
Abstract
Abstract
Background:
Hospital admissions at the end of life (EOL) represent an established indicator of poor quality of care.
Objective:
To examine the impact of intensity of integrated primary and specialist home-based palliative care for chronic diseases (HPCCD) plans of care on EOL hospital access.
Methods:
Retrospective population-based study using linked mortality, hospitalization, and home care data. Intensity of HPCCD was measured 90–31 days before death; outcomes were hospital death and prolonged hospital stay for medical reasons in the last month of life. Outcomes were modeled through Poisson and quartile regressions. Adults aged 65–84 years with at least an ordinary hospitalization and a drug treatment in the year before death, who died from nononcological chronic diseases in the Veneto Region, January 2012–December 2013, were included.
Results:
Among 2087 patients, 1016 (48.7%) did not receive any HPCCD homecare visit; 860 (41.2%), 152 (7.3%), and 59 (2.8%) had <2, 2–4, and 4–7 homecare visits/week, respectively. Hospital death occurred for 1310 patients (62.8%) and the median hospital stay in the last month of life was five days (interquartile range 0–14). In multivariate analysis, a higher intensity of HPCCD was associated with lower rates of prolonged (≥14 days) EOL hospitalization and hospital death with a dose–response relationship. When no access to HPCCD was compared with 2–4 visits/week, adjusted percentage of hospital death decreased by −18.4% (95% confidence interval [CI] −5.4% to −29.7%) and the length of hospital stay decreased by 37.9% (95% CI 16.7%–56.0%).
Conclusions:
The intensity of integrated HPCCD plans of care was associated with a reduction in EOL hospital stay and in hospital death.
Introduction
D
To avoid inappropriate health service utilization and, at the same time, improve quality of life in terminally ill patients, a multidisciplinary team approach centered in primary homecare is mandatory, with a strict coordination between generalist and specialist palliative care.3,7 When appropriate specialist support and facilities are available, general practitioners (GPs) have already been shown to deliver effective palliative care.8–11 However, GPs may have uneven experience, training, and professional interest in this field and, as a result, there is still limited evidence to gather an on-going debate regarding the impact of integrated primary and specialist palliative care on EOL hospital utilization and quality of care. 12
The purpose of the present study is to evaluate the impact of intensity of a Home-based Palliative Care for Chronic Diseases (HPCCD) plan of care on place of death and length of hospital stay for medical reasons over the last 30 days of life.
Methods
Setting
In Italy, several regulatory measures have recently strengthened palliative care services.13,14 In particular, the approach of the Veneto Region is characterized by an emphasis on the integration among health professionals involved in HPCCD: GPs, nurses, out-of-hours physicians, and palliative care physicians.15,16 When a chronic disease patient needs to receive home-based palliative care, he/she is referred to the health district to undergo a multiprofessional and multidimensional evaluation, leading to a tailored integrated homecare plan. Less intensive integrated HPCCD plans of care are implemented by health district nurses (24 hours/7 days) and the GP under the supervision of the palliative care specialist. The GPs are generally readily available on call 12 hours/5 days with on-call physicians providing coverage for the rest of time. More complex integrated HPCCD plans of care are directly carried out by a dedicated palliative care unit (24 hours/7 days palliative care nurses and palliative care specialists readily available on call 12 hours/7 days).
Study population
This study included patients residing in the Veneto Region, aged 65–84 years, who died from nononcological chronic diseases between January 1, 2012, and December 31, 2013. The chronic diseases indicative of palliative care need were selected according to death certificates and the list proposed by the Global Atlas of Palliative Care at the End of Life. 3 Nononcological chronic diseases as causes of death of patients included in the study are reported in Table 1. The following exclusion criteria were applied: (1) patients who died at 85+ years of age (as they often live in nursing homes, thus not eligible for HPCCD plan of care); (2) patients who died by accidents, tumors, acute myocardial infarction, stroke (as they do not generally show the typical EOL illness trajectory and pattern of care); (3) patients not hospitalized and not undergoing drug treatment between 365 and 91 days before death (as they were probably not affected by a severe chronic disease); and (4) patients deceased in a nursing home or hospice or discharged in a nursing home 90–31 days before death (Fig. 1).
