
Abstract
Abstract
Background:
Palliative care has been recommended as a means to assist patients with idiopathic pulmonary fibrosis (IPF) in managing symptom burden and advanced care planning. Timing of referral is important because although most patients display a gradually progressive course, a minority experience acute deterioration, an outcome associated with high mortality.
Aim:
To describe characteristics of IPF patients referred to a specialty lung disease center over a 10-year period who experienced acute deterioration and subsequent intensive care unit (ICU) admission, including frequency and timing of referral to palliative care.
Design:
Retrospective review.
Setting/Participants:
We identified 106 patients admitted to the ICU with acute deterioration due to a respiratory or nonrespiratory cause. Variables examined included demographics, date of first center visit, forced vital capacity, diffusing capacity of the lung for carbon monoxide (DLCO), and palliative care referral.
Results:
ICU admission occurred early (median 9.5 months) and, for 34%, within four months of their first center visit. For nearly one-half of these patients, ICU admission occurred before their third clinic visit. Only 4 (3.8%) patients received a palliative care referral before ICU admission. The majority (77%) died during ICU admission. With exception of the relationship between DLCO% predicted at first visit and time to ICU admission (r = 0.32, p = 0.005), no variables identified those most likely to experience acute deterioration.
Conclusion:
Due to high mortality associated with ICU admission, patients and families should be informed about palliative care early following diagnosis of IPF.
Introduction
I
Given high symptom burden and absence of curative therapy, discussion of palliative care is recommended early for patients with advanced lung disease to improve symptom management and facilitate advanced care planning.8–10 However, despite an extensive body of literature that supports the benefits of early palliative care, patients with advanced lung disease receive palliative care less frequently than those with cancer, heart failure, dementia, or end-stage renal disease.11,12 From a study that examined medical record documentation of palliative care in patients admitted to 15 hospitals, Brown et al. 13 reported that compared with patients with metastatic cancer, patients with interstitial lung disease, including those with IPF, and chronic obstructive pulmonary disease who died in an intensive care unit (ICU) were less likely to have documentation of a discussion of their prognosis or a do-not-resuscitate order at the time of their death. This is concerning because the onset of acute respiratory failure in patients with IPF is associated with extremely high mortality.14–18
A recent systematic review of 22 controlled trials conducted in outpatient, acute care, and ICU settings concluded that patients at high risk of death who received advance care planning or palliative care interventions were admitted less frequently to the ICU or, if admitted, tended to have a reduced ICU length of stay. 19 This finding was consistent across the studies, despite wide variation in study type and quality. Nevertheless, although the high mortality14–18 and unpredictable disease trajectory1–4 associated with IPF are well known, our experience and that of others supports the conclusion that palliative support of IPF patients has been limited to date.8,10,13 We reasoned that exploration of the frequency of palliative care referrals and factors associated with these referrals may help explain this low referral rate.
We reviewed consecutive ICU admissions of IPF patients referred to a specialty interstitial lung disease center over a 10-year period. Our primary goal was to identify the frequency of referral of IPF patients to palliative care. In addition, we examined factors that may have influenced decision-making regarding referral.
Methods
Setting
We reviewed medical records of consecutive patients with IPF referred to the University of Pittsburgh Dorothy P. and Richard P. Simmons Center for Interstitial Lung Disease over a 10-year period. The Simmons Center, a specialty center affiliated with the University of Pittsburgh Medical Center (UPMC), annually evaluates ∼200 patients with IPF.
Sample
Using UPMC health system's data repository and specialty database, we identified 860 patients with a confirmed diagnosis of IPF whose first center visit occurred between May 2001 and December 2012. We extracted data for all patients whose care involved admission to a UPMC hospital ICU. Approval to conduct the study was obtained from the University of Pittsburgh Committee for Oversight of Research and Clinical Training Involving Decedents (CORID No. 411) as all patients included in the study were deceased. Elective admissions (lung transplant recipients and patients admitted for postprocedure observation) were excluded.
