
Abstract
Abstract
Background:
Evidence on the impact of pediatric palliative care programs (PPCP) on resource utilization is scarce and requires broader measures to include utilization beyond the hospital setting.
Objective:
This research aims to provide a Canadian comparative analysis between children in a PPCP with those under usual care, including hospice use to inpatient resource use measurement.
Methods:
We conducted a retrospective matched-pairs (disease and age at death) cohort comparison of children who died in hospice versus hospital (never enrolled in a PPCP), from 2008 to 2012. Utilization was retrieved from administrative databases and chart review. The main outcomes were number of admissions and length of stay (LOS).
Results:
Eleven pairs were found. PPCP users were more likely to have advanced directives (100% vs. 27%). After controlling for disease and age, we found no significant difference in number of admissions; however, PPCP users had an increase in admissions post-referral compared to pre-referral (median 3.08 admissions), driven by the need for critical care. We did not find a significant difference in LOS, but observed longer admissions among PPCP users pre- (1.91 days/month) and post-referral (3.66 days/month) compared to usual care. Over 60% of inpatient utilization shifted to the hospice post-referral.
Discussion:
The terminal pediatric population referred to PPCP may systematically differ from those under usual care even before enrollment, presenting with higher inpatient utilization in critical care nearing death. A significant portion of inpatient utilization shifted to the hospice, with implications for resource reallocation and enhancements in PPCP referrals.
Background
P
There is a prevailing belief that pediatric palliative care programs (PPCPs) can improve the efficiency of healthcare delivery through the coordination of care offered beyond hospital settings, more specifically in hospices or at home. A systematic review on the impact of pediatric home care 3 found a decreased burden of care and costs for families and reduced acute care admissions. However, children still require inpatient care from time to time. Another systematic review 4 demonstrated that PPCP users have shorter length of stay (LOS). Yet, only one study to date has measured days spent in hospice, in which LOS was found to be longer, demonstrating a shift in healthcare setting rather than a decrease in healthcare utilization. 5 Nonetheless, the impact of this shift and resource allocation from tertiary to hospice care and PPCPs remain outstanding questions.
British Columbia's (BC) pediatric population is served by BC Children's Hospital (BCCH), which works with the holistic hospice-based PPCP Canuck Place Children's Hospice (CPCH). CPCH coordinates care across the publicly funded healthcare settings and its operation directly affects hospital inpatient admissions. Therefore, CPCH offers an appropriate setting to investigate important resource reallocation questions.
Objective
We examined utilization of healthcare resources, including hospital and hospice care, of children enrolled in CPCH compared with those under usual care at BCCH.
Methods
Design
Assumptions made at study outset are described in Figure 1 and detailed in Appendix 1.6,7 We used a retrospective cohort comparison of children who were residents of BC and died from life-threatening conditions (LTCs) between January 2008 to December 2012 in hospice (hospice users) versus hospital (controls). Pairs were matched by disease code and age at death. Data were extracted from the hospice database, cancer registry, BCCH administrative database, and chart review. We obtained monthly utilization of health services (number, type, and acuity levels) for up to three years before death. Each outcome measure was converted to a rate per patient per month.

Process of delimitation of pre- and postreferral periods.
The matching process was initiated with the entire deceased population at CPCH during the study period (n = 100, 41% from cancer). Matches were sought among those who died at BCCH. Medical notes from chart and cancer registry reviews confirmed primary diagnosis. Children not receiving palliative care, who died as a consequence or complication of curative treatments, were excluded. Once paired by cancer type, an oncologist assessed the implication of age difference within pairs on treatment course. If different treatments for the same cancer could have been used (e.g., radiotherapy + chemotherapy + surgery vs. chemotherapy + surgery), the pair was excluded. Ethics approval was obtained from the Research Ethics Board at BCCH (CW13-0210/H13-01162) and the CPCH Research Committee.
Analyses
We plotted average LOS in both cohorts by months before death to understand trends overtime. To explore the shift in healthcare setting, we computed the mean LOS by facility. We performed pairwise comparisons within cohorts (pre- vs. postreferral) and between cohorts (hospice user vs. usual care control, age- and disease-matched pairs). Pairwise comparisons are based on the median difference between pairs. We applied the Wilcoxon signed-rank test. A two-sided test was employed, and 95% confidence intervals were calculated. Statistical analyses were conducted using R software© (Version 0.98.507 2009).
Results
Demographics
A final sample of 11 pairs was found. Overall, hospice users had more advanced directives in place compared with their matches (100% had “Do not attempt resuscitation” directive vs. 27% of controls, p = 0.013). Despite no other significant differences in age and gender distributions between groups, the hospice group was 1.5–2.8 years younger and predominantly female. The mean observation period was 23.4 months, and mean length onto program was 89 days (Table 1).