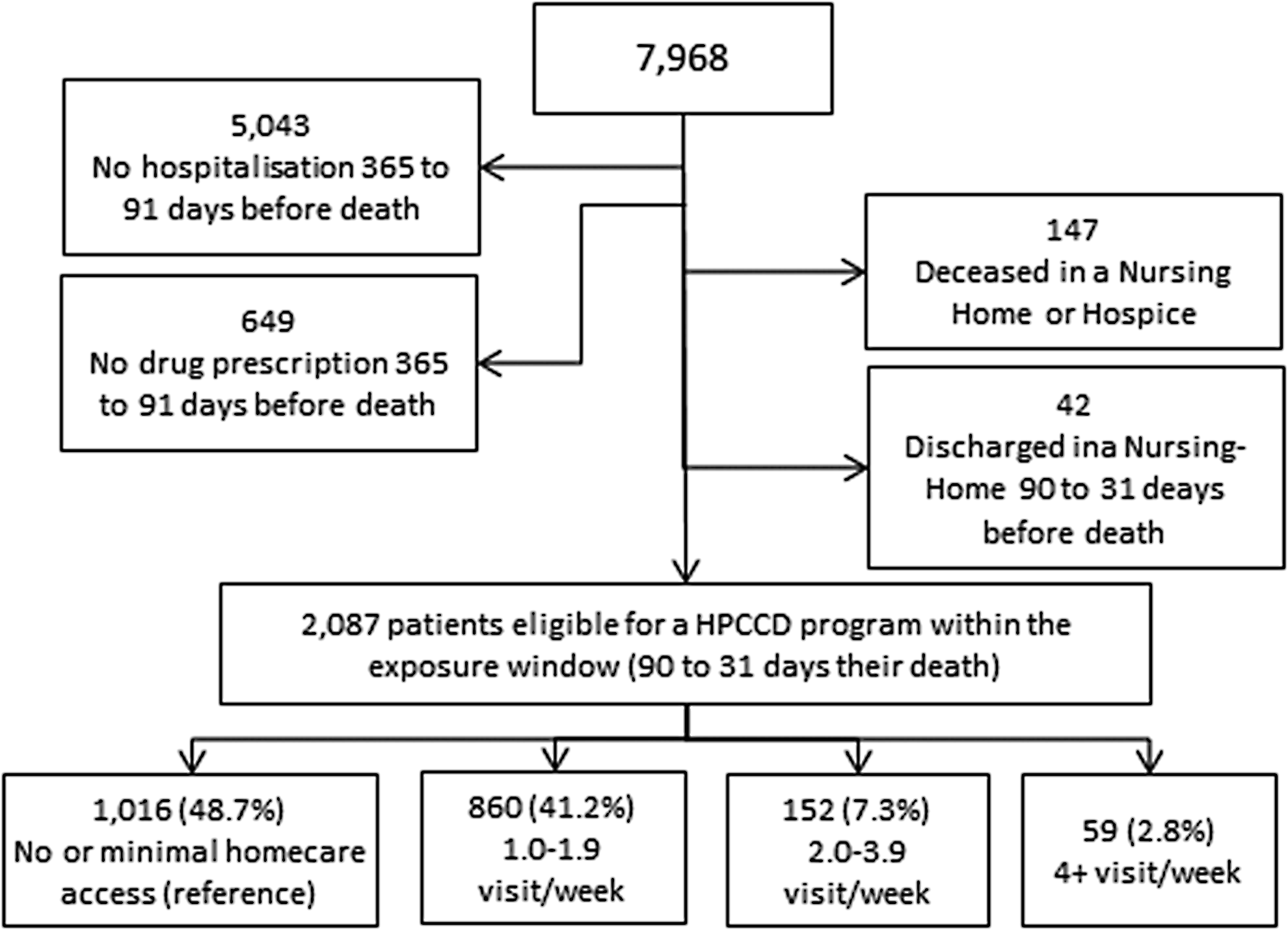
Definition of the study population. Deaths from selected chronic diseases in patients aged 65–84 years (13 local health units of the Veneto Region, 2012–2013). HPCCD, home-based palliative care for chronic diseases.
