
Abstract
Abstract
Background:
Advance care planning (ACP) discussions often occur in the inpatient setting when patients are too ill to participate in decision making. Although the outpatient setting is the preferred time to begin these discussions, few physicians do so in practice. Many internal medicine (IM) residents report inadequate training as a barrier to having outpatient ACP discussions.
Objective:
To assess whether a novel curriculum entitled Goals of Care Ambulatory Resident Education (GOCARE) improved resident physicians' understanding of and preparedness for conducting ACP discussions in the outpatient setting.
Design:
The curriculum was delivered over four weekly three-hour small group sessions to IM residents. Each session included didactics, a demonstration of skills, and a simulated patient communication laboratory that emphasized deliberate practice.
Setting/Subjects:
IM residents from an urban, academic ambulatory care practice.
Measurements:
Impact of the intervention was evaluated using a retrospective pre–post design. Residents completed surveys immediately after the course and six months later.
Results:
Forty-two residents participated in the curriculum and 95% completed the postcourse survey. Residents' self-rated level of preparedness increased for ACP discussions overall (4.0 pre vs. 5.2 post on 7-point Likert scale) and for communication steps involved in ACP (p < 0.001). Fifty-nine percent of participants completed the six-month follow-up survey. Residents' self-rated preparedness to engage in outpatient ACP discussions remained high (4.5 pre vs. 5.5 post at six months p < 0.001). Residents also reported increased use of ACP communication skills (p < 0.001) six months later.
Conclusions:
The GOCARE curriculum provides an alternative model of communication training that can be integrated into residency training and improve residents' skills in outpatient ACP discussions.
Background
P
Although evidence suggests that patients are willing and eager to participate in ACP discussions and that advance directive (AD) completion has recently increased for older adults, less than 40% of patients engage in ACP discussions.2,12,13 Several physician barriers to outpatient ACP discussions have been identified. These include lack of time, discomfort in communicating the topic of ACP, lack of training, and the perception that patients are reluctant or fearful of discussing ACP with their physicians14–16
Residency is a critical time for learning ACP skills, as medical residents have the basic clinical understanding of serious illness and its impact on patients' lives, but have not yet crystallized habits in clinical practices. Prior resident training curricula have primarily focused on delivering bad news, discussing end-of-life care, and determining code status in the hospital setting. These do not address the particular challenges of outpatient ACP discussions.17–24
With the exception of a recent study, 25 training for outpatient discussions have primarily focused on completing ADs, which is only one step in the complex ACP process.17,26 Often, ADs indicate wishes for specific life-sustaining treatments, but exclude the rationale for these desires and patient values. ACP in the outpatient setting, therefore, should be a patient-centered process that involves ongoing discussions of patients' values and goals in the context of changes to their health. It requires skills to engage both patients and surrogate decision-makers in an empathic and time-efficient manner.
To improve resident training in outpatient ACP discussions, we developed a novel curriculum entitled Goals of Care Ambulatory Resident Education (GOCARE) using a framework that prepares physicians, patients, and surrogates to make future medical decisions in alignment with patients' goals and values.27,28 The curriculum aims to improve resident physicians' understanding of and comfort with ACP discussions and improve the frequency with which they engage in these conversations. For this prototype study, we evaluated the impact of this curriculum on residents' confidence and willingness to engage in outpatient ACP discussions.
Methods
Intervention
The GOCARE curriculum was developed after conducting a focus group with internal medicine (IM) residents to determine communication training needs, a literature review of ACP communication strategies, and consultation with content experts. The instructional method was adapted from previously validated communication training courses that have shown observable improvement in communication skills for oncology, geriatrics, and palliative care fellows.29,30
The curriculum was delivered over four weekly three-hour small-group sessions of 6–9 residents. Each group was facilitated by two faculty members who were trained in teaching communication skills. Each session included brief didactics, a demonstration of skills, and a communication laboratory that emphasized deliberate practice (Table 1). Didactics covered steps in a patient-centered ACP framework informed by Respecting Choices, 31 the Serious Illness Conversation checklist, 32 and Prepareforyourcare.org 33
ACP, advance care planning; COPD, chronic obstructive pulmonary disease; GOCARE, Goals of Care Ambulatory Resident Education.
The framework included the following: (1) Asking permission to discuss ACP; (2) Identifying and involving a healthcare proxy or surrogate decision-maker; (3) Clarifying patient and surrogate understanding of the patient's current health status and prognosis; (4) Exploring patient's goals and values in the context of the illness; and (5) Matching the care plan to the patient's goals and priorities. We also taught specific communication skills that are useful in the context of ACP conversations, including “NURSE” statements, 34 Ask-Tell-Ask, 35 and “VALUES.” “VALUES” (Fig. 1) is a new mnemonic we developed adopting or modifying questions from the resources above31–33 to teach residents different ways to elicit goals from patients. This mnemonic differs from VALUE, described in the ICU palliative care literature, 36 that assists ICU clinicians to remember effective communication strategies when speaking to patients' families.