Measurements
Sociodemographic and clinical characteristics included age, gender, race, smoking history, date of first center visit, admission source, primary reason for ICU admission, transplant status, and duration of survival. Primary reason for admission was categorized as respiratory (acute deterioration, resulting in respiratory compromise) or nonrespiratory (cardiac, neurologic, gastrointestinal, etc.).
Forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO) values were extracted from the electronic data repository for the first center visit (initial entry) and subsequent recordings before ICU admission.
Gender-age-physiology (GAP) index is a validated mortality prediction model that classifies patients into three stages (I, II, III) by summing points for gender, age, and physiology (FVC, DLCO). Points are assigned for gender (0 = female, 1 = male), age (≤60 years = 0, 61–65 years = 1, >65 years = 2), FVC% predicted (>75% = 0, 50–75% = 1, <50 = 2), and DLCO% predicted (>55% = 0, 36–55% = 1, ≤35% = 2). For DLCO, a score of 3 is assigned if symptoms prohibit ability to perform the test. The total possible score (range 0–8) is used to classify patients as stage I (0–3 points), stage II (4–5 points), or stage III (6–8 points). GAP stage III has the highest mortality risk. 20 The model was developed and validated using retrospective data from three large geographically distinct cohorts of patients with IPF. Model discrimination was assessed by the c-index, and calibration was assessed by comparing predicted and observed mortality. The model successfully identified three stages of disease with one-year mortality of 6%, 16%, and 39%, respectively. 20
Time from first center visit to ICU admission and from ICU admission to death was computed by determining the interval between these dates. Data were restricted to the initial ICU admission if multiple ICU admissions occurred.
Palliative care referral was defined as a formal request for consultation documented in the electronic data repository. Clinical characteristics associated with this referral were obtained from electronic records.
Transplant status was categorized as listed candidate, referred/waiting evaluation, deferred postevaluation, declined as candidate, or not referred at the time of ICU admission.
Data analysis