L*, all codes of the ‘Diseases of the skin and subcutaneous tissue’ chapter in International Statistical Classification of Diseases and Releated Health Problems, 10th Revision. (ICD) M*, all codes of the ‘Diseases of the musculoskeletal system and connective tissue' chapter in ICD-10.
According to the Italian law on privacy (DL 196/2003), the study is exempt from Ethics Committee approval and no specific written consent is needed as data were anonymized by the regional statistical office by means of a unique identifier.
The analysis was limited to 13 local health units (of 21 within the Veneto Region), which reported an accurate registration of the dates of HPCCD visits made by GPs, for a total population of about 2.9 million inhabitants. Data on healthcare utilization in the EOL of all selected decedents were retrieved from Regional Hospital Discharge records (2011–2013), homecare visit records (2012–2013), and hospice records (2013). Death in hospital was defined as a death occurring in the hospital according to Hospital Discharge records. Prolonged EOL hospital stay for medical reasons, considering only medical diagnosis-related groups, was defined as a stay exceeding the 75th percentile of stay that occurred during the last 30 days of life.
Statistical analyses
Two distinct time windows were defined: an exposure window between 90 and 31 days before death and an outcome window corresponding to the last 30 days of life. Intensity of HPCCD plans of care was classified into four categories by grouping patients receiving no homecare access, <2, 2–4, and 4–7 visits per week, the denominator being days spent at home. The association between the four HPCCD categories and the study outcomes was assessed by quartile regression (prolonged EOL hospital stay) and robust Poisson regression (death in hospital). Covariates included in the regression models were gender, marital status, Charlson Comorbidity Index (derived from hospital discharge diagnoses, four classes: 0, 1, 2, 3+), number of hospitalizations occurring 365–91 days before death (two classes: 1, 2+), number of hospitalizations that occurred 90–31 days before death (two classes: 0,1+), underlying cause of death (five classes: Cardiovascular Diseases and Diabetes [taken as reference]; Neurological Disease and Dementia; Respiratory Diseases; Liver and Kidney Diseases; and Frailty Markers, Cutaneous, Subcutaneous, and Rheumatological Diseases). All statistical analyses were performed using Stata, version 13; a value of p < 0.05 was considered statistically significant.
Results
The linkage of the three sources identified 2087 patients who died from chronic diseases in the study period. Their main characteristics are described in Table 2. The majority of patients were male, older than 75 years, and married. The Charlson Comorbidity Index was greater than zero in 83.9% of subjects; 41.3% had two or more hospitalizations between 365 and 91 days before death and 43.1% had a further hospitalization 90–31 days before death.
Almost half of the patients (n = 1016; 48.7%) were not included in any HPCCD plan of care, with remarkable differences among local health units (range 39.2%–65.4%). On average, 860 (41.2%), 152 (7.3%), and 59 (2.8%) patients received, respectively, <2, 2–4, and 4–7 homecare visits/week during the exposure period, while 130 (6.2%) received the first homecare visit 90 days or less before death. Among patients entering an HPCCD plan of care, the median number of homecare visits during the observation period was 7 (interquartile range [IQR] 3–14); visits were made mostly by nurses (72.6%), followed by GPs (21.1%). Palliative care physicians made 2.0% of the homecare visits (4.1% among those receiving 4+ visits/week during the exposure period).
The overall percentage of patients who died in hospital was 62.8% (n = 1310, range among local health units 52.9%–71.4%), while the median duration of EOL hospital stay for medical reasons was 5 days (IQR 0–14, with range of 2–7 days among local health units); 956 (45.8%) and 502 patients (24.1%) had an EOL hospital stay of 7+ and 15+ days, respectively.
Risk factors for death in hospital and prolonged EOL hospital stay (≥14 days) are shown in Table 3. After adjustment for other known factors, patients with previous or recent hospitalization had an increased risk of hospital death and prolonged EOL hospital stay for medical reasons. An increased risk was also observed for patients who died from liver and kidney disease as well as from respiratory diseases (only for hospital death).
Statistically significant results are reported in bold.
Quartile regression (75th percentile).
Robust multivariate analysis.
CI, confidence interval; EOL, end of life; RR, relative risk.