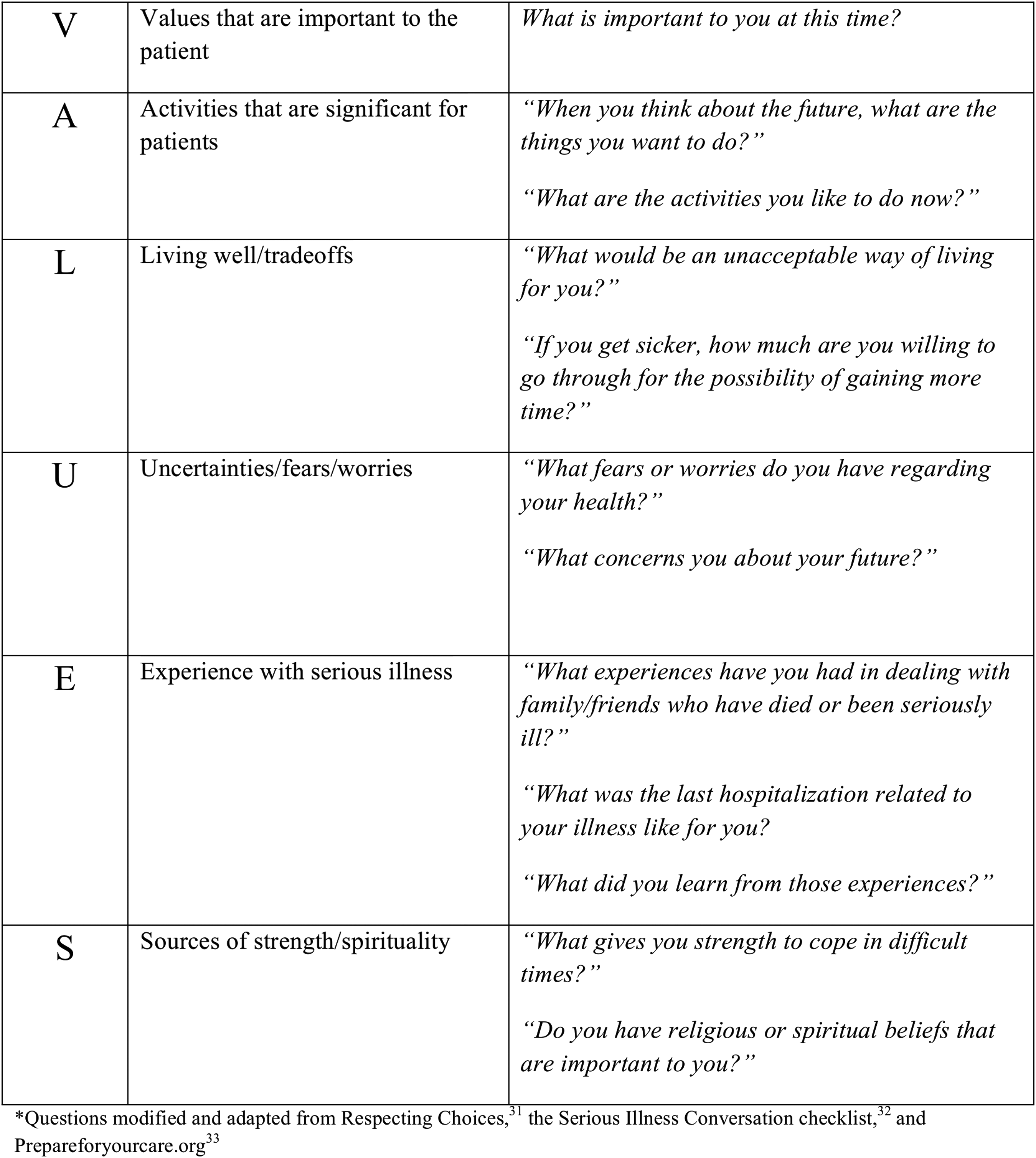
VALUES Mnemonic. Questions modified and adapted from Respecting Choices, 31 the Serious Illness Conversation checklist, 32 and Prepareforyourcare.org 33
The course also emphasized the involvement of surrogate decision-makers in the discussions and communication with other medical providers involved in patients' care. Knowledge areas covered in the course included hospice care, legal issues regarding life-sustaining treatment decisions, and proper documentation of ACP discussions in the medical record. During the communication laboratory, residents practiced communication skills with both a trained simulated patient and family member, received immediate feedback from the group, and reflected on their main “take-home points” after each skill practice. Two evolving outpatient cases were used for skill practice; the first case centered on a patient with progressive chronic obstructive pulmonary disease and the second involved discussions with the daughter of a patient who had progressive dementia.
