnoses were cardiac disease (predominantly heart failure or syncope), infectious disease (predominantly pneumonia and cellulitis), and abdominal pain (predominantly unknown cause or bleeding). Of the original 123 patients enrolled, 21 patients died. Of the original sample of 123, 26 were alive and completed follow-up to the end of the study. A total of 76 people were lost to follow-up; 51 patients were lost to follow-up at the three-month interval and an additional 25 were lost to follow-up at the six-month interval. We confirmed through the Social Security Death Index and local obituaries queries that no patient lost to follow-up had died.
No patients were receiving hospice or palliative care at time of admission.
The baseline PPS scores ranged from 30 to 100 across all patients, with the distribution as shown in Figure 1. The mean baseline PPS score for all 123 patients was 70.7 (SD: 22.8). There was no significant difference between those reached and those lost to follow-up, specifically in age (78.9 vs. 77.8, p = 0.65), gender (p = 0.15), race (p = 0.99), and PPS score (p = 0.47), respectively.
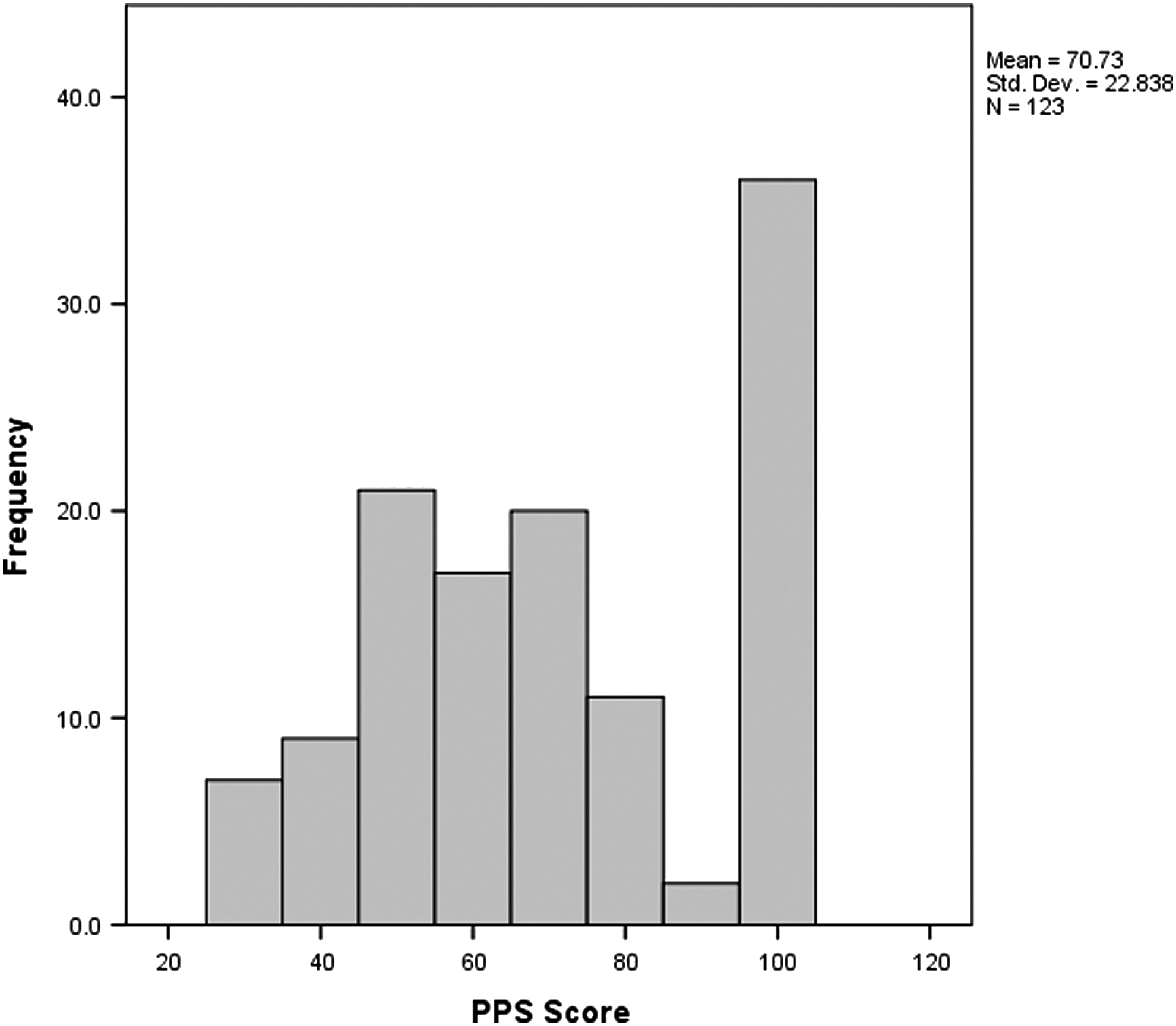
Baseline PPS score. PPS, Palliative Performance Scale.
The average baseline PPS score of the 60 patients who completed follow-up at three months was 74.7 (SD: 23.6) versus 71.67 (SD: 20.4) for those 51 lost (p = 0.47). However, the mean baseline PPS score for the 12 patients who died was 47.5 (SD: 14.8). This represents a significantly lower mean PPS score in those who died than those who did not (p = 0.001 with ANOVA).