Data analysis was conducted using SAS software. Descriptive statistics (mean, percentile) were used to summarize demographic and medical condition data. When data were not normally distributed, median and interquartile range were used. To test for differences between patients admitted for a respiratory versus nonrespiratory condition and ICU survivors versus nonsurvivors, t-tests were used for continuous variables and chi-square for noncontinuous variables when data were normally distributed. The Mann-Whitney U test was used when data were not normally distributed. Spearman's rho was used to determine the correlation between time (months) from first visit to ICU admission. All p < 0.05 values were considered statistically significant.
Results
Of the 860 patients evaluated during the study period, 297 (35%) were admitted to an ICU. After excluding lung transplant recipients (n = 134), admissions for postprocedure observation (n = 48), and patients with missing data (n = 9), 106 (12%) patients remained for final analysis (Fig. 1).
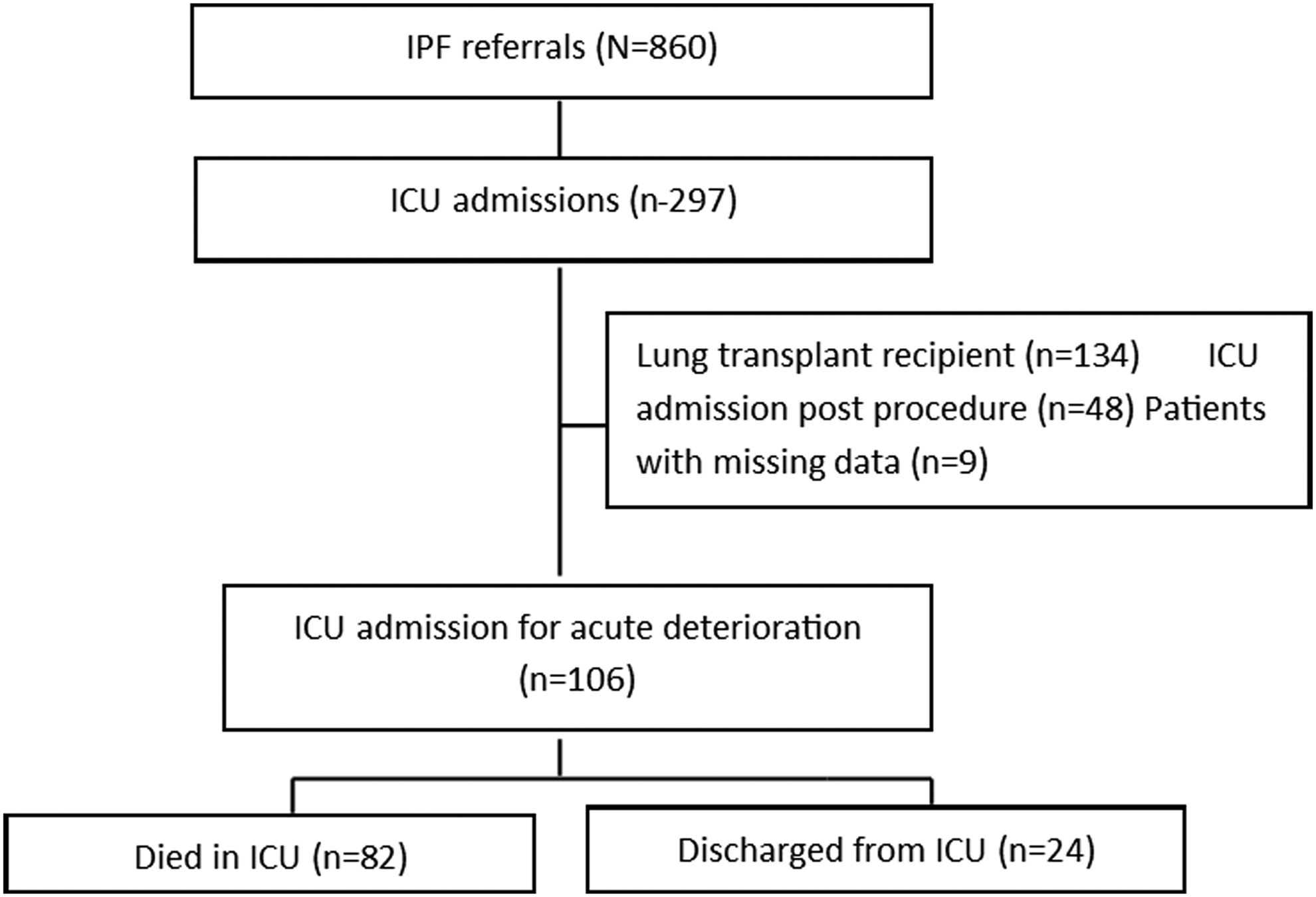
Subject flow chart.
Mean (SD) age of patients at their first center visit was 68.0 ± 9.8 years (Table 1). The majority were male (71%), Caucasian (89%), and former smokers (77%). Median pulmonary function values reflected moderate disease severity; however, there was wide variability in these measures. Median FVC was 62% predicted (IQR range 52–74%) and median DLCO 39% predicted (IQR range 32–57%). A minority was listed as a transplant candidate (n = 11; 10.3%) or referred/waiting for evaluation (n = 20; 18%). None of these patients received a transplant. All listed candidates and the majority (15/17) patients who were referred/waiting evaluation died before ICU discharge.
Results are median (interquartile range) or mean ± SD unless otherwise specified.
IPF, idiopathic pulmonary fibrosis; ICU, intensive care unit; FVC, forced vital capacity; DLCO, diffusing capacity of the lung for carbon monoxide; ED, emergency department.
During the study period, 89 (84%) patients were admitted with a primary diagnosis of acute respiratory deterioration and the remainder for a nonrespiratory diagnosis. Nonrespiratory causes included cardiovascular (n = 6), neurologic (n = 4), gastrointestinal (n = 1), and other conditions (n = 6). When comparisons were made between patients admitted for a respiratory and nonrespiratory diagnosis, there were significant differences in age and duration of survival. Compared with patients with a nonrespiratory diagnosis, patients admitted with a respiratory diagnosis were younger (67 ± 10.1 vs. 72.1 ± 6.3 years, p = 0.04) and died in a shorter interval after ICU admission (1.02 ± 2.31 vs. 3.25 ± 10.43 months, p < 0.001). FVC tended to be lower for patients admitted for a respiratory diagnosis; however, the difference did not reach statistical significance (p = 0.05).