Over the course of the four weeks, residents were tasked with identifying five patients with a serious illness from their continuity clinic panel to engage in ACP discussions and to schedule visits with at least two of these patients. During the first of these visits, the focus was to get buy-in to discuss ACP and identify a healthcare proxy. In the second visit, the focus was to clarify the patient's understanding of disease prognosis, explore goals and values, and document the conversation. The electronic medical record (EMR) was reconfigured to facilitate ACP documentation and retrieval. Residents shared reflections on these visits with their small groups during the course.
Subjects
All 42 second-year IM residents participated in the GOCARE curriculum as part of their four-week ambulatory block from January to June 2013 at an urban, academic ambulatory care practice.
Measurements
We used a retrospective pre–post survey that was administered on the last day of the course to assess residents' self-rated attitudes, skills, and behaviors regarding outpatient ACP discussions. Items in our survey were modeled after a questionnaire used to evaluate outcomes of a communication skill workshop for geriatrics and palliative care fellows. 30 It included residents' retrospective self-assessment of their level of preparedness to perform several ACP communication steps in the outpatient setting before and after GOCARE. This was measured on a 7-point Likert-type scale, modeled after reportable milestones of the Accreditation Council for Graduate Medical Education (ACGME). 37 It also assessed the willingness of residents to engage in ACP conversations in the outpatient setting before and after GOCARE.
In addition, residents were asked to list two “important lessons” learned from GOCARE that they believe will influence their future conduct of ACP conversations in the outpatient setting. They were also asked to rate the perceived value of GOCARE against other curricula in the residency program. Although GOCARE was targeted for outpatient ACP skills, the postcourse survey also included similar reflections on self-preparedness for the inpatient setting to test the hypothesis that the skills learned would also help residents feel more prepared for ACP discussions during inpatient rotations. Demographics and baseline information, including previous communication skills and palliative care training and prior experience with outpatient ACP conversations, were also collected.
To determine whether residents' perception changed over time, a six-month follow-up survey was administered through email. Using a retrospective pre–post design, this survey reassessed residents' preparedness to discuss specific ACP steps. It did not, however, differentiate between the outpatient and inpatient settings to keep the survey length short and increase participation. The survey did ask about overall preparedness for ACP discussions specifically for the outpatient setting. In addition, residents were asked to report how often they used communication skills such as “Ask-Tell-Ask” and “NURSE” during patient encounters before and six months after the course. This was evaluated on a 5-point scale of Never, Rarely, Sometimes, Often, and Always.
The surveys were voluntary and anonymous. Individual identifying information was not collected or recorded. All course surveys were chosen to be retrospective in design to ensure resident anonymity and to correct for response-shift effect. 38 Our study was exempted from the institutional review board at our institution. We used descriptive statistics for baseline characteristics, and a paired-sample t test for survey analysis of the retrospective pre and post responses. Statistical significance was defined as p < 0.05. We used SPSS version 21 (IBM SPSS). A chart review was conducted after completion of GOCARE to determine whether residents completed their assigned ACP visits with patients and documented it in the EMR.
Results
Forty-two second-year IM residents participated in the GOCARE curriculum. Ninety-five percent of the participants completed the postcourse survey, while 59% (n = 25) completed the six-month follow-up survey. Baseline characteristics are presented in Table 2. Approximately 40% of residents reported prior communication skill training and 34% reported some form of palliative care training during medical school or residency. Only three residents reported engaging in five or more outpatient ACP discussions in the past year, discussions that could have included healthcare proxy, code status, and/or goals of care discussions.
At the completion of GOCARE, there was a statistically significant increase in residents' self-rated preparedness for ACP discussions in both the inpatient and outpatient settings (Table 3). The greatest change was seen in the following ACP discussion steps: choosing an appropriate healthcare proxy, giving bad news, eliciting goals of care, and discussions of treatment options, including comfort care in the outpatient setting. In addition, residents reported higher overall preparedness for engaging in ACP discussions in the inpatient setting compared to the outpatient setting at baseline (5.23 vs 4.00 on a 7-point Likert scale), as well as after the completion of GOCARE (6.28 vs 5.20). Upon chart review immediately after the completion of GOCARE, 40 residents (95%) documented in the EMR at least one ACP visit with 10 of these residents (20%) engaging in more than the required number of visits (>2 visits).
p < 0.001 for all comparisons.