The relative risk (RR) of hospital death and prolonged EOL hospital stay decreased with a dose–response relationship, according to the number of homecare visits/week performed 90–31 days before death. Prolonged EOL hospital stay significantly decreased when 2+ visits/week were provided, when compared with patients with no homecare visits. The value of the 75th percentile of the adjusted number of ordinary hospital days in the last 30 days of life dropped from 15.63 (95% confidence interval [CI] 14.37–16.90) to 9.50 days (95% CI 4.32–14.67) with a relative reduction of 39.3% (95% CI 5.5%–68.0%). A decreasing trend in hospital death was also observed, although it was significant only for the category 2–4 visits/week (−18.4%, 95% CI −5.4% to −29.7%).
Discussion
Our findings showed that almost half of the patients dying from nononcological chronic diseases received minimal or no homecare access between 90 and 31 days before death, with a wide range across local health units. About one-third of patients received <2 homecare visits/week between 90 and 31 days before death and only about one-tenth received 2+ visits/week. Hospital death and prolonged EOL hospital stay for medical reasons were reduced at increasing intensity of homecare visits, with a dose–response relationship.
Population-based data on the number of people receiving palliative care in Europe are scarce. A recent study—based on a standardized questionnaire retrospectively filled by a sentinel network of GPs in the Netherlands, Belgium, Italy, and Spain—similarly shows that 50%–65% nonsudden decedents received primary palliative care in the last three months of life, while 29%–47% received specialist palliative care, with a median duration of 15–30 days before death. 17 Unlike cancer patients, who generally have an EOL trajectory characterized by a short period of evident decline, chronic patients are better described by trajectories of (1) long-term limitation with intermittent serious episodes, sometimes leading to hospital admissions (e.g., heart failure or chronic obstructive pulmonary disease), and (2) prolonged dwindling due to dementia or generalized failure of body systems.18,19 As a result, the EOL trajectory of chronic patients in most cases is not easily predictable and patients with organ failure and dementia receive a smaller amount of primary and specialist EOL palliative care compared with cancer patients.17,20
The population of nononcological chronic patients eligible for palliative care is quite elusive; the WPCA-WHO Global Atlas of Palliative Care at the End of Life recently proposed the following list of diseases: cardiovascular diseases, cirrhosis of the liver, endocrine, blood, and immune disorders, kidney disease, neurological disorders, protein energy malnutrition plus HIV/AIDS, tuberculosis, and other pediatric conditions. 3 The presence of pain as well as of other stressful symptoms (e.g., dyspnea, anorexia, severe energy loss, mental confusion with behavioral problems, insomnia, and low mood) or of care delivery problems conducing to health needs is usually high among these patients during the last year of life.2,21 In the present study, only decedents aged 65–84 years with a hospitalization that occurred 365–91 days before death and with drug prescriptions were chosen to better identify EOL trajectories requiring palliative care. Other approaches have been recently proposed to obtain a more precise estimate of people needing nononcological palliative care, integrating information from both underlying and contributory causes of death and previous hospitalizations; if the focus is on home palliative care, disability is of great importance as well.19,22,23
A direct measurement of the population-based prevalence of advanced chronically ill patients with limited life prognosis in need of palliative care has also been recently implemented in Spain; 24 this important study has been carried out by healthcare professionals using a standardized tool across all settings of care. More prospective research is surely needed for a timely and reliable recognition of patients eligible for integrated HPCCD in the Veneto Region.
Most reviews and experimental studies about the impact of home-based palliative care on EOL hospitalization refer to cancer patients,4,25 but some trials report on a miscellanea of cancer and noncancer patients11,26–28 or patients affected by chronic heart failure and chronic obstructive pulmonary disease.29–31 Experimental studies do have their limits: target populations, team compositions, models of interventions, and usual care definitions are very heterogeneous; balance, blinding, attrition, power calculation, and intention-to-treat analysis are often troublesome. 25 For these reasons, observational studies can contribute as well.
