
Abstract
Abstract
Background:
Antimicrobials are commonly used in patients near the end of life, but the percentage and predictors of patients prescribed antibiotics while hospitalized on a comfort care protocol are unknown.
Objective:
To determine how often patients in the acute care setting are continued on antimicrobials when they are transitioned to comfort-focused care and to describe patient characteristics correlated with antimicrobial use.
Design:
Retrospective cohort study conducted from June 2012 to August 2014.
Setting:
Two interrelated academic medical centers.
Patients:
Inpatients >18 years old transitioned to a comfort care protocol.
Measurements:
Administration of antimicrobials to patients on the comfort care protocol.
Analysis:
We generated descriptive statistics and used a modified Poisson regression to estimate unadjusted and adjusted associations along with 95% confidence intervals (CIs) and p-values.
Results:
There were 1881 patients included in the study; 77% of patients ultimately transitioned to a comfort care protocol received antimicrobials during their admission and 82% died in hospital. Of the 711 alive at ≥24 hours after comfort care orders, 111 (15.6%) were still on antimicrobials. After adjusting for age, a documented infection was positively associated with being on antibiotics (adjusted relative risk [ARR] = 1.46, 95% CI: 1.00–2.12, p = 0.05). Patients in the medical and surgical intensive care units (ICUs) were less likely than those on medicine to receive antimicrobials (MICU ARR = 0.32, 95% CI: 0.14–0.72, p = 0.01; SICU/Neuro ARR = 0.32, 95% CI: 0.12–0.85, p = 0.02).
Conclusions:
Antimicrobial use is relatively high in hospitalized patients near the end of life, even when the goal is comfort.
Introduction
P
Methods
We conducted a retrospective cohort study of antimicrobial use in inpatients >18 years old who transitioned to comfort care at two academic hospitals from June 1, 2012, to August 1, 2014. We have a standardized “comfort care order set” (CCO); it suggests providers to stop measuring vital signs and laboratory testing and provides standard orders for symptom management. It provides no guidance on antimicrobial use. This order set is used for patients who may die in the hospital or who will transition to hospice care at home or at a facility. Our institutions did not enroll inpatients in hospice during this study period. Patients usually remain on the same unit with the same primary team after CCO, although some patients transfer out of intensive care units (ICUs).
We abstracted demographics, visit information, CCO information, antimicrobials used, infection diagnosis, and diagnostic and death data from Microsoft Amalga, a repository for clinical data from our hospitals. Antimicrobials were defined as antibiotics and antifungals administered by any route. We classified participants into diagnostic groups based on ICD-9 codes specified at any point and types of medical problems (e.g., all malignancies grouped). We generated statistics on all patients on comfort care and the subset still inpatient 24 hours after CCO initiation. We measured the number of patients with CCO and the number still alive at 24, 48, 72, and 96 hours after CCO, along with the proportion receiving antimicrobials 24 hours before CCO and at each time point. Time cut points were calculated based on date and time the CCO was implemented and discharged. Length of stay was calculated based on date and time of admission and discharge.
Among inpatients at 24 hours after CCO, we compared those who did versus did not receive antimicrobials on or after this time, and calculated counts and proportions across factors of interest. We estimated relative risks for being on any antimicrobial in the subset still in the hospital 24 hours after CCO. We used Poisson regression models with a log link and robust error variance to estimate unadjusted and adjusted relative risks (ARRs) and 95% confidence intervals (CIs) and p-values in lieu of logistic regression because our outcome was common. 10 We adjusted for other factors (age and length of stay) that might confound associations. We estimated the proportion still on antimicrobials 24 hours before and 24 hours after CCO by medical service. We determined types of antimicrobials among patients on antimicrobials 24 hours after CCO. All analyses were conducted using Stata 13.0. The UW Human Subjects Division approved this study.
Results
We identified 1881 inpatients with CCO during our study period. One thousand five hundred thirty-seven (81.8%) died in the hospital, 8.2% were discharged home, and 10% went to another facility (Table 1). One thousand four hundred fifty-four (77.3%) patients received antimicrobials during their admission (Table 1). Almost two-thirds of patients received antimicrobials 24 hours before CCO (Fig. 1). After CCO, the proportion on antimicrobials dropped and remained similar across time (Fig. 1). Among those in hospital 24 hours after CCO, those with a documented infection were more likely to be on antimicrobials; however, after accounting for age this finding was not statistically significant (Table 2).