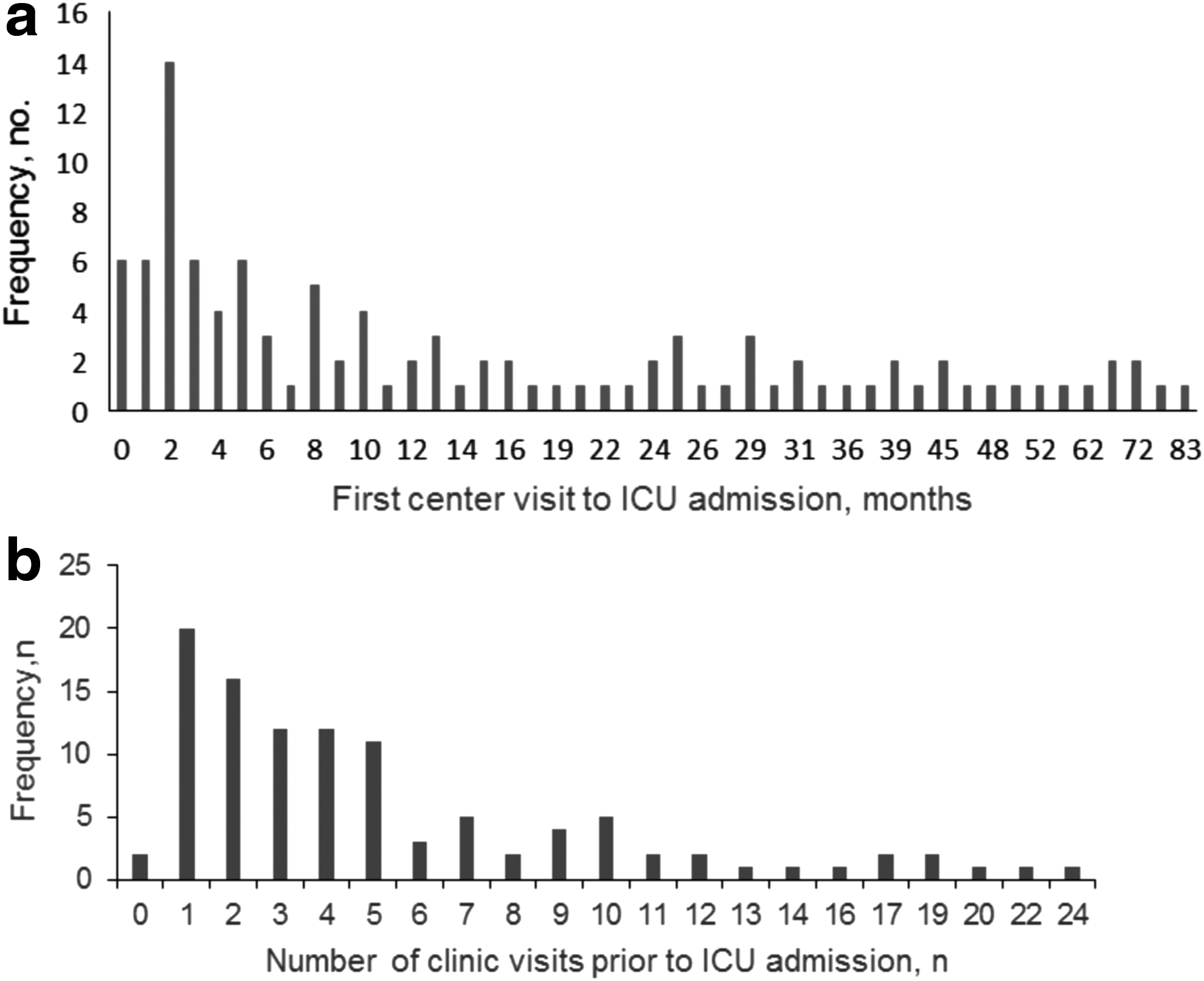
Median time from the first center visit to ICU admission was 9.5 months (range 0–83 months) (Fig. 2a). The majority of patients (n = 79, 75%) were admitted from the emergency department; the remainder were direct ICU admissions from another facility or transferred from a lower acuity unit. ICU admission occurred relatively soon following referral for a substantial number of patients: 36% were admitted before their second clinic visit and 47% before their third clinic visit (Fig. 2b).