DNAR, do not attempt resuscitation; LOP, length onto the program; SD, standard deviation.
Number of admissions
Hospice users had significantly more admissions in the postreferral period compared with controls (Table 2) and a significant increase in monthly admissions compared with prereferral. The results seem to be driven by the number of admissions in critical care beds (intensive care at the hospital or high acuity beds at the hospice). No statistically significant changes were observed among controls. When exploring the shift in healthcare setting, the majority of postreferral admissions among hospice users occurred in hospice (>70%), despite being critical care admissions (Table 3).
CI, confidence interval.
Pair #78 was excluded from the prereferral period as the hospice user was a newborn enrolled in the program from birth.
SD, standard deviation.
Length of stay
Outpatient visits remained roughly the same, while inpatient admissions increased toward death in both groups (Figs. 2 and 3). Similar trends were observed in both groups until ∼15 months before death, when inpatient utilization diverged. Hospice users consumed more healthcare resources in this period on average, especially in the last 2 months of life, when they required more critical care. Children enrolled in the palliative care program from 12 months to 2 days before death, with a maximum enrollment rate of 67% in the last month of life (not all program users were enrolled for the full month before death). Referral close to death is a plausible explanation for not finding significant differences when comparing aggregate data from pre- to postreferral.

LOS per person/month at risk over time, by arm: outpatient and inpatient admissions.
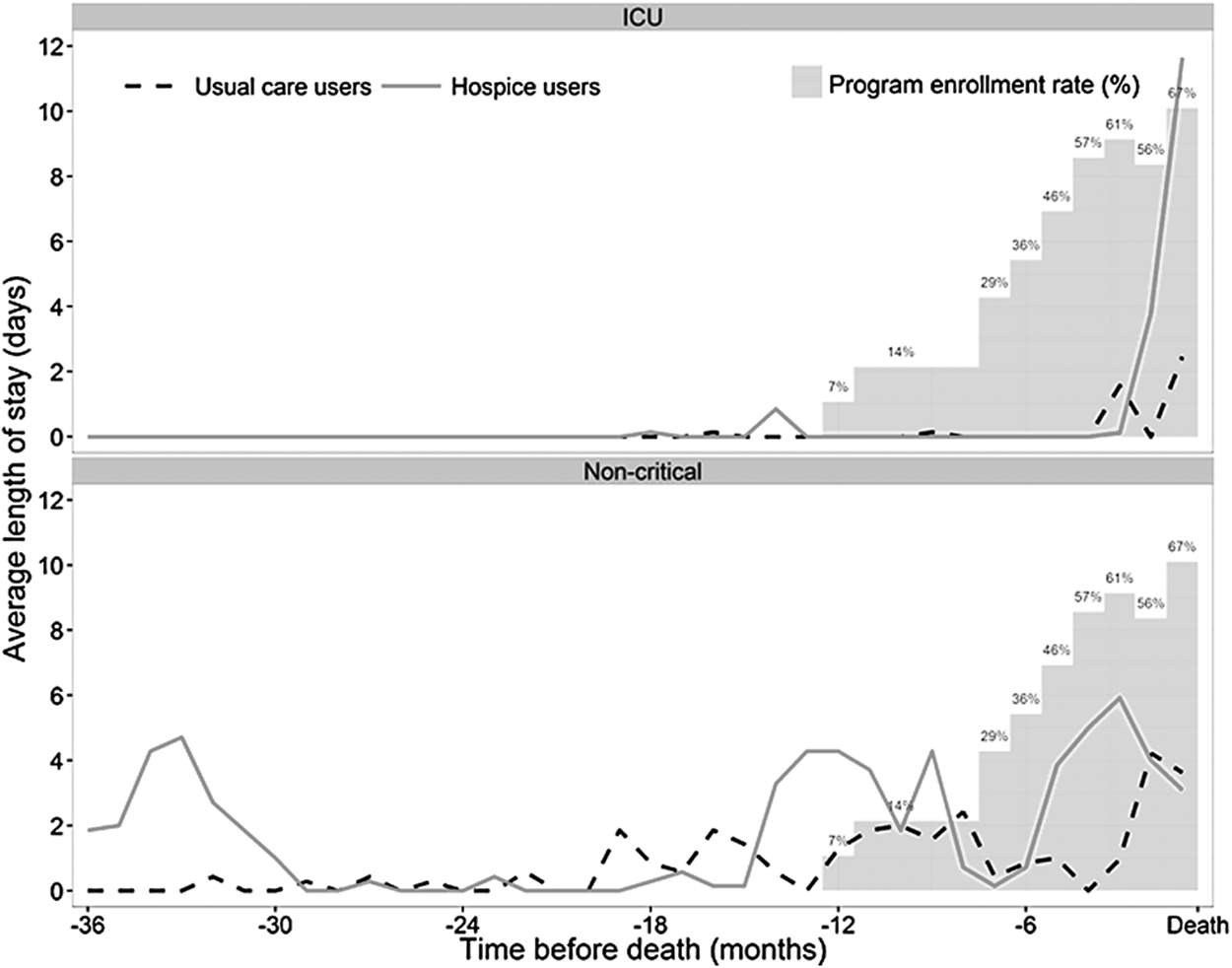
LOS per person/month at risk over time, by arm: critical and noncritical admissions.