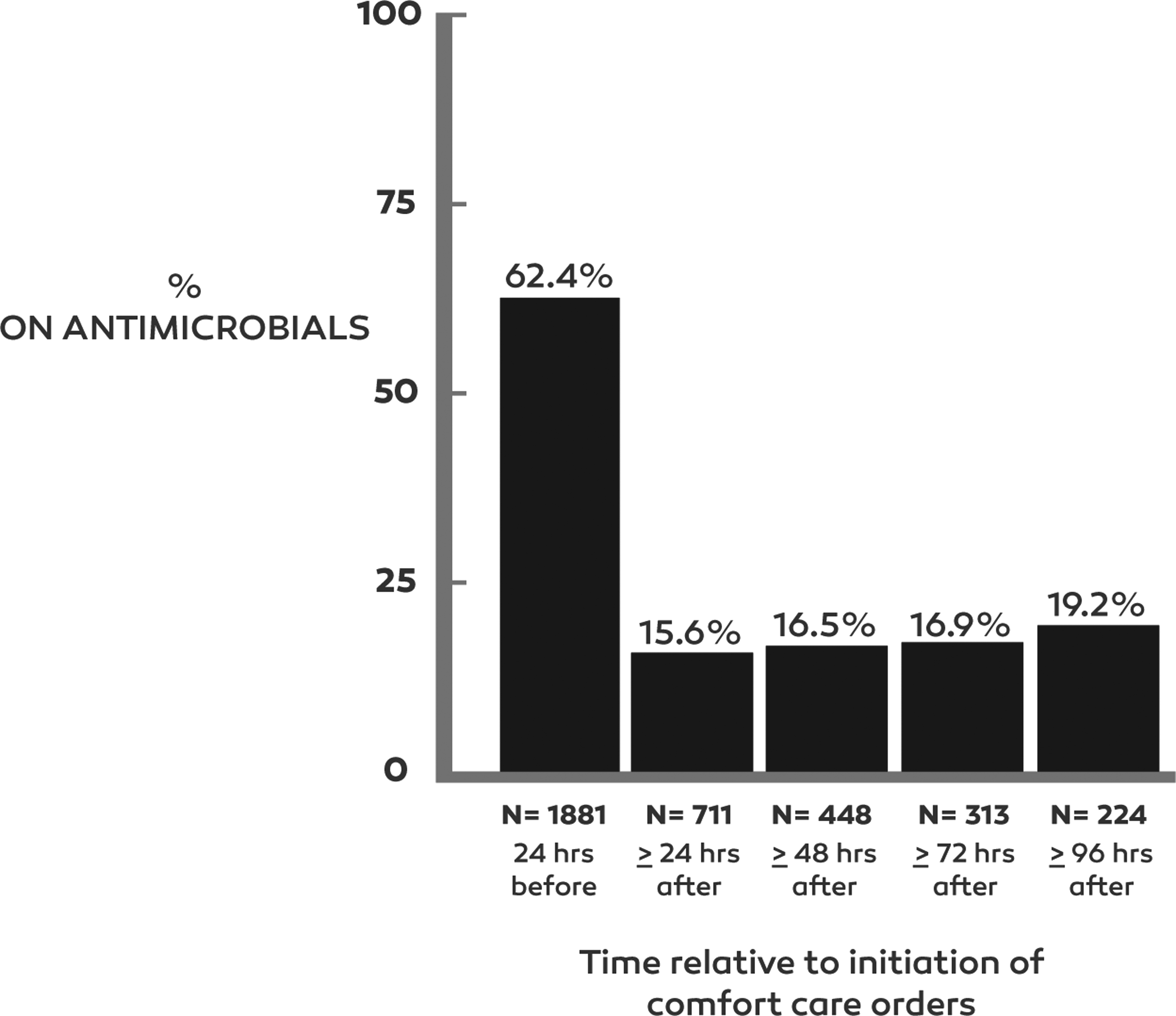
Proportion of patients on antimicrobials by time relative to initiation of comfort care orders.
GI, gastrointestinal; SD, standard deviation.
Age adjusted estimate also adjusted for having an infection.
Age adjusted estimate also adjusted for having an infection, disposition, and length of stay (<7 or ≥7 days); service missing 5.3%.
CCO, comfort care orders; CI, confidence interval; MICU, medical intensive care unit; RR, relative risk; SICU, surgical intensive care unit.