Few patients (n = 27; 25%) had a formal palliative care referral before ICU admission. Of these 27 patients, 23 patients received a palliative care referral during their ICU stay (Fig. 3). Reasons for palliative care referral included worsening of disease course, symptom management, and requested by patient/family member.
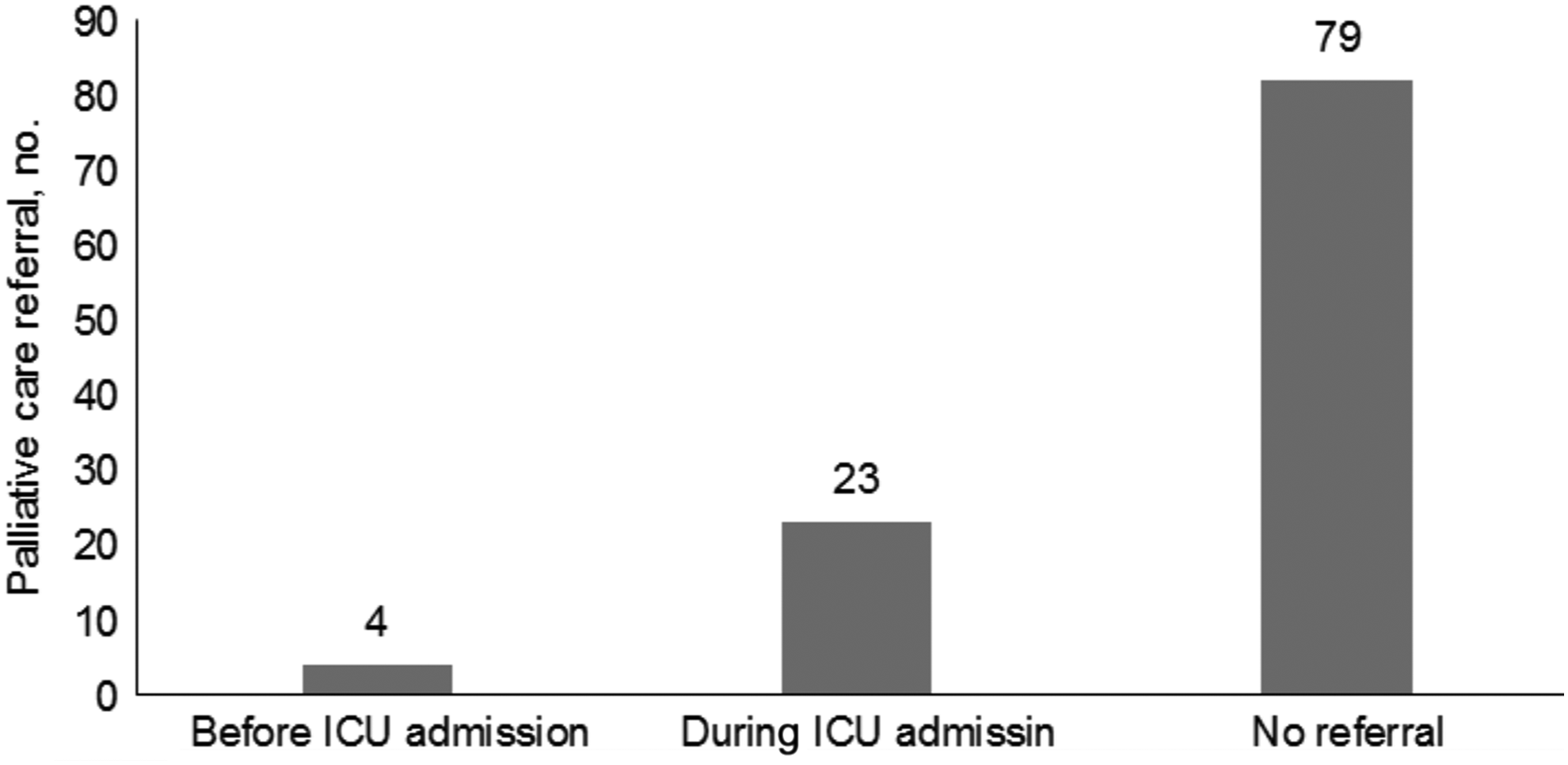
Palliative Care Referrals. Of the 106 patients, 27 (25%) had a formal palliative care referral. Four of these referrals occurred before ICU admission.