The mean baseline PPS score for patients who reached three-month follow-up (n = 34) was 88.5 (20.0). Mean PPS score for the same group at six months decreased to 82.1 (SD: 18.9). Paired sample t tests indicate this was a significant decline in scores (p < 0.001).
Kaplan–Meier survival estimates are shown in Figure 2. We identified three distinct survival curves based on the ranges of PPS score (0–30, 40–60, and 70–100). Survival was measured from time (day) of enrollment to death or survival at 90 and 180 days, whichever came first. A statistically significant difference in survival is noted between the three PPS subgroups at both three and six months (p < 0.001 Log-Rank test for each, 95% CI: 0.00, 273). At three months, PPS scores of 0–30 had a 42.9% survival rate, 40–60 had an 85.1% rate, and 70–100 had a 97.1% rate. At six months, patients with PPS scores of 0–30 had a 14.3% survival rate (mean days of survival 107), 40–60 had a 74.5% survival rate (mean days of survival 151), and 70–100 had a 95.7% survival rate (mean days of survival 175). To understand and control for the impact of age on the association of PPS score with death, Cox proportional analysis revealed B = 3.2 (95% CI: 6.042, 109.365; p < 0.005) for PPS 40–70 and B = 1.8 (95% CI: 1.64, 22.216; p = 0.007) for PPS 0–30. Age had a B = 0.013 (95% CI: 0.970, 1.015; p = 0.562) in the regression.

Kaplan–Meier survival curves at six-month interval with baseline PPS scores stratified into three subsets (0–30 dot-dash [bottom], 40–60 large dash [middle], 70–100 small dash [top]).
Discussion
Our findings indicate that the PPS score may be a predictor of survival when applied in the ED to patients admitted to the hospital and therefore a useful screen for ED providers, although the study is small. While previous studies have shown the PPS to be a predictor of survival in patients already receiving hospice or palliative care,10–15 our study is unique, in that our patient population included a heterogeneous group presenting to the ED. While our patient population is different from previous studies evaluating the PPS, our data are similar to Morita, 18 Harrold, 14 and Head, 11 in that our data report groupings of PPS scores. This is in contrast to Lau's study, 19 which has individual survival curves for each PPS score. Our data did not have a sufficient number of patients with each individual PPS score to substantiate that data. Similar to the findings of the meta-analysis by Downing et al., functional status in the ED, as in palliative populations, seems to predict survival.
The results of our study may offer insight into the use of the PPS as a prognostic tool. In the setting of the ED, limited time and resources place an added burden on the provider to determine which patients may or may not benefit from aggressive life-prolonging therapies.
As suggested by the Choosing Wisely campaign, a system to identify those that would benefit from palliative care needs attention so that ED physicians and healthcare personnel may engage appropriate consults. Given our data, a PPS of 30 or below should be further explored in a larger sample to explore prompting the ED provider to consider engaging available palliative care services at their institution. The PPS may be a simple prognostic tool to help predict survival and may guide emergency clinicians regarding patient and family discussions, subsequent recommendations for treatment, and discharge planning. It may be a guide to emergency physicians on the effective, timely, and appropriate use of palliative care consultation in the ED.
Limitations
There are several limitations to our study. Our study was done at a single center with a relatively narrow demographic range. However, it should be noted that our study subjects were all admissions to the ED, not selected for cancer diagnosis, for example, and the PPS remained predictive of survival. Our patients were not currently receiving palliative or hospice care and were not preselected as they have been in previous PPS studies. In addition, the initial PPS score evaluation was done by a single investigator, while the three- and six-month follow-up score evaluations were done by three separate team members. This may have added variability among the PPS scoring categories, but is a strength in the consistency of the initial PPS and the primary predictor of survival curves. Fifty-one patients were lost to follow-up during the three-month period and an additional 25 patients during the six-month period, although the demographics of patients lost to follow-up did not differ significantly from those who were able to complete the study. We cross-checked each patient lost with the Online Death Index, medical records, and local obituaries; however, we may be unaware of the possible deaths of some patients and may have incorrectly labeled them as lost to follow-up. Finally, our three- and six-month follow-up was done within one week of the three- and six-month date to allow several attempts to contact subjects. We would not expect this variation to significantly impact the PPS score assessed at those intervals.
Future studies are necessary to further validate the role of the PPS in the ED with a broader demographic and larger population. In such a study, each PPS may be evaluated separately for predictive capabilities, further assisting in ED evaluation for services. 10 The current standard of care of ED nursing includes fall risk and mental status assessment, which are components of the PPS. Expanding this assessment to the full PPS warrants further study as it may more clearly identify the most vulnerable patients in the ED.
Conclusion
The PPS may be a useful tool to predict survival in patients over 55 years who are admitted from the ED. It may have implications in early identification of patients who have a high risk of death and may benefit from discussions about goals of treatment and alternate care options. The use of the PPS may further assist providers in assessing disposition and advocating for patient wishes, including palliative and hospice services.
Footnotes
Acknowledgments
The authors would like to express their gratitude to their patients and families for their time and participation, and to Paul Lupia—their extraordinary volunteer. The authors would like to thank the UConn ED staff, Dr. Robert Fuller, and Dr. Thomas Regan for their assistance.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.