In both unadjusted and adjusted analyses, those with a cancer diagnosis (ARR = 1.44, 95% CI: 1.01–2.06), a longer length of stay (≥7 vs. <7 days, ARR = 1.49, 95% CI: 1.00–2.23), and those discharged home or to a facility (vs. dying in the hospital) were more likely to be on antimicrobials 24 hours after CCO (Table 2) (both p-values <0.001). Patients on a medicine service were most likely to be on antimicrobials, although the only statistically significant differences were between medicine and the medical ICU (MICU; ARR = 0.32, 95% CI: 0.14–0.72) and surgical ICU (SICU)/Neuro ICU (ARR = 0.32, 95% CI: 0.12–0.85). Twenty-four hours before CCO, those on the oncology (79.1%) and medicine (71.9%) services and in the MICU had the highest proportion of patients on antimicrobials (Fig. 2). Twenty-four hours after CCO, Medicine (22.1%) and Oncology (20.0%) had the highest proportion on antimicrobials and ICUs had the lowest.
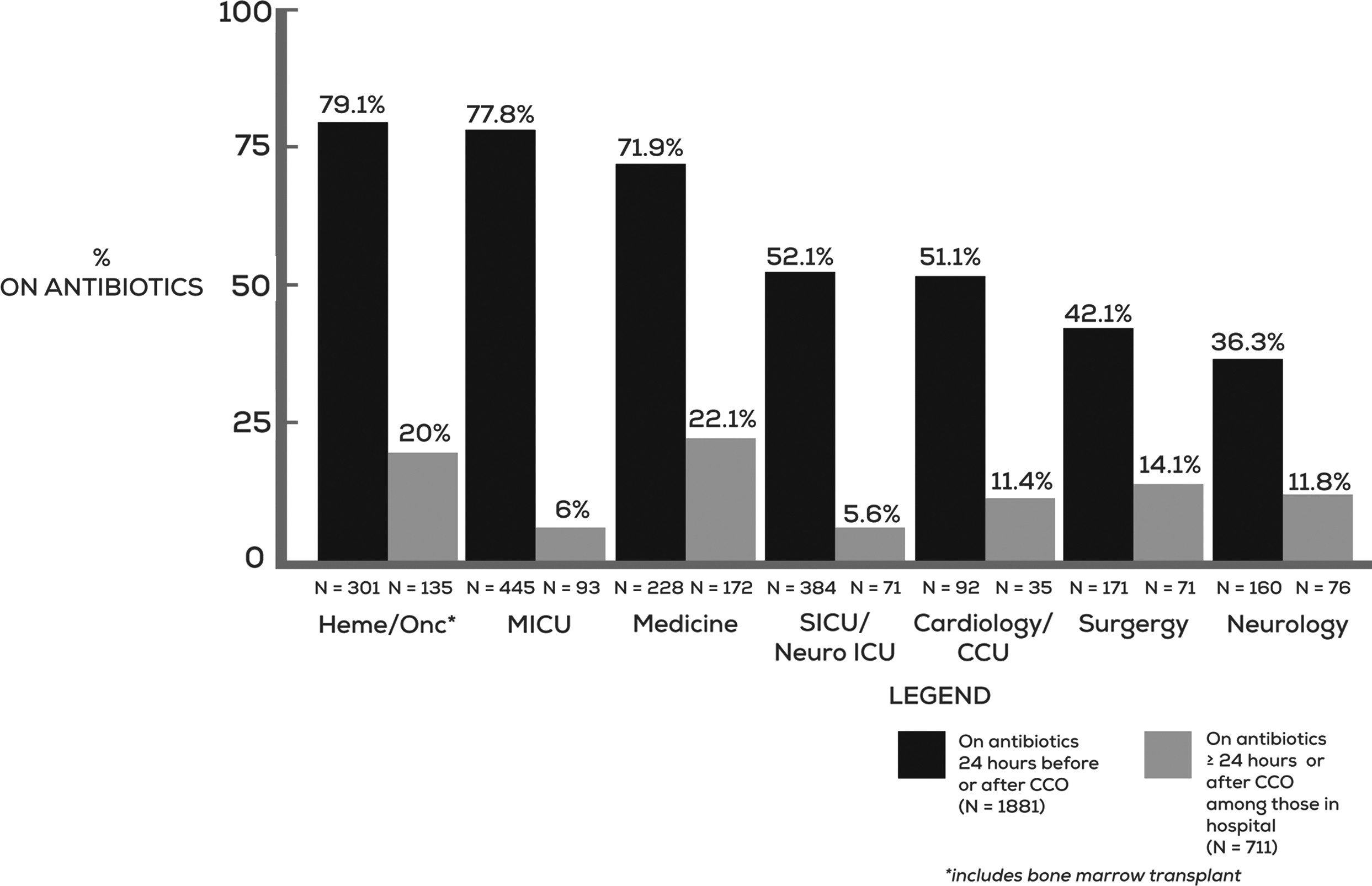
Proportion of patients on antimicrobials while on comfort care by medical service.