To identify factors that might influence survival, we compared demographic characteristics (age, gender), pulmonary function values (FVC, DLCO), and GAP score in survivors and nonsurvivors (Table 2). Thirteen patients who did not have complete pulmonary function data were excluded from this analysis. There were no differences in age, gender, first visit FVC% predicted, first visit DLCO% predicted, GAP score, or other pulmonary function-related variables. Over half (61%) were classified as GAP stage II and the remainder as GAP stage I (21%) or GAP stage III (18%). Both the most recent FVC% predicted (IQR 40–81) and DLCO% predicted (IQR 24–51) before ICU admission exhibited wide variability. There was a significant positive relationship between DLCO% predicted at first visit and time to ICU admission (Spearman rho = 0.32, p = 0.005) and a marginally significant relationship for FVC% predicted at first visit (Spearman rho = 0.20, p = 0.054), suggesting higher risk for ICU admission in those with worse lung function.
GAP, gender, age, physiology.
Results are in median (interquartile range) unless otherwise specified.
Excludes patients who did not have complete pulmonary function data.
If DLCO was unmeasurable, three points were assigned when computing GAP score.
Discussion
We have previously reported that patients with IPF, a disease without cure for those who are not candidates for lung transplant, die at an alarmingly high rate in the hospital. 10 In this study, we found that a small but significant minority of IPF patients was admitted to the ICU very soon after a first visit to a specialty lung center. The rapid course for this subgroup of IPF patients poses a significant challenge to the clinician to capture the opportunity to introduce palliative care to patients who need it most without diminishing the hope of those who may be desperate for the positive messages that a specialty lung center can provide. Adding to this challenge, before ICU admission, almost half of these referrals had been seen for two visits.
The incidence of IPF increases with older age, with presentation typically occurring in the sixth and seventh decades.1,2 Men are more commonly diagnosed with having IPF than women and the majority of patients have a history of cigarette smoking, consistent with our sample.1,2 Although a slow progressive decline in pulmonary function is more common, some patients experience rapid progression from the onset of diagnosis.4,21 The potential for rapid progression may explain the high percentage of patients admitted from the emergency department within a relatively short interval after center referral as well as the small number listed for transplant or awaiting evaluation. Patients admitted for a respiratory diagnosis were younger, but survived for a shorter interval following ICU admission, suggesting a rapid decline.
We are unaware of prior studies that report risk for ICU admission, the timeline between referral to a specialty lung center and ICU admission, or the number of center visits preceding this outcome among a large cohort of patients with IPF. In our study, ICU admission occurred early (median 9.5 months) and, for almost half of these patients, ICU admission occurred before their third clinic visit. Can we predict which patients are going to suffer rapid deterioration at a first or second visit? Several challenges are associated with this goal. First, symptoms at the onset of IPF are subtle, which delays confirmation of the diagnosis. 4 We previously reported that patients with IPF experience an average of a two-year delay between onset of symptoms and referral to a specialty lung center, 10 a finding consistent with the delay reported by others.22,23 Second, the disease course is highly variable and studies, to date, have been unsuccessful in identifying reliable predictors of escalation.24–26 In our cohort, we found that DLCO (% predicted) was significantly associated with rapid admission to the hospital. DLCO has previously been implicated in IPF as a factor influencing prognosis and, based on our findings, may serve to identify patients at higher risk of symptom escalation. Further study will be necessary to investigate this potential.