Although the differences in LOS between groups were not statistically significant (at alpha = 0.05) in either pre- or postreferral periods, they became larger after enrollment (Table 4): median monthly difference in LOS was 1.91 days prereferral and 3.66 days postreferral. The shift in healthcare setting to hospice is evident since 60% of inpatient days were spent in hospice postreferral, more notably in the noncancer subgroup (Table 5).
Pair #78 was excluded from the prereferral period, the hospice user was a newborn enrolled in the program from birth.
LOS, length of stay; SD, standard deviation.
Last admission before death (end-of-life admission)
No significant differences were found between groups for length of end-of-life (EOL) admission or use of invasive procedures to prolong life. However, hospice users tended to have shorter EOL admission (median difference between pairs of 3.25 days), and lower absolute numbers of invasive procedures. Statistical tests on the use of procedures were not valid given the differences in LOS.
Limitations
The mean difference between pairs in monthly inpatient LOS in our sample was 0.5 days (hospice users 9.3 days vs. controls 8.8 days) with a standard deviation of 10.4 days. Among other limitations of this study, the biggest challenge was the matching process, which was limited by the naturally small size of this population (i.e., 210–250 deaths/year in BC*), 8 the lack of a national database of palliative care users, and lack of data from children with home deaths. There are two plausible reasons for the low number of comparable pairs: children may have died from the same diseases, but at different ages across groups; or children may have died at approximately the same age in both groups, but from different diseases. A population database is required to address these challenges.
Discussion
Acknowledging the sample size limitation, this study is the first of its kind to provide information on the variability of outcomes among children who died from LTCs with a broader comparative approach to inpatient healthcare utilization. These preliminary findings suggest that the pediatric population referred to a palliative care program may be different than those who died under usual care (even before enrollment), presenting with more intense resource needs, especially critical care nearing death. Despite the need for critical care, a relevant shift in setting from hospital to hospice for healthcare utilization was observed, most evident in the noncancer subgroup. These findings align with the only previously published pre–post study that measured hospice utilization and showed palliative care users to have longer LOS than those under usual care. 5 Given the acuity level of admissions and the fact that these children did not have a home death, hospice users may have occupied hospital beds, including intensive care unit beds, in the absence of the hospice. Future studies that include severity of disease and the starting point from which children should have been referred to a palliative care program can shed light on the systematic differences between these children. Determining a ground zero for palliative care referral is fundamental to allow for unbiased comparison between groups and detangle possible confounding factors.
Conclusions
Our results show a shift in healthcare setting utilization among palliative care users rather than a decrease in resource utilization suggested by the majority of existing literature in this field that do not include measurement of resource utilization in hospices. It allows a more comprehensive understanding of how these programs can impact resource utilization across various healthcare settings.
Enhanced timing of shifts to hospice-based programs may offer a more holistic approach to care for families earlier in the disease trajectory and relieve hospital resources to meet other demands within the pediatric population, shifting the conversation to more appropriate resource allocation for both palliative and nonpalliative populations.
Footnotes
Acknowledgments
The authors are grateful for the contribution of Peijun Sang, consultant from UBC Department of Statistics, who supported the statistical analysis planning; Karyn Epp for providing assistance from her PHSA team with data retrieval; and Dr. Rod Rassekh and Ms. Cindy Stutzer from the division of Pediatric Hematology/Oncology/BMT at BC Children's Hospital for the insight and assistance with the matching process for the oncology cases. This article did not receive funding and it was originated from a master thesis for the MSc degree in the School of Population and Public Health at the University of British Columbia. T.C. was funded by an External Graduate Award for students in the Health Economics Concentration as well as a UBC International Tuition Award and UBC Faculty of Medicine Award.
Author Disclosure Statement
No competing financial interests exist.