Among the 111 patients who received antimicrobials 24 hours after CCO, 44 (39.7%) were receiving intravenous antibiotics, 48 (43.2%) oral only, and 19 (17%) both oral and intravenous. Fluoroquinolones (32.4%) and vancomycin (28.8%) were most commonly administered. Of the 32 patients getting vancomycin, 24 (75%) received it both parenterally and enterally. 21.6% received penicillins, 17.1% cephalosporins, 11.7% carbapenems, 10.8% antifungals, and 51.4% other antimicrobials.
Discussion
Our study shows that antimicrobial use is relatively high at the end of life at our institutions. We found that over three-quarters of patients in our study who were ultimately placed on comfort care received antimicrobials during their hospitalization and between 15% and 20% of patients on the comfort care protocol were on antimicrobials between 24 and 96 hours after the initiation of the order set. This was somewhat lower than the finding in a national cohort of patients on hospice, in which 27% received antimicrobials during their final week of life. 2 It is reassuring that despite the higher intensity of care available in the hospital setting, the percentage of patients given antimicrobials in our study was slightly lower than the percentage receiving antimicrobials while on hospice care in the national cohort.
We hypothesized that teams would continue antimicrobials initially and then discontinue them over time, but this was not the case. We were unable to account for patients who were discharged on antimicrobials, but in this sample, a majority of the patients died in the hospital. Patients with cancer were frequently prescribed antimicrobials in this setting, which is consistent with findings in other studies. This may be due to increased risk of infection, practice variation between oncology providers and other providers, or requests for antimicrobials from oncology patients and/or families. Patients on the general medicine service, and those who were ultimately discharged from the hospital, were more likely to receive antimicrobials after comfort care initiation compared to patients on intensive care services. General medicine providers may have an increased comfort level with the lower-intensity care plan of the comfort care order set and see the benefit of its use even in patients who are not acutely dying.
Consistent with prior work in this field, there was not a strong association between continuing antimicrobials after the initiation of CCO and documenting an infectious diagnosis. This may reflect less rigorous documentation of infections after initiation of CCO. Only gastrointestinal infection and pressure ulcers were strongly associated with continued antimicrobials. There are robust systems within both hospitals supporting the care and documentation of pressure ulcers, which may explain the number of documented pressure ulcers.
The most commonly administered antimicrobials in our sample were fluoroquinolones and vancomycin. Fluoroquinolones carry risks to the patient that may be uncomfortable to patients near the end of life, including neurotoxicity, dysglycemia, antibiotic-associated diarrhea, skin reactions, and Clostridium difficile infection. 11 Intravenous vancomycin requires close monitoring, which may negatively impact comfort. The use of these broad-spectrum agents also has implications beyond the individual patient as follows: transmission of drug-resistant microorganisms may have catastrophic consequences for other hospitalized patients.
Our study has several limitations. Only 111 inpatients in our sample were still on the comfort care protocol at 24 hours, so we could perform limited analyses. Because we used medication administration data, we measured whether antimicrobials were administered in 24 hour increments. We could have missed patients on antimicrobials that were renally dosed less often than every 24 hours or patients who died or were discharged before 24 hours. Diagnoses were based exclusively on ICD-9 codes; for infectious diagnoses, there were no microbiologic, laboratory, or imaging studies available to confirm the diagnosis.
To our knowledge, this is the first study to specifically look at continuation of antimicrobials after CCO in a cohort of hospitalized patients with a variety of diagnoses. From an antimicrobial stewardship perspective, it is encouraging that antimicrobials were often stopped with the initiation of CCO, but we remain concerned that antimicrobials were administered to approximately one-fifth of patients whose goal of care was presumably comfort. What motivated prescribers to continue antimicrobials in imminently dying patients, whether these medications assisted or hindered that goal, and the expectations of providers, patients, and families regarding the ability of antimicrobials to prolong life and/or enhance comfort in dying patients should all be the focus of future study. The results of such investigation may assist in the formulation of evidence-based guidelines for antimicrobial stewardship at the end of life.
Footnotes
Acknowledgment
Funding and support was received from the Institute for Translation Health Science (ITHS) Bioinformatics Consult Team from grant NIH/NCRR ULTR000423.
Author Disclosure Statement
No competing financial interests exist.