Prior studies have reported high mortality associated with the need for ventilatory support in patients with IPF.14–18 Using data pooled from nine studies, Mallick 15 reported an overall mortality of 87% in 135 patients who managed with mechanical ventilation following ICU admission. In those discharged from the ICU, three-month mortality was 94%. These findings are, disappointingly, essentially the same as more recent reports. Gaudry et al. 17 reported mortality of 74% during ICU admission from a series of 27 patients and, with the exception of patients who received a lung transplant, only one survivor at 12 months. From a series of 18 patients initially managed with noninvasive ventilation, Vianello et al. 16 reported that 8 (44%) patients survived to ICU discharge. There were, however, no survivors at one year. Consistent with these findings, in the present study, mortality was high during ICU admission and for those discharged from the ICU, survival was relatively brief, an outcome that reflects the progressive nature of the disease and absence of curative treatment.
Given the lack of curative treatment and inability to predict disease progression, we suggest that patients diagnosed with having IPF would benefit from clinician-initiated discussion of palliative care early following their diagnosis.27,28 Unfortunately, due to reasons related to age, comorbidities, and organ availability, the vast majority of IPF patients will not be accepted as transplant candidates and will, therefore, follow a fatal prognosis. In fact, we discovered that only four patients had a formal palliative care referral at the time of ICU admission. When referral does occur, it is often late in the course of the disease. We previously reported in a study of 277 IPF patients that time of referral was highly correlated with time of death. 10 Our findings were disappointingly consistent with others reporting delayed referral in patients with advanced lung diseases.11–13
In contrast to the extensive literature that has explored benefits of palliative care in patients with cancer, few studies have examined factors that influence decisions to provide palliative care referral in patients with advanced lung disease.28–30 Many reasons have been proposed to explain timing of referral. These include the prognostic uncertainty of IPF, the fear of diminishing hope, clinician discomfort with palliative care discussions, and limited patient and caregiver understanding of potential benefits of palliative care.9–12,31 We suspect that a primary obstacle is fear that referral will diminish hope. Findings from patients diagnosed with having cancer and other terminal conditions, however, suggest this concern may be unfounded. Patients newly diagnosed with metastatic lung cancer assigned to early palliative care reported better quality of life, fewer depressive symptoms, and, despite receiving less aggressive end-of-life care, experienced longer survival. 32 Coulourides Kogan et al. 33 reported that patients with a terminal illness, when informed of this consequence during a palliative care consultation, did not experience a loss of hope, but instead reframed goals. This observation may relate to content of palliative care discussions. Yoong et al. 34 analyzed content of discussions during palliative care consultations and patient visits with their oncologist. During palliative care consultations, the initial visit focused on building rapport and understanding prognosis and later discussions on resuscitation preferences. This focus was also a part of discussions led by the oncologist, but palliative care discussions were more likely to emphasize psychosocial elements, such as coping, versus treatment and management of complications.
Notably, the receptiveness of IPF with patients to palliative care is unknown. The extensive literature that supports benefits of palliative care has largely involved patients with metastatic cancer. 32 We are unaware of any randomized controlled trials that have tested the benefit of early referral to palliative care, either through a formalized referral or provided as part of subspecialty care, for patients with IPF. Such evidence would seem highly important to clarify potential benefits and optimal timing of referral.
Our study has several limitations. The study used a retrospective design, which limited data to that included in the health system data repository and center database. We limited our definition of palliative care to documentation of a formal consultation in the health system data repository. This approach may have missed conversations that were not documented. It is possible that healthcare providers provided similar information and support, absent a formal referral. Thus, the provision of palliative care or palliative care consults might be underreported. Finally, our study involved one specialty center. Outcomes of patients managed at other centers or not referred may differ from our findings. However, our sample was relatively large and included all IPF patients referred over a 10-year interval. Our finding that DLCO% predicted may serve as a means of identifying patients at greatest risk for ICU admission is noteworthy and deserves further study.
Conclusion
While only a minority of IPF patients referred to our specialty center were admitted to an ICU, those admitted to the ICU experienced rapid deterioration and very high mortality. We found that a small fraction of these patients had a formal palliative care referral at the time of ICU admission. Our findings identify a critical gap in the care of patients with IPF. We suggest that introduction of palliative care should occur early following diagnosis. Future studies are needed to test ways to promote earlier introduction and address specific needs of this patient population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.