A relationship between the intensity of homecare visits and hospital EOL utilization has already been described in a few population-based observational studies of terminally ill patients, with shares of nononcological patients widely ranging from 20% to 75%8,9,32–35; the timeliness of initiation of homecare visits can be influent as well. 32 Unlike other observational studies, this one focuses only on nononcological decedents; patients dead from liver and kidney diseases and COPD and respiratory diseases show poor outcomes and attention is also drawn to a broad spectrum of rheumatologic diseases that can lead to severe frailty and bedsores. 6 As a statistical issue, robust Poisson regression provides a more precise estimate of the effect size given that the event is not rare and odds ratios (ORs) estimated by logistic regression would overestimate the effect size. 36 Were ORs instead of RRs (through a robust Poisson regression) calculated in this study, an intensity of 2–4 homecare visits/week would be associated with an OR of death in hospital equal to 0.57 (95% CI 0.39–0.82), which is not far from the results of experimental or quasi-experimental studies.2,25,33
Our findings suggest that some diseases (identified on the basis of the main cause of death) may be more difficult to treat at home, requiring a prolonged hospitalization at the end of life or necessitating a hospital death. COPD is frequently associated with stressful symptoms such as shortness of breath, exhaustion, and pain, being identified as a critical area also in a previous population study. 37 Hepatic and renal failure involves important signs and symptoms (e.g., icterus, bleeding diathesis, neurological symptoms, asthenia, and vomiting). These complex diseases request a high intensity of care, thus specific clinical skills are needed, as well as good training and better integration of care between specialists and of palliative care physicians.
This study has some strengths: it has a population basis and takes into account home visits provided by both primary and specialized healthcare professionals, within an integrated holistic view of the continuum of care. 6 It is also, to our knowledge, one of the first population-based studies comparing EOL hospital outcomes in a terminally ill nononcological patient receiving palliative care.
The study has limitations as well: the approach is retrospective 38 and the definition of health problems of the target population is based on the underlying cause of death, which poorly captures both palliative care needs and trajectories of EOL disability.18,19,23 Other relevant outcomes such as quality of life, symptoms, and caregiver outcomes have not been investigated due to the intrinsic limits of claims data.4,12,39 The study size is not large, especially for decedents receiving 4+ visits per week. Last, we included in the analyses only 13 of 21 local health units since they provided reliable data for homecare visits performed by GPs. Our regional model of palliative care for chronic diseases cannot be generalized to other countries and is itself still in development.15,16 The integrated palliative care coverage is not yet uniform throughout the region. The palliative care specialist visits may be to some degree underreported in some local health units. Yet, most of the time spent by palliative care specialists to supervise these chronic nononcological patients is devoted to contacts with hospital specialists, to multidimensional evaluation, and to discussion/revision of the customized palliative homecare plans with GPs and health district nurses; staff education, advice, and guidance are of great importance as well, thus leaving little time to home visits of selected patients.
The vast majority of EOL home visits is made by nurses, so their education and coordination (daily and weekly coverage, shift scheduling) are of foremost relevance. During the visit, nurses control symptoms and general conditions of patients in a standardized way; when necessary, they perform both simple and complex healthcare services (e.g., medication, infusions, catheterizations, transfusions). The GPs can further improve their recognition of nononcological patients needing palliative care, thus improving a timely integration with the palliative care units.40,41 Of interest, the Dutch model puts a strong emphasis on GP palliative formal education and GPs represent the main providers of formal care for terminally ill cancer and noncancer patients. 17 The integrated primary and specialist palliative care approach has also been recently tested in Italy by means of a pilot study involving about 100 GPs enrolled within 10 palliative care units: a range of clinical, psychosocial, and communication actions was implemented, ensuring continuity of care and proportionate treatment and avoiding an unnecessary quality-of-life deterioration in cancer and chronic patients with low life expectancy and high need of palliative care. 42
Our preliminary findings need to be confirmed by further research, which could take into account other important variables that may impact the quality of EOL care, such as goal of care and level of social support at home. Furthermore, more research is needed to clarify the reasons why study outcomes varied by cause of death.
Conclusions
Integrated primary and specialist palliative care can be provided to terminally ill patients with nononcological diseases in a population-based way to reduce the risk of inappropriate hospital stay and death. A multidisciplinary approach involving GPs, nurses, out-of-hours clinicians, and palliative specialists may be of great help, overcoming communication problems between settings and providers of care and actively exploring any problem that may reduce patients' quality of end of life.
Footnotes
Author Disclosure Statement
No competing financial interests exist.