Scale
1. Not prepared, do not know the general principles/skills involved in the discussions.
2. Not prepared to lead a discussion by myself, but aware of the general principles/skills.
3. Somewhat prepared, know the basics, and have trouble starting and moving conversations forward.
4. Moderately prepared, I can start a discussion but feel that I get “stuck” easily.
5. Adequately prepared, but I have discomfort during challenging situations.
6. Pretty well prepared, although I can benefit from additional experience.
7. Extremely well prepared, at an “expert” level, and I can teach others.
Residents' self-reported preparedness also was increased at the six-month follow-up. Specifically, residents reported that they were more prepared after GOCARE in using the ACP communication steps for inpatient and outpatient clinical settings and engaging in ACP discussions in the outpatient setting (Table 3). Residents also reported a statistically significant increase in the use of communication skills taught in the course such as “Ask-Tell-Ask” and “NURSE” statements in clinical encounters (Table 4).
p < 0.001 for all comparisons.
The GOCARE curriculum was rated as either “very useful” or “extremely useful” by over 60% of the residents. Over two-thirds of the residents rated GOCARE as “just as valuable” or “more valuable” compared to the highest rated curricula in the residency program, including a course on evidence based medicine 39 and a course on teaching skills. 40 The most cited “important lessons” learned from the course were “eliciting the patient's goals” and recognizing the importance of “initiating advanced care planning in the outpatient setting.”
Discussions
ACP is a process that involves communication skills beyond completing AD forms. Such discussions should begin in the outpatient setting when patients are able to participate in decision making and involve surrogate decision-makers. We developed this curriculum to teach the components of ACP using didactics, skill demonstration, and deliberate practice with role play and real-time patient encounters. We evaluated the impact of the curriculum on residents' self-rated preparedness and willingness to engage in these discussions immediately after the course and six months later.
The results demonstrate that residents had an increase in self-rated preparedness to discuss ACP and used the communication steps involved both immediately post GOCARE and six months later. Particularly, residents continued to feel more prepared to engage in ACP discussions in the outpatient setting and focus on exploring patients' goals and values. Residents also reported an increase in use of communication skills such as “Ask-Tell-Ask” and “NURSE” statements six months later. These findings suggest that GOCARE improved residents' confidence discussing ACP with patients and their families and residents readily used communication skills learned in clinical practice. It also suggests the importance of deliberate practice, use of reflection, and application in real clinical encounters in teaching communication skills that have lasting impact on learners.
Of note, 95% of residents completed at least one ACP discussion in the outpatient setting during GOCARE. Incorporation of deliberate and reflective practice in other communication training programs has produced similar results.29,30 Unlike GOCARE, however, most of these communication courses are typically designed as multiday intensive retreats, which are rarely feasible for residency programs. Similar to Chan et al., 25 GOCARE uses deliberate practice and real patient encounters to help residents integrate skills learned and incorporate them into daily practice. GOCARE provides an alternative model that can be compatible with standard residency training structures.
The results of our study also highlight that IM residents felt more prepared to engage in ACP discussions in the inpatient setting compared to the outpatient setting and this persisted after GOCARE. This might be explained by the disproportionately larger percentage of time most residents spend on inpatient rotations where goals of care discussions seem more common and routine. This argues for the importance of ACP curricula to be focused on outpatient scenarios and ways to incorporate these skills into outpatient practices. Furthermore, our findings illustrate that an outpatient-directed curriculum can impact not only outpatient preparedness for these discussions but also translate to improved confidence with conversations in the inpatient setting.
Residents also felt GOCARE was useful to their education and that its value is comparable to the highest rated courses in the residency. GOCARE fulfills an important mandate from the ACGME and the Institute of Medicine that residents develop competency in effective communication skills that promote shared decision making with patients and families so that patients receive care that reflects what matters most to them.37,41,42
There were some limitations in our study. The study was conducted at one institution and results may not be generalizable across training programs. Other limitations were the use of nonvalidated retrospective pre/post surveys and the relatively low response rate for the six-month follow-up survey which may have contributed to a selection bias. In addition, the six-month follow-up survey did not distinguish preparedness between inpatient and outpatient settings for specific ACP steps which makes it difficult to ascertain how much impact the course had on residents in each particular setting and compare with the effect immediately post course.
Nonetheless, our results suggest that our curriculum prototype can lead to improvement in residents' level of preparedness and willingness to engage in both inpatient and outpatient ACP discussions and that these effects can be sustained over time. Future research for GOCARE will be to develop an objective method of assessing change in ACP communication skills through direct observation with real or simulated patient encounters, measure the occurrence and quality of documented ACP discussions in the EMR, and assess the degree to which patients with documented ACP discussions have wishes for care honored subsequent to their loss of decisional capacity.
Footnotes
Acknowledgments
Thank you to support from the Mount Sinai Department of General Internal Medicine and the Mount Sinai Auxiliary Board. The authors also thank Anthony Back, Robert Arnold, and Amy Kelley for assisting with the curriculum development of the program.
Author Disclosure Statement
No competing financial